
Abstract
Objective: To examine transforming growth factor beta 1 (TGFβ1) gene polymorphisms in Turkish patients with nonsyndromic cleft lip with/without cleft palate (nsCL/P). Methods: A total of 205 Turkish subjects were included; 80 nsCL/P patients and 125 unrelated control individuals. Analysis of gene polymorphisms was carried out by polymerase chain reaction and DNA sequencing. Results: We found the substitution of a proline by a leucine at codon 10 (Pro10Leu) and the substitution of an arginine by a proline at codon 25 (Arg25Pro) in exon 1 of the TGFβ1 gene in nsCL/P patients. Conclusion: This is the first report investigating prevalence of TGFβ1 polymorphisms in Turkish patients with nsCL/P.
Introduction
P
Previous studies found an association between transforming growth factor beta 1 (TGFβ1) and nsCL/P (Bodo et al., 1999; Jin and Ding, 2014; Stoll et al., 2015). TGFβ is a family of cytokines that regulate cell growth, proliferation, and matrix synthesis (Roberts and Sporn, 1988; Massague, 1990). There are three isoforms of TGFβ in mammals such as TGFβ1, TGFβ2, and TGFβ3 (Fujii et al., 1986). Each TGFβ isoform, which is encoded by a distinct gene, is synthesized from a large precursor protein (Blobe et al., 2000).
Previous studies have displayed high expression of TGFβ1, TGFβ2, and TGFβ3 during the development of palatal shelves (Fitzpatrick et al., 1990; Gehris and Greene, 1992). Effects of TGFβ signaling can be dependent upon the activity of several transcription factors known as Smads (Piek et al., 1999). Polymorphisms that occur either within coding regions or in the promoter can potentially disrupt the gene function by altering the gene activation or transcriptional regulation (Cooper, 2002). In this article, we studied TGFβ1 gene in Turkish patients with nsCL/P.
The TGFβ1 gene consists of seven exons localized on human chromosome 19q13 (Fujii et al., 1986; Derynck et al., 1987). TGFβ1 accelerates palatal shelf fusion in vitro. nsCL/P fibroblast phenotype is associated with TGFβ1 expression. Bodo et al. (1999) have showed that nsCL/P fibroblasts produce less active TGFβ1 mRNA levels with a parallel decrease in TGFβ1 gene.
TGFβ1 polymorphisms have been associated with diseases, including lung cancer, diabetes, cardiovascular diseases, and inflammatory diseases (Yokota et al., 2000; Mattey et al., 2005; Guerra et al., 2012; El-Sherbini et al., 2013). Among these polymorphisms, Pro10Leu (29C>T; rs1800470) and Arg25Pro (74G>C; rs1800471) in the exon 1 are the most frequently reported polymorphisms. At codon 10, TT genotype is associated with high TGFβ1 expression (Eliopoulos et al., 2009). At codon 25, the GG genotype is associated with high TGFβ1 production than heterozygotes (Grainger et al., 1999). These polymorphisms in exon 1 of the TGF-β1 are located in the signal peptide sequence that is cleaved from the TGF-β1 precursor at the level of codon 29. The signal sequence releases export of the newly synthesized protein across the membranes of the endoplasmic reticulum (Cambien et al., 1996).
The purpose of this study was to investigate the association between exon 1 of the TGFβ1 polymorphisms and Turkish patients with nsCL/P and to determine the prevalence of the Turkish population.
Materials and Methods
Study population
For this study, 80 children aged 0-10 years with nsCL/P (the case group), admitted to the Department of Orthodontics of Ankara University Faculty of Dentistry, were selected. Blood samples were collected. The selection criterion for the nsCL/P group was no association with any other major malformations. All cases were examined and screened for the presence of association between nsCL/P and other syndromes. Blood samples were collected from this selected group. The control group comprised 125 healthy children aged 0-10 years with no reported familial history of orofacial clefts. The study approval was obtained from the Ankara University Faculty of Dentistry, Clinical Research Ethics Committee.
Molecular analysis
Genomic DNA was isolated from peripheral blood samples by the conventional phenol-chloroform (Merck) method using proteinase K (MBI Fermentas). Peripheral blood samples were collected in test tubes containing ethylenediaminetetraacetic acid (EDTA).
Approximately, 200 ng of genomic DNA was used as a template for polymerase chain reaction (PCR) amplification of exon 1 of TGFβ1 gene. The primer set included a forward primer 5′-CTA GGT TAT TTC CGT GGG-3′ and the reverse primer 5′-CCT TGG CGT AGT AGT CG-3′ (Stoll et al., 2015).
