
Abstract
Aims:
In this meta-analysis, we evaluated the usefulness of serum thymidine kinase 1 concentration (STK1c) for monitoring the outcome of extensive open surgery in patients with lung cancer. We also compared STK1c between a healthy population and patients with benign and malignant lung tumors to assess its potential value for early detection of lung cancer and for distinguishing between benign lung disease and malignant cancer.
Materials and Methods:
Related studies were retrieved from publications in PubMed, Cochrane, China National Knowledge Infrastructure, Wanfang databases, and Internet searches. Correlation was evaluated using weighted mean difference. Fixed or random effect models were selected for data analyses based on heterogeneity tested with the chi-square test. Publication bias was assessed using a funnel plot and Egger's test.
Results:
Twenty studies were selected for analysis, which showed that STK1c was significantly (p < 0.00001) reduced by 41.7% 1 month after extensive open surgery, approximately corresponding to an STK1c half-life of 1 month. STK1c levels were significantly higher in lung cancer patients than in healthy persons (p < 0.00001) or in patients with benign lung disease (p < 0.00001). There was also a significant difference in STK1c between patients with benign and malignant lung disease (p < 0.0001).
Conclusions:
The half-life of STK1c may be an important tool in the clinical evaluation of surgical response in patients with lung cancer. STK1c may also be beneficial in the early detection of lung cancer.
Introduction
T
In the clinical assessment of the effectiveness of surgical treatment, the half-life of STK1c has been proposed as an important tool for monitoring the response to treatment in patients with breast cancer (He et al., 2000), gastric cancer (Zou et al., 2002), and renal cell carcinoma (Nisman et al., 2016). STKa has also been used for monitoring the response to chemotherapy in patients with lymphoma and leukemia since 1983 (Gronowitz et al., 1983). However, few studies have used the half-life value of STKa to monitor response to surgery in cancer patients. Thus, when anti-
In controlled clinical studies, STK1c was shown to be a specific and reliable marker for monitoring the treatment, prognosis, relapse, and survival of cancer patients using both blood and solid tumor samples. When tumors were successfully resected using extensive open surgery, STK1c decreased with a half-life (reduce by 50%) of ∼1 month in patients with lung (Li et al., 2005), gastric (Zou et al., 2002), and breast (He et al., 2000) cancers. However, the numbers of cases described in these reports were limited. Although other techniques of measuring STK1c, such as sandwich ELISA, are available, there are no reports to date on the use of these techniques to monitor the response to surgery.
Lung cancer accounts for the majority of cancer-related deaths globally (Siegel et al., 2013). In men, the highest lung cancer incidence rates are found in Eastern and Southern Europe, North America, Micronesia and Polynesia, and Eastern Asia. Among women, it is the fourth most commonly diagnosed cancer and the second leading cause of cancer death. The incidence of lung cancer is markedly increasing in China and other Asian countries, and in Africa. In recent years, computed tomography scanning and other imaging technologies in combination with pathological tumor-node-metastasis staging have improved the survival of lung cancer patients. Unfortunately, biomarkers of value for the early detection or monitoring of lung cancer, much less so for the evaluation of therapeutic effectiveness, have not yet been reported (Rhea and Molinaro, 2011). STK1c is efficacious as a prognostic tool because changes in its levels reflect a patient's response to treatment and risk of disease recurrence (Alegre et al., 2014). However, owing to the limited numbers of cases described in recent clinical studies of STK1c in lung cancer patients, the findings to date are insufficient to guide clinical decision making.
To strengthen the evidence for the potential uses of STK1c in oncology, we used meta-analysis to evaluate the value of STK1c in monitoring the outcome of extensive open surgery in patients with lung cancer. We also compared STK1c levels in healthy individuals with those of patients with benign and malignant lung disease to verify its usefulness as a screening tool for the early detection of lung cancer and to distinguish between benign and malignant lung tumors.
