
Abstract
Aims: The aim of the present study was to re-establish a set of normative data for serum thymidine kinase 1 (STK1) for the Chinese population. Methods: The study included 14,960 Chinese subjects (9586 males and 5374 females) from 20 to 79 years old. Subjects suffering from diseases that could affect STK1 levels were excluded. STK1 was measured by a sensitive chemiluminescence dot blot assay. The reference intervals were calculated using the LMS method. Results: Peak thymidine kinase 1 (TK1) serum levels were observed at 20 years of age for both genders. After the age of 20 years, serum TK1 levels decreased slowly from 0.51 to 0.36 pM, reaching a plateau to a mean of 0.35 pM in late adulthood. The mean pretreatment STK1 Z-scores in patients with solid malignant tumors obtained from related studies for cancers were 0.01 ± 0.99 (males, −0.07 ± 0.97; females, 0.09 ± 1.02). Conclusions: The present study established age- and gender-specific normative STK1 data for the Chinese population and showed the utility of these references for screening patients with solid malignant tumors.
Introduction
T
Recent studies have suggested that patients with an elevated STK1 (risk cutoff value >2.0 pM) showed a significantly higher frequency of obesity, fatty liver, and HBV infections, as well as various types of moderate/severe premalignancies, conditions that increase the risk of developing malignancies over the years(Chen et al., 2011; Cao et al., 2014). Serum TK1 levels are known to vary with age, gender, and physiological condition (Chen et al., 2011; Cao et al., 2014). Therefore, it is necessary to establish normative STK1 data specifically for the Chinese population.
The STK1 assay in large-scale health screening studies was initiated in China since 2006, the results of which demonstrated that it had the potential to be used for identifying individuals with malignancies in a group of healthy people (Chen et al., 2008, 2011; Huang et al., 2011). We previously reported population-based reference ranges of serum TK1 for Chinese based on the data from 11,880 healthy adults in 2008 (Chen et al., 2008). The reference was widely used and acceptable in clinical investigation (Pan et al., 2010; Huang et al., 2011).
However, as the reference value was a crude cutoff point, it did not properly reflect data variation among adults with different age and gender. STK1 was applicated in clinical oncology based on case-control trials or routine clinical settings as a proliferation biomarker, and the control group usually comprises healthy individuals with matched gender and ages. Therefore, there is a need to establish age- and sex-specific normal ranges to increase the accuracy of diagnosis and management.
In this cross-sectional study, we reanalyzed serum TK1 levels in 14,960 Chinese adults in a health screening center of central south China to pre-establish normative data for the Chinese population aged between 20 and 79.
Materials and Methods
Study subjects
Health screening of 42,383 people (24,194 men and 18,189 women; aged 20-79 years) was performed at the Health Management Center of the Third Xiangya Hospital, Central South University in Hunan Province of China between 2013 and 2014. According to the previous studies (Chen et al., 2008; Topolcan and Holubec, 2008), we excluded subjects from medical histories who had malignancies, premalignancies, thyroid disease, liver disease (moderate/severe fatty liver, liver cirrhosis, in particular), renal disease, severe cardiac disease, moderate/severe type of hyperplasia of breast or prostate, or refractory anemia, or to be at high risk for hepatitis B, or using any medication that could affect STK1 levels such as exogenous hormone therapy, or those who were pregnant and had suffered from an acute illness, such as inflammation/virus infection within 4 weeks.
Moreover, those whose serum creatinine was elevated to more than 176.8 μM, whose alanine aminotransferase (ALT) level was threefold that of the upper normal values, or whose white blood cell (WBC) level was elevated to more than 10.0 × 109/L were also excluded. Also, obese or extremely thin subjects with a body mass index (BMI) above 28.0 kg/m2 or below 18.5 kg/m2 were also excluded from this study. The final analysis consisted of 14,960 subjects (9586 males and 5374 females).
To evaluate the efficacy of STK1 in screening for apparently healthy individuals with early solid malignant tumors, we obtained pretreatment STK1 data of subjects with solid malignant tumors from previous studies of STK1 in clinical trials or health screening (Chen et al., 2011; Cao et al., 2014). In total, 116 adults (66 males and 51 females) aged between 32 and 59 years with early solid malignant tumors according to the pathologic diagnosis with serum TK1 measurements were available for this purpose.
All participants provided informed consent before entering the study, and approval was obtained from the Human Subjects Committee at Third Xiangya Hospital, Central South University.
Data collection
The assessment of medical history, lifestyle behaviors, and medication was based on the standardized questionnaire in the medical record. Trained staff reviewed the completed questionnaires and entered the responses into a database. Anthropometric variables were measured with standard methods. BMI was computed as weight in kilograms divided by the square of height in meters. Blood samples were drawn from the antecubital vein by careful venipuncture using a 21G sterile syringe without stasis at 08:00-10:00 hours after a fasting period of 12 h. Fasting plasma glucose, serum ALT, and creatinine were measured by routine methods.