PCR was carried out in a total volume of 50 μL containing 200 ng of template DNA, 1 U Taq polymerase (Fermentas), and 1× (NH4)2SO4 buffer with 10 pmol of each primer, 0.2 mM of all four dNTPs (Fermentas), and 1.5 mM MgC12. The PCR conditions were 5 min at 95°C followed by 37 cycles of 30 s at 95°C, 30 s at 57°C, and 30 s at 72°C, with a 10-min elongation step at 72°C at the end of each cycle. The PCR products were electrophoresed in a 2% agarose gel containing ethidium bromide. A 523 bp fragment was amplified by PCR. After PCR, we sequenced using an automated sequencer (Beckman Coulter CEQ 2000 XL DNA Analysis System). The detected mutations were confirmed by repeating the sequencing analysis on a new PCR product.
Statistical analysis
Genotype and allele frequencies were calculated by genotype count and compared by χ2 test with the values predicted by the assumption of Hardy-Weinberg equilibrium. Statistical significance was accepted at p < 0.05. The odds ratios (OR) and 95% confidence interval (CI) were calculated and assessed between Pro10Leu and Arg25Pro polymorphisms and nsCL/P.
Results
In our study, the 80 Turkish patients with nsCL/P and 125 unrelated individuals were studied. TGFβ1 analysis revealed two polymorphisms at codon 10 and 25 in exon 1 of the TGFβ1. Figure 1 displays the sequence analysis of the TGFβ1 gene variations.
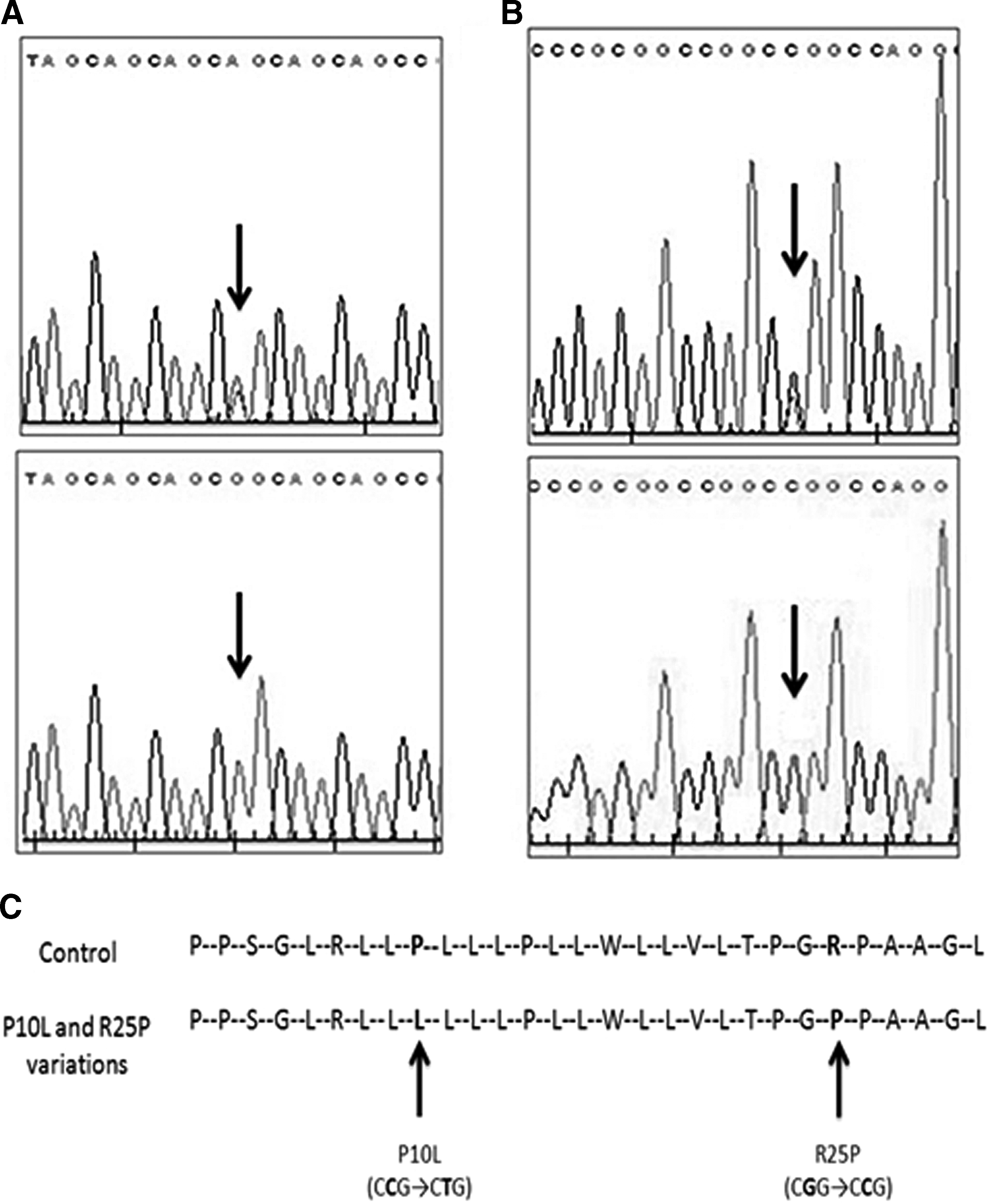
Sequence analysis of the TGFβ1 gene variations at codon 10 and 25:
The first polymorphism of codon 10 was caused by a codon CCG instead of CTG transversion resulting in an amino acid substitution of proline to leucine (Pro10Leu). The second polymorphism at codon 25 was detected. It was caused by a codon CGG instead of CCG transversion resulting in an amino acid substitution of arginine to proline (Arg25Pro). The genotype and allele frequencies of the Pro10Leu and Arg25Pro polymorphisms in nsCL/P patients and controls are shown in Table 1.