Materials and Methods
Search strategy
Relevant articles published up to April 2016 were retrieved from PubMed, Cochrane, China National Knowledge Infrastructure, and Wanfang databases and from the Internet (www.baidu.com, scholar.google.com) using the following medical subject heading terms: “thymidine kinase 1 or TK1”; “lung or pulmonary”; and “disease or neoplasm or cancer or carcinoma or tumor or malignancy.” The search was restricted to human studies, but not limited linguistically. References from each study, systematic review, and meta-analysis were reviewed to identify further relevant literature, and manual retrieval was used to reduce selection bias.
Inclusion and exclusion criteria
Eligible studies were included strictly in accordance with the following criteria: open access publication; use of the experimental method developed by the Swedish TK1 research team (Sino-Swed Research Institute); STK1c measured using a commercial kit based on an enhanced chemiluminescence dot blot assay system (SSTK Ltd., Shenzhen, China, www.sstkbiotech.com); containing data with corresponding 95% confidence interval (CI), or data that could be re-estimated; use of healthy individuals as control groups; and data that were most sufficient and from the same population. Studies were excluded based on the following criteria: animal or in vitro experiments, review articles, repeated literature, mechanistic studies, no relation to human participants, lack of appropriate control groups, lack of description of analysis method, evaluation using immunohistochemistry and activity, and lack of access to full text.
Data extraction and quality assessment
The full text and additional information for each study were reviewed and the following data were extracted: research details (first author, year of publication, and country of participants), study population characteristics (ethnicity, number of participants, sex ratio, mean age, lung cancer types, and sources of control), and relevant data for meta-analysis (specimens, values, weights, weighted mean difference [WMD], and 95% CI). Two investigators independently used the Newcastle-Ottawa Scale (NOS; Stang, 2010) to assess the quality of studies, and those with NOS scores higher than 5 were included in the meta-analysis.
All patients in studies included in the meta-analysis had undergone extensive open surgery. Surgical injury induces the activation of immunological, inflammatory, metabolic, and endocrine mediators, which are proportional to the severity of the surgical stress. Oxidative stress is also believed to be part of the surgical stress response, and may be associated with myocardial injury, sepsis, pulmonary edema, kidney and liver failure, and increased mortality (Karayiannakis et al., 1997).
Statistical analysis
Meta-analysis was performed using RevMan 5.3 software provided by the Cochrane collaboration network. WMD was used as the effect indicator to evaluate the consistency of the selected studies. We first adjusted WMD by comparing the healthy participants to the lung cancer group, or the benign lung patients to the lung cancer group, or the preoperative to the postoperative group, each with the corresponding 95% CI. Because differences in statistical data could result from a random error or significant heterogeneity among individual studies, a chi-square test was performed and a p-value of <0.05 was considered to indicate significant heterogeneity among individual studies. If significant heterogeneity was observed, a random-effects model was adopted. Otherwise, a fixed-effects model was applied in the meta-analysis. Subgroup analyses could also be conducted to explore the potential sources of between-study heterogeneity. Furthermore, publication bias was estimated using a funnel plot, and a p-value of <0.05 indicated significant publication bias. STATA 12.0 software was used for sensitivity analysis, funnel plot, and Egger's linear regression test to assess publication bias. The difference in STK1c value before and after surgical treatment was determined using Student's t-test (STATA 12.0).
Results
Study selection
The literature retrieval and selection process is shown in Figure 1. A total of 358 articles were identified from database searches after duplicate removal, of which 286 articles were excluded following review of the titles and abstracts. Reviews, letters, and meta-analyses, and articles unrelated to the research topic, were also excluded. This resulted in 72 articles suitable for full-text review, of which 27 were not associated with lung cancer. Furthermore, 25 of the remaining 45 articles were excluded because they did not contain sufficient data (10) or failed to meet the experimental requirements (15). Finally, 20 articles were suitable for the meta-analysis.