Serum TK1 concentration assay
The TK1 protein concentration was measured by an enhanced chemiluminescent (ECL) blot assay as described by the manufacturer (commercial kit; SSTK, Inc., Shenzhen, China) (Wu et al., 2003). Samples comprising 3 μL of serum were directly applied to nitrocellulose membrane in duplicate. The serum samples were probed with the anti-TK1 chicken IgY antibody raised against a peptide (residue 195-225, GQPAG PDNKE NCPVP GKPGE AVAAR KLFAPQ). The TK1 peptide was dotted at different concentrations (20, 6.6, and 2.2 pM) as an extrapolation standard. The intensities of the spots on the membrane were determined by CIS-1 imaging (SSTK, Inc.). From the intensity of the TK1 standard of known concentrations, the concentration of the serum TK1 was calculated and expressed as pM (He et al., 2005).
Statistical analyses
Descriptive statistics by gender were calculated using SPSS statistical software package version 19.0 (SPSS, Inc., Chicago, IL). Construction of the age- and gender- specific percentile curves was performed using the LMS Chartmaker Light version 2.3 software program (The Institute of Child Health, London, UK), which fit smooth centile curves to the reference data using the LMS method (Cole and Green, 1992). This method summarizes percentiles at each age based on the power of the age-specific Box-Cox power transformations used to normalize data. The final curves of the percentiles were produced by three curves representing skewness (L curve), the median (M curve), and coefficient of variation (S curve).
By using penalized likelihood, the three curves were fit as cubic splines by nonlinear regression (Cole, 1989; Cole and Green, 1992). Thus, one advantage of the LMS method is that the three curves, L, M, and S, completely summarize the measurement's distribution over the range of STK1. The sensitivity and specificity of the STK1 assay were determined by a receiver operation characteristic (ROC) analysis.
Results
Tables 1 and 2 include the serum TK1 values across the percentiles by age and gender. Tables 3 and 4 show the number of subjects and smoothed L, M, and S values by age and gender. The equation for the LMS is
Values were calculated by the LMS method with LMS Chartmaker.
LMS: L, skewness; M, median, S, coefficient of variation; TK1, thymidine kinase 1.
Values were calculated by the LMS method with LMS Chartmaker.
Values were calculated by the LMS method with LMS Chartmaker.
Values were calculated by the LMS method with LMS Chartmaker.
where Z is the Z-score that corresponds to a percentile. We presented the following STK1 percentile curves for men and women aged between 20 and 79 years: 2.5th, 5th, 15th, 25th, 50th, 75th, 85th, 95th, and 97.5th. In general, the serum TK1 concentration did not show a normal distribution, peaked at initial age of years, and declined with age until late adulthood in both men and women; as a result, we adopted the LMS method to analyze these data. Estimated percentiles as well as the variables L, M, and S required for calculation of SD scores are provided in Tables 3 and 4 for both genders in increments of 5 year.
The smoothing curves of +2SD, +SD, median, −SD, and −2SD of serum TK1 for males and females are displayed in Figure 1a and b, respectively. There was a gender difference in STK1 percentile curves: the 50th percentile curve of women was higher than men during 25 and 49 years of age, and men had higher values accordingly than women after 50 years of age. The STK1 percentile values decreased with the rise in age more conspicuously in women than in men. For men, during 20 and 49 years of age, STK1 decreased slightly or leveled off in the mid- and lower percentiles, but increased again (starting at about the age of 50 years) within the upper percentiles. Women displayed a similar pattern of age-related changes in STK1 compared to men before 50 years, but kept decreasing until 70 years of age with a slight increase within the upper percentiles.

Smoothing centile curves of +2SD, +SD, median, −SD, −2SD of serum thymidine kinase 1 values in Chinese male
To assess the validation of the constructed reference ranges in clinical use, we calculated SD scores (Z-score) of pretreatment STK1 levels in 116 adults with malignant solid tumors, whose data were obtained from previous studies of STK1 in clinical trials or health screening (Chen et al., 2011; Cao et al., 2014). The average pretreatment STK1 Z-score in subjects with malignant tumors was 0.01 ± 0.99 (males, −0.07 ± 0.97; females, 0.09 ± 1.02). The percentages of patients showing less than −2 SD were 2.59% (males, 3.03%: females, 1.96%).
The sensitivity and specificity of the STK1 assay were determined by an ROC analysis. Patients with early solid malignant tumors (n = 116) with five different types of tumors were compared to healthy people and people with various illness (n = 870) except for premalignancies or malignancies (Figure 2). The mean ROC value, including cancer patients (n = 116), was 0.91. The sensitivity and specificity at an STK1 cutoff value of 0.72 pM (used in this health screening study) based on five types of tumors were 0.793 and 0.923, respectively, with a Youden index value of 0.716.