CI, confidence interval; nsCL/P, nonsyndromic cleft lip with/without cleft palate; OR, odds ratios.
Twenty-two (28%) of 80 case group had the CT genotype and 41 (51%) were homozygous in TGFβ1 gene Pro10Leu polymorphism. In the control group (n = 125), 48 (38%) were heterozygous and 60 (48%) were homozygous. The frequency of the T allele in the nsCL/P case group and the control group was 65% and 67%, respectively. The frequency of CT genotype was not statistically significant compared to controls (p = 0.06, odds ratio = 2.18 [0.94-5.06], 95% CI). The frequency of TGFβ1 29 C > T homozygous was higher compared to the control group (OR = 1.46 [0.67-3.19], 95% CI, p = 0.66), but the difference was not statistically significant.
Seventy-four (93%) of 80 case group had the GG genotype and six (7%) were GC genotype in TGFβ1 Arg25Pro polymorphism. In the control group (n = 125), 113 (90%) were wild type and 12 (10%) were heterozygous. The frequency of the C allele in the nsCL/P case group and the control group was 6% and 12%, respectively.
The frequency of TGFβ1 74 G > C heterozygous was higher compared to the control group (OR = 1.31 [0.48-3.64], 95% CI, p = 0.79), but the difference was not statistically significant. The frequency of C alleles was higher in nsCL/P compared to the control group (odds ratio = 1.29 [0.48-3.52], 95% CI, p = 0.80), but the differences in frequencies were statistically insignificant.
Discussion
The nsCL/P is a common birth defect, which has a complex etiology, including interaction of environmental and genetic factors (Stuppia et al., 2011). TGFβ1 that is localized at chromosome 19q13 is a candidate gene, which is responsible for the cause of nsCL/P (Murray, 2002).
In present study, we investigated the association between the TGFβ1 and Turkish patients with nsCL/P, and we detected the substitution of a proline by a leucine at codon 10 (Pro10Leu; g.5911C>T) and the substitution of an arginine by a proline at codon 25 (Arg25Pro; g.5956G>C) in exon 1 of the TGFβ1 gene.
Polymorphism Pro10Leu that causes replacement of proline by leucine at position 10 is located in the signal peptide sequence. The polymorphism that occurs in the signal peptide sequence affects the signal peptide's function and export of synthesized protein efficiency (Dunning et al., 2003).
Result of replacement of proline by arginine at position 25, arginine that is polar amino acid is replaced to a charged proline, which is apolar amino acid. Thus, signal peptide regulation leads to differences in export of synthesized protein efficiency (Crilly et al., 2002).
TGFβ signaling has an important role in promoting fusion of the palatal shelves (Bush and Jiang, 2012). Bodo et al. (1999) first reported that TGFβ1 and TGFβ3 are correlated to nsCL/P in a human model. nsCL/P fibroblasts produce less active TGFβ1 with a parallel decrease in TGFβ1 transcription. Jin and Ding (2014) reported the first genetic evidence showing that TGFβ1 and TGFβ2 are functionally required for mouse secondary palate formation in vivo. They showed that 40% of [Tgf-β1+/−; Tgf-β2−/−] mutant embryos displayed cleft palate on C57 background.
In the study, no significant difference was found for TGFβ1 polymorphisms (Pro10Leu and Arg25Pro) and nsCL/P patients. Similar to our conclusion, Stoll et al. (2015) reported no significant association in Leu10Pro polymorphism between nsCL/P patients and control individuals, but exchange of leucine by proline at codon 10 was correlated with Arg25Pro genotype (p < 0.025).
In conclusion, this is the first report investigating prevalence of TGFβ1 Pro10Leu and Arg25Pro gene polymorphisms in Turkish patients with nsCL/P. The present study is helpful to provide knowledge to other researchers about included gene variations analyzed in TGFB pathway in nsCL/P patients. Doing further studies will be beneficial to verify these results with a larger group of patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.