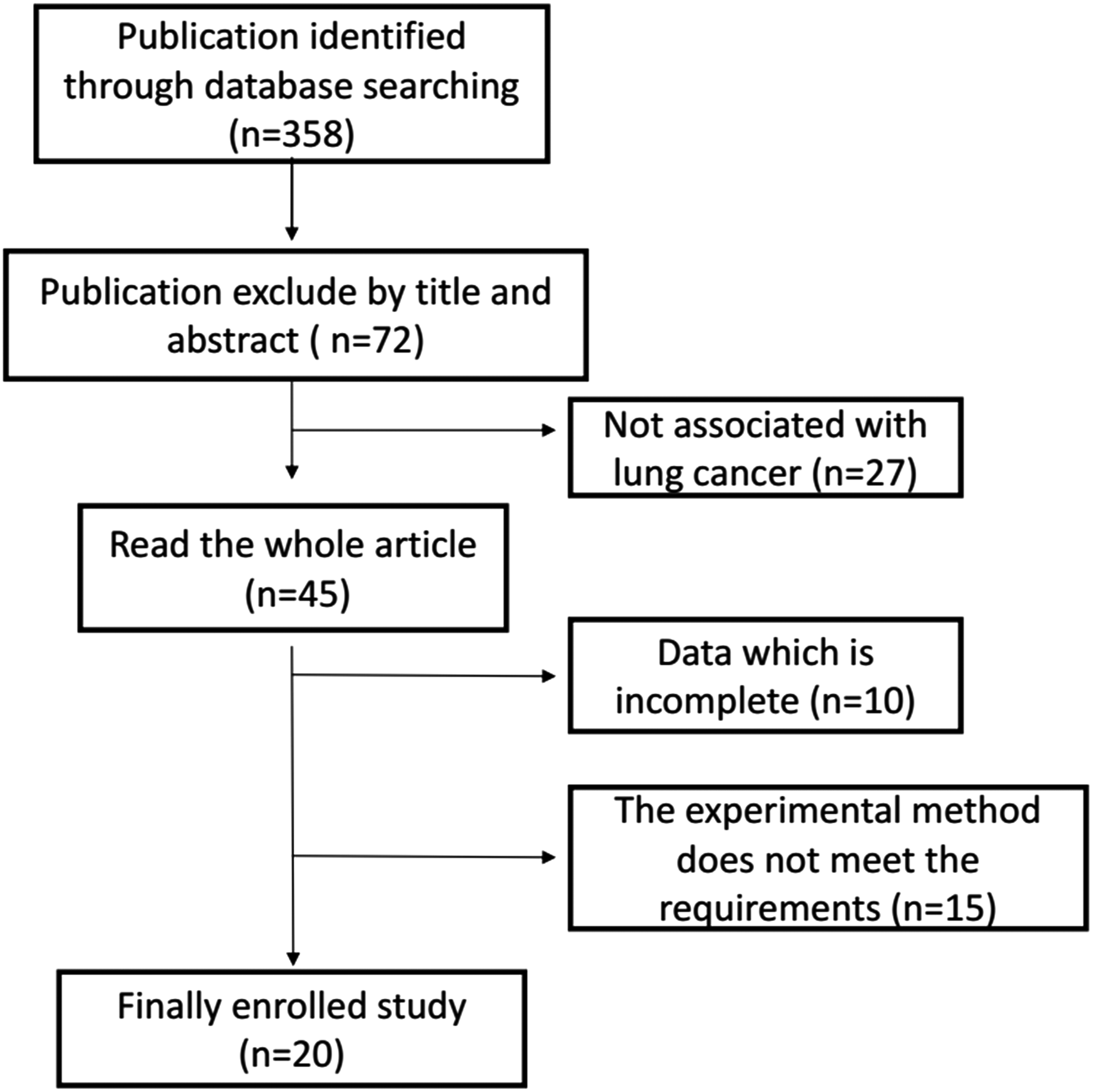
The process of literature retrieval and selection.