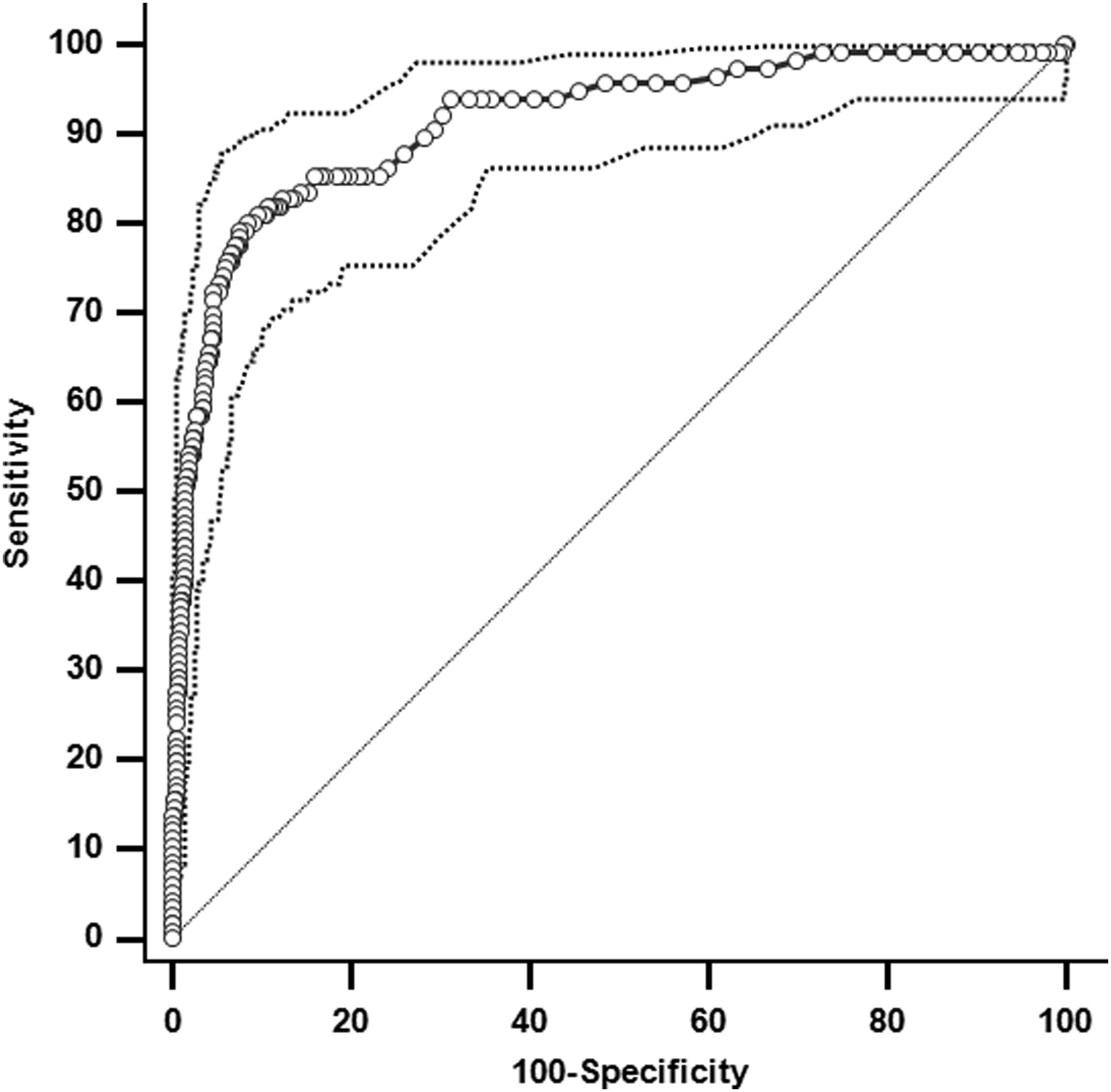
Receiver operation characteristic analysis of the chemiluminescent dot blot assay of 116 patients with five different types of malignant solid tumors and 870 healthy people and people with different types of illnesses, except for individuals with premalignant or malignant diseases.
Discussion
In the present study, we constructed the age- and gender-specific ranges for serum TK1 levels measured by ECL dot blot for a sample of 14,960 Chinese subjects aged between 20 and 79 years.