Study characteristics
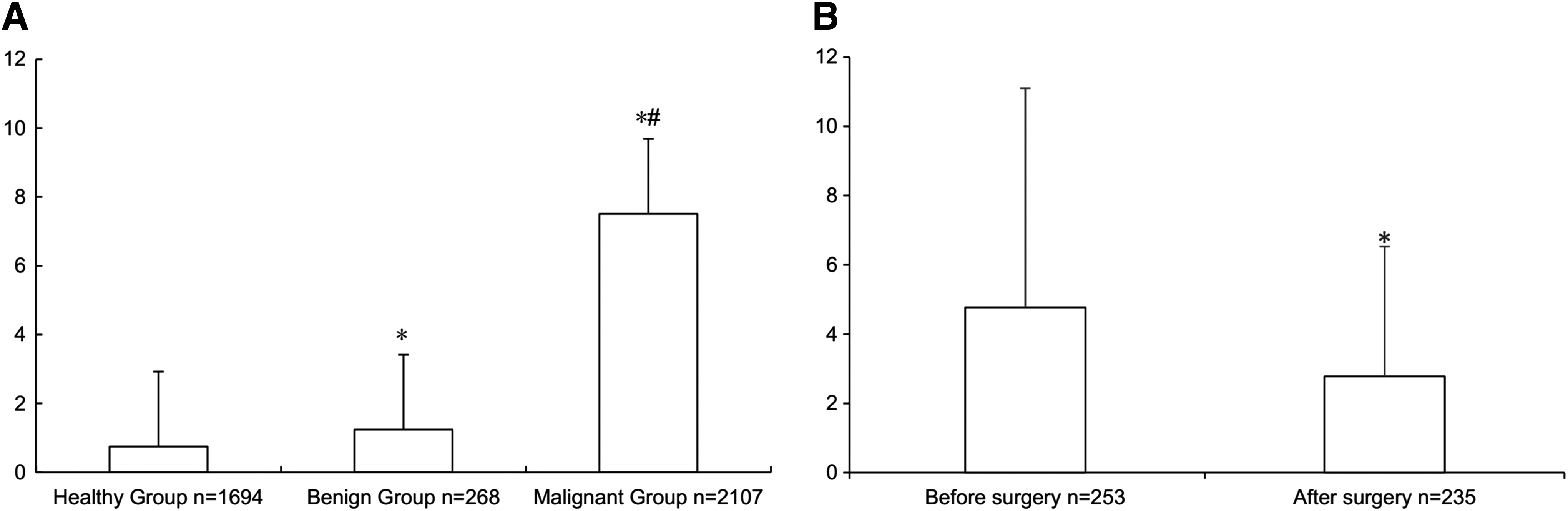
The main clinical features of the selected studies are listed in Table 1. A total of 4069 participants from 20 studies conducted between 2005 and 2015 were included in our analysis. These participants included 1694 individuals in the healthy group, 268 in the benign lung disease group, and 2107 in the lung cancer group. However, after analysis of the correlations between the different groups, not all individuals were included in the final analysis. There were 253 preoperative and 235 postoperative individuals in the lung cancer group, from 6 studies, and determination of the correlation with STK1c values between these groups was the main objective of this study.
Meta-analysis
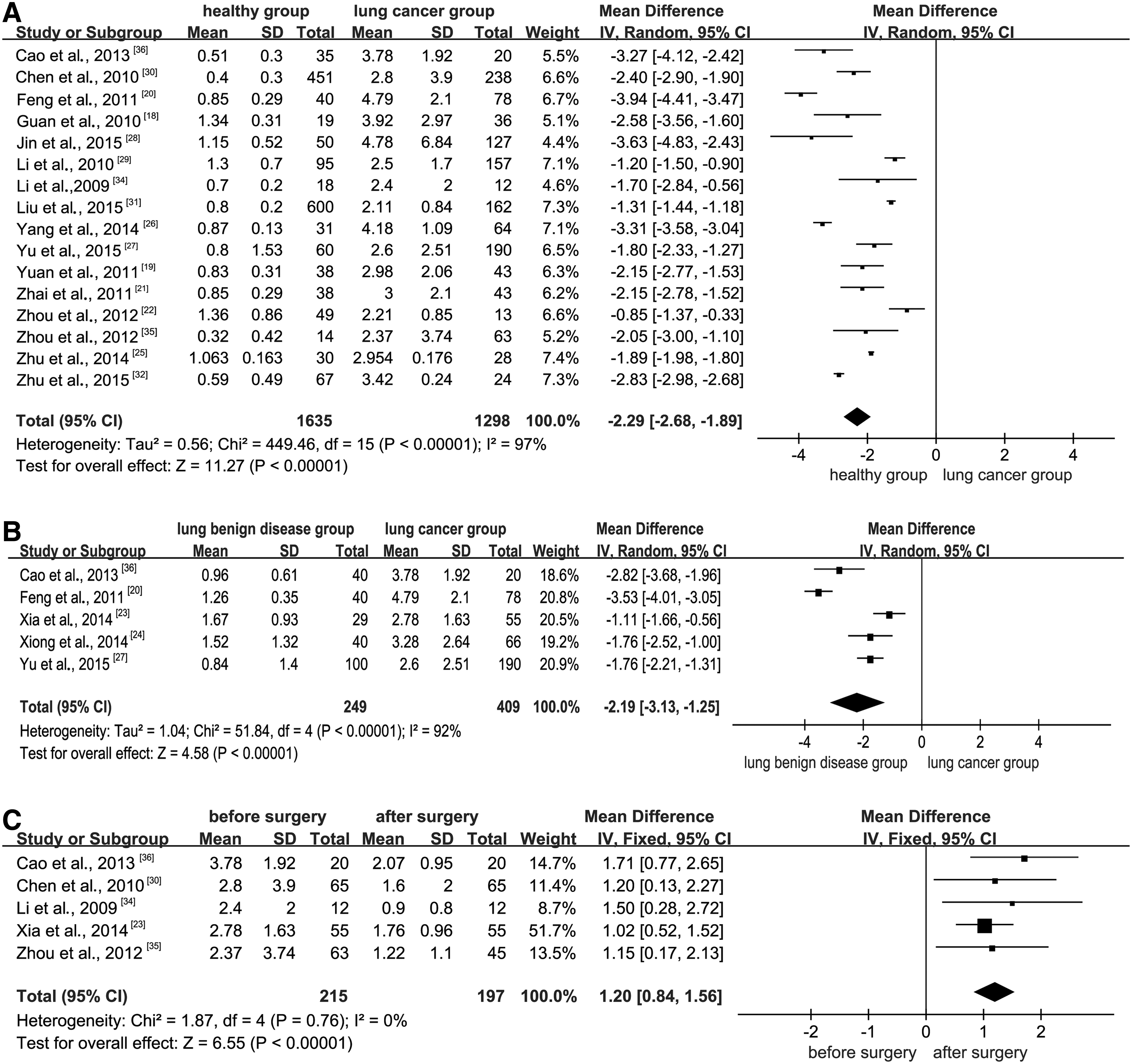
Two studies were further excluded from the 20 selected because they adopted X optical film instead of charge-coupled device (CCD) optical signal acquisition, leading to relatively large divergent data. Of the remaining 18 studies, 16 were selected for STK1c level analysis between the healthy control group (1635 individuals) and the lung cancer group (1298 individuals) (Figs. 2A and 3A). Heterogeneity testing was applied between the two groups, and the difference was statistically significant (p < 0.00001, I2 = 97%). Therefore, a random-effects model was used to merge the effect quantity. The results showed that, at the 0.05 test level, the difference between the two groups was statistically significant (WMD = −2.29; 95% CI −2.68 to −1.89; p < 0.00001). Thus, STK1c levels in the healthy control group (0.75 ± 0.54 pM) were significantly lower than in the lung cancer group (7.51 ± 5.52 pM) and were also lower than the benign disease group (1.24 ± 1.42 pM).
Statistical analysis of healthy control versus lung cancer group
TK1 values compared in each group
STK1c correlation analysis between the benign lung disease and lung cancer groups is shown in Figures 2B and 3A. One of the six selected studies was disregarded for the previous reason of notable data divergence. Five studies were finally used in the analysis, including 249 and 409 individuals in the benign disease and the lung cancer groups, respectively. Heterogeneity testing between the two groups was statistically significant (p < 0.00001, I2 = 92%). Again, a random-effects model was used to merge the effect quantity (WMD = −2.19; 95% CI −3.13 to −1.25; p < 0.00001). STK1c levels in the benign disease group (1.24 ± 1.42 pM) were significantly lower than in the lung cancer group (7.51 ± 5.52 pM).