The median STK1 levels decreased slowly in young and middle aged subjects from 0.51 to 0.36 pM with a further plateau pattern during ages 50-79 years to ∼0.35 pM. Peaks of serum TK1 levels were observed at initial years in both genders. Women displayed a similar pattern of above changes in STK1 compared to men until 70 years of age with a slight increase within the upper percentiles. Szantho et al. also observed a statistically significant decline in the TK1 activity from young (18-35 years) to middle aged (36-60 years) and further on to elderly (60-86 years) healthy individuals adopting a competitive chemiluminescent immunoassay (Szantho et al., 2014). However, there are no significant differences between those relatively healthy Chinese males and females in percentage males and females in percentage of serum TK1 concentrations with age and centile compared in line with previous observations (Cao et al., 2014; Szantho et al., 2014).
The established reference intervals in the present study were constructed by the LMS method with all subjects together, and the LMS method is one of the most widely applicable approaches for age-related reference intervals (Chuchana et al., 2007; Fenton and Sauve, 2007; Silverwood and Cole, 2007; Cole, 2009; Isojima et al., 2012; Hagiwara et al., 2014; Oyhenart et al., 2014). There are several different methods to construct age-related intervals (Royston, 1991; Corish and Kennedy, 2003; Rathouz and Gao, 2009), however, it is unlikely that using a method independently would be appropriate in all circumstances with each method having both advantages and limitations.
There were several reasons for using the LMS method to construct the reference charts in the present study, although other statistical methods such as the parametric “mean and SD model” or the ROC curve analysis were used (Szantho et al., 2014). First, with the LMS method, we could easily produce convincing centile curves even when the skewness of data changed with age (Moussa, 2002). The serum TK1 concentration by ECL blot assay was not normally distributed, and the skewness of the distribution varied with age. The reference values in the charts constructed by the polynomial equation model depend critically on the assumption of normality without time-varying skewness and non-normal kurtosis accommodation (Silverwood and Cole, 2007). Hence, we thought that the LMS method was superior to a general polynomial structural equation model in the present study. Second, when we utilize these established references to analyze many measurements for clinical or research purposes, the Z-score for any individual measurement can be easily calculated with this method (Vaz Fragoso et al., 2011). In addition, the LMS method maximum penalized likelihood was used to estimate the age-related curves for each of the L, M, and S by natural cubic splines. It indicated that the subjective grouping step was removed, and the curve fitting across age was controlled directly by the values of equivalent degrees of freedom for three smoothing parameters (Cole et al., 1998).
So, we represent the slow decline in serum TK1 concentration from young to middle aged and further reaching a plateau in the elderly smoothly in the newly established centile curves, adopting the LMS method with all subjects together, which included adequate samples for smoothing centile curves.
The usefulness of reference centiles is demonstrated in screening for patients with malignant solid tumors, especially in the transition period aged between 32 and 59 years. The mean pretreatment STK1 Z-score in patients with malignant solid tumors obtained from previous clinical trials or health screening was 0.01 ± 0.99 (males, −0.07 ± 0.97; females, 0.09 ± 1.02) and its sensitivity in detecting patients less than −2SD was 97.41% (males, 96.97%; females, 98.04%). It is reasonable to conclude that newly established references for serum TK1 levels were useful for screening patients with malignant solid tumors in the transition period. In the subsample, the present study evaluated the threshold value of STK1 to predict malignant solid tumors using ROC analysis. The 85th percentiles were identified as the thresholds for diagnosing malignant solid tumors in those health screening participants.
On the contrary, the utility of STK1 for malignant solid tumors was limited, as the percentage of those 116 patients showing less than −2 SDS was 2.59% (males, 3.03%: females, 1.96%). These results may be explained by the fact that STK1 appears to be regulated by multiple factors and a certain percentage of cancer patients have completely normal results. However, the mean SDS of STK1 levels in those patients was 0.01 ± 0.99 (males, −0.07 ± 0.97; females, 0.09 ± 1.02), which was low enough to consider those malignant solid tumors as differential diagnosis.
This study has several limitations. First, the cross-sectional nature of the study should be considered when interpreting the findings reported. Second, selection bias might have occurred because participants were urban adults from middle to upper socioeconomic strata who underwent a health checkup in a single area of China. Finally, since the antibody used for the ECL blot assay cannot probe with some TK1 mutation at present, it is possible to get a low STK1 concentration in certain patients with cancer. Therefore, our age-specific reference ranges need to be validated in other healthy populations as well.
In conclusion, the present study established age- and gender-specific normative data of serum TK1 for the Chinese population and showed that the serum TK1 concentration declines with age from youth to middle age and keeps a plateau pattern in late adulthood. Furthermore, the utility of this reference showed sensitively for screening patients with malignant solid tumor pretreatment. Further studies are needed to assess the age-specific reference ranges in other healthy populations.
Footnotes
Acknowledgments
This work was supported, in part, by a grant from Key Science and Technology Projects in Hunan Province (2011SK2012) and by a grant from Science and Technology Plan Projects (2013BAI04B01).The authors thank Chang Liu for his help in programming and statistical analyses as well as all participants for their contribution.
Author Disclosure Statement
No competing financial interests exist.