STK1c values in the preoperative and postoperative groups of patients are shown in Figures 2C and 3B. One study was excluded from the analysis because of a large data difference, as X optical film signal acquisition was again used instead of CCD. The number of individuals in the preoperative and postoperative lung cancer groups was 215 and 197, respectively. Heterogeneity testing between the two groups revealed no statistical significance (p = 0.76, I2 = 0%). Therefore, a fixed-effects model was adopted to merge the effect quantity (WMD = 1.20; 95% CI 0.84-1.56; p < 0.00001). STK1c values significantly decreased after surgery, from 4.77 ± 6.33 pM to 2.78 ± 3.75 pM (p = 0.0000). This represented a decrease of 41.7%, which corresponded to an STK1c half-life of ∼1 month.
Sensitivity analyses and publication bias
Sensitivity analysis was conducted to evaluate the effect of excluding any individual study. By exclusion of one publication at a time in sequence, the summary results of the remained publications did not change substantially. A funnel plot and Egger tests were used to examine the potential for publication bias. In our meta-analysis, sensitivity in the healthy control and lung cancer groups was stable, and the funnel plot indicated no evidence of publication bias as shown in Figure 4A, B. The Egger test also showed a lack of publication bias (Table 2, p = 0.368). We were unable to perform a similar analysis between the benign and malignant lung disease groups, or between the preoperative and postoperative groups, because of the limited numbers of cases in these groups.

Sensitivity analysis
Discussion
Tumors are primarily characterized by uncontrolled cell proliferation, and the proliferative activity correlates with the aggressiveness of the disease. Despite recent advances, lung cancer remains a devastating disease with an unfavorable prognosis. Major contributing factors to the poor outcome include difficulties in diagnosing the disease sufficiently early in its course-during the asymptomatic stage-and an incomplete understanding of the biology underlying disease progression. Biomarkers of tumor cell proliferation are clinically valuable because they may improve the early detection and treatment monitoring of the disease. Unfortunately, only a few biomarkers are established for use in the early detection of tumors in screening programs (Zhou et al., 2013). Controlled clinical studies have shown that STK1c has potential as a biomarker for monitoring tumor therapy and relapse, and has therefore been extensively studied in recent years using both biochemical and immunological techniques. When STK1c was compared with commonly used biomarkers such as CYFRA21-1 and NSE in patients with lung cancer, all three serum biomarkers were significantly increased in patients compared with healthy individuals, with positive rates for STK1c, CYFRA21-1, and NSE of 74.4%, 51.2%, and 46.5%, respectively (Zhou et al., 2013). Moreover, biomarkers alone or in combination have the potential for clinical use in lung cancer treatment. For example, the positive rates of STK1c, CEA, CA-125, and CA-199 in a 6-18-month follow-up study were found to correlate with treatment outcomes as follows: STK1c (91.7%), CA-125 (86.7%), CEA (63.6%), CA-199 (61.6%), STK1c + CA-125 (100%), STK1c + CEA (95.8%), and STK1c + CA-199 (95.8%) (Xu et al., 2009a, 2009b; Zeng et al., 2009). Studies using immunohistochemical analysis of TK1 in lung cancer cells also showed that it was a better prognostic biomarker than Ki-67 for pT1 adenocarcinoma (Xu et al., 2014). Therefore, compared with other lung cancer biomarkers, STK1c provides more useful and potentially reliable information on tumor cell proliferation. However, clinical evidence for the detection of TK1 levels in patients with lung cancer remains insufficient for its use in the early prediction and monitoring of surgical treatment effects.
As reported by Cao et al. (2016), peak levels of STK1 are observed before 20 years of age in both sexes. After the age of 20, levels decrease slowly from 0.51 to 0.36 pM, reaching a plateau at a mean of 0.35 pM in late adulthood. The mean pretreatment STK1c Z-scores in patients with solid malignant tumors obtained from related cancer studies were 0.01-0.99 (men, 0.07-0.97; women, 0.09-1.02). Thus, Cao et al. (2016) established an age- and sex-specific normative data of STK1c for the Chinese population, and showed that levels of STK1c declined with age from youth to middle age and plateaued in late adulthood. Furthermore, the utility of this reference showed sensitivity for the pretreatment screening of patients with malignant solid tumors. Based on these findings, the present study aimed to explore the use of STK1c as a predictive factor for monitoring the outcome of surgery in lung cancer patients. In our meta-analysis, we found that the mean value of STK1c in the healthy control group was significantly lower than that in the lung cancer group (p < 0.00001), indicating that STK1c could serve as an early indicator of lung cancer risk. Furthermore, STK1c values were significantly lower in the benign lung disease group than in the lung cancer group (p < 0.00001), but were significantly higher than those in healthy individuals (p = 0.0000), demonstrating that STK1c could distinguish between different levels of abnormal proliferation of lung tumor cells, a finding with important clinical implications for the differentiation between benign and malignant tumors. More importantly, STK1c level was found to be a reliable index for monitoring the effect of extensive open surgery in lung cancer patients, with a half-life of about 1 month. This was consistent with previous lung cancer studies where STK1c decreased by 55% in a tumor-free group but increased by 115% in a tumor-metastatic group (Li et al., 2005), and also correlated with tumor grade, lymph nodal status, and tumor size (Chen et al., 2010).
The half-life of STK1c may depend on treatment type, including extensive open surgery, minimally invasive surgery, or chemotherapy, and on different types of malignant tumors. In previous studies, following extensive open surgery in patients with non-small cell lung, esophageal, or gastric cardia cancers (Li et al., 2010a) or gastric cancer (Zou et al., 2002), a transient increase in STK1c (100-234%) within 1 week of surgery was observed. This change might be attributable to anemia, infection, and/or inflammation induced by the extensive open surgery (Li et al., 2010b). After 1 month, STK1c values had decreased by 40-50%, which corresponded to a half-life of about 1 month. However, neuroendocrine stress and inflammatory responses were contained using laparoscopic (minimally invasive surgery) treatment. In a study on 56 primary bladder cancer patients, STK1c had a half-life of 6 days after cystectomy using an electrosurgical technique (Zhang et al., 2006). All patients were regarded as tumor-free after the treatment. STK1c decreased further, reaching levels corresponding to those of healthy individuals by 1 month after surgery. The mean STK1c value in patients with non-Hodgkin's lymphoma during treatment with chemotherapy has also been investigated, and it was found to increase to 127% during the first few days of treatment and then decline by 79% 1 month after the start of chemotherapy (Pan et al., 2008). Thus, it has been concluded that STK1c should not be used for disease monitoring during the first week after extensive open surgery, to avoid transient nontumor-related increases in its level (Li et al., 2010b). Instead, STK1c should be determined ∼1 month or later after surgery, when the accuracy of this biomarker is clinically optimal.
We suggest that the half-life of STK1c represents an important tool for monitoring surgical response in patients with lung cancer. The half-life index may provide valuable information on how to assess the likely effects of treatment on a patient and to devise a reasonable treatment plan. Moreover, this information may enable individualized therapy for different cancers, and avoidance of overtreatment or unplanned changes in treatment strategy. The elevated STK1c levels observed in patients with disease recurrence after curative-intent surgery also represent a new option for evaluating therapeutic outcome in a short time period. Thus, the half-life index of STK1c may provide information that could improve survival and enhance the quality of life among cancer patients.
Our meta-analysis had some limitations. First, several unpublished results were not included. Second, possible bias, such as selection and publication bias, may have occurred in the study as comparison between some groups could not be done because of the small number of references. Finally, because of the limited referred conditions, subgroup analysis to explore potential sources of inter-study heterogeneity, such as countries and cancer types, was not performed.
In conclusion, STK1c is beneficial for monitoring patients after extensive open lung surgery, and for evaluating the risk of developing malignant tumors to enable early detection.
Footnotes
Acknowledgments
This work was supported by Natural Science Foundation of Shanghai (No. 14ZR1413200), Shanghai Municipal Commission of Health and Family Planning, Key developing disciplines (No. 2015ZB0501), and Shanghai Key Laboratory of Clinical Geriatric Medicine (No. 13dz2260700). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article. This meta-study was made possible by research cooperation between oncology doctors running clinical investigations on TK1 in China, Sino-Swed Molecular Bio-Medicine Research Institute, Shanghai, China, developing the TK1 assay.
Author Disclosure Statement
No competing financial interests exist.