
Abstract
Aim:
The genetic variation in the CD14 rs2569190 promoter region contributes to the susceptibility of developing periodontitis. Since, CD14 gene polymorphism studies among various ethnic populations have produced conflicting results, the present study was designed to unearth the association between the CD14 rs2569190 gene polymorphism and generalized chronic periodontitis (GCP) in a South Indian population of Tamil ethnicity.
Methods:
Polymorphisms in the CD14 rs2569190 promoter region were analyzed in 96 subjects who were periodontally healthy and 96 patients with GCP. DNA extracted from peripheral venous blood was genotyped by polymerase chain reaction-restriction fragment length polymorphism analysis. One-way analysis of variance, Chi-square testing, and logistic regression analysis were used to test association between GCP and the CD14 rs2569190 single nucleotide polymorphism (SNP).
Results:
The distribution of the CD14 rs2569190 genotypes and allele frequencies showed significant differences between the test and control groups. Prevalence of the polymorphic TT genotype and T allele of the CD14 rs2569190 were significantly increased in GCP patients when compared with healthy controls.
Conclusion:
The results of the present study suggest that the T allele and the TT genotype of the rs2569190 SNP in the promoter region of the CD14 gene are associated with GCP in a South Indian population of Tamil ethnicity.
Introduction
P
The CD14 is a pattern recognition receptor (PRR) and its production is genetically regulated. The CD14 is a single-copy gene encoded on chromosome 5q23-21 and expresses two protein forms: membrane-bound CD14 (mCD14) and soluble CD14 (sCD14) (Holla et al., 2002). mCD14 is a 55 kD glycosylphosphatidylinositol-anchored membrane protein expressed on the surface of monocytes/macrophages, neutrophils, and gingival fibroblast and is involved in the process of cellular response to bacterial lipopolysaccharide (LPS) (Goyert et al., 1998). The sCD14 lacks the glycosylphosphatidylinositol anchor and circulates in high amounts in plasma (Bazil et al., 1986). sCD14 is identified for its potential of modulating cellular and humoral immune responses by interacting directly with T and B cells. The concentration of sCD14 in serum is elevated in many systemic, inflammatory, immunological, and infectious diseases. CD14 is implicated in the LPS-mediated bone resorption and monocyte-endothelial cell interactions (Holla et al., 2002).
Occurrence of mCD14 and sCD14 forms of the CD14 receptor has been demonstrated in subjects with periodontal disease. Interestingly a single nucleotide polymorphism (SNP) (C > T) at CD14 rs2569190 (−260) promoter region (also known as −159) causes the gene to express elevated levels of sCD14. Both heterozygous (CT) and homozygous (TT) genotypes of CD14 express elevated levels of sCD14 than CD14 gene with CC genotype. Hence, patients with higher expression of CD14 genotypes (CT and TT) exhibit an increased serum level of sCD14.
Literature evidence of CD14 gene polymorphism in various ethnic populations has established conflicting outcomes. Studies in Caucasian population demonstrated affirmative (Donati et al., 2005; Tervonen et al., 2007; Sahingur et al., 2011) and negative (James et al., 2007) association with generalized chronic periodontitis (GCP). Studies in Asian populations also illustrate contradictory association of CD14 rs2569190 gene polymorphism with GCP (Yamazaki et al., 2003; Loo et al., 2012). Presently, there have been no studies on the association of CD14 gene polymorphism with periodontal diseases in Indian population. Hence, the present study was intended to unearth the association of CD14 rs2569190 genotype with GCP in a South Indian population of Tamil ethnicity.
Materials and Methods
Study sample
The total study sample included 192 probands recruited from the Outpatient Department of Periodontology, SRM Dental College, Chennai, India from April 2015 to July 2016. The study was approved by the Ethics Committee and Scientific Committee of the Institutional Review Board (SRMDC/IRB/2014/MDS/No.502) and informed consent was obtained from all participating individuals. All samples were from individuals of South Indian Tamil ethnicity.
Sample size calculation
Sample size was calculated based on the allele frequencies reported by Donati et al. (2005). According to the results of the abovementioned study, to obtain a power of 90% with α error of 5%, our total sample included 192 probands representing 96 healthy controls and 96 individuals diagnosed with GCP. Individuals were diagnosed to have GCP when presented with clinical attachment loss (CAL) ≥5 mm, and probing pocket depth (PPD) ≥5 mm involving ≥30% sites. The inclusion criteria for healthy gingiva were: absence of gingival bleeding on probing, PPD ≤3 mm, no attachment loss, absence of any clinical signs of gingival inflammation, and no previous history of periodontal disease. Current or former smokers, pregnant and lactating women, history of antibiotic usage in the past 6 months, systemic disease influencing periodontal pathogenesis and/or treatment outcome, and periodontal disease modifiers, such as food impaction, factitious habits, and bruxism, were excluded from the study.
Clinical examination
A full mouth periodontal examination was conducted and parameters assessed were plaque index (PI) (Loe, 1967), gingival index (GI) (Silness and Loe, 1964), PPD, and CAL at six sites per tooth. All the clinical parameters were recorded by the same examiner (D.I.) using a University of North Carolina 15 probe.
Sample collection
One milliliter of peripheral venous blood was collected under aseptic conditions from the antecubital vein and transferred to an ethylenediaminetetraacetic acid (EDTA)-coated vacutainer and stored in a deep freeze refrigerator (−80°C). The samples were processed at Enable BioLabs, a research laboratory situated at Urapakkam, Chennai, India. DNA extraction was performed using the Column-Based DNA Extraction Kit (Cat. no. P4850; Sigma-Aldrich, St. Louis, MO) in accordance with the manufacturer's advised protocols. The concentration was determined by analyzing 1 μL of the sample in a fluorescence-based DNA quantifier (Qubit, Austria).
Polymerase chain reaction for CD14 promoter SNP
Primers were designed to specifically amplify 830 base pair region of promoter sequence of CD14 rs2569190 gene (flanking the known polymorphism site at −260 region) using the following primers:
Forward primer: GCTGAGGTTCGGAGAAGTTGC
Reverse primer: GGTGCCAACAGATGAGGTTCAC
Polymerase chain reaction (PCR) was performed on 25 ng of DNA samples under the following conditions: after an initial denaturation at 94°C for 5 min, 35 cycles of denaturation at 94°C for 45 s, primer annealing at 55°C for 45 s, primer extension at 72°C for 1 min was performed, with a final extension at 72°C for 5 min. A negative control reaction without DNA was run to confirm the specificity of amplification in experimental samples. As the PCR amplifies the promoter region of CD14 containing the polymorphism, the PCR amplicons must be considered as copies of the promoter region itself.
PCR-restriction fragment length polymorphism analysis
Five microliters of PCR amplicons was digested with polymorphism-sensitive type II restriction endonuclease, AvaII (TaKaRa, Japan) and were analyzed by running them in a 1.5% agarose gel at 100 V for 30 min with 1X TAE (Tris Acetate EDTA) buffer. The DNA bands were visualized by staining the gel with Ethidium Bromide and images were captured in a gel documentation unit. The results were analyzed based on the number of bands and their migration pattern in the agarose gel corresponding to DNA size marker. A representative image is depicted in Figure 1.

Agarose gel electrophoresis of PCR amplicons digested with AvaII enzyme Lane 1: DNA size marker, Test 1 and 14: homozygous TT genotype, Test 2-4, 7, 11-13, and 15: hetreozygous CT genotype, and Test 5, 6, 8-10: homozygous CC genotype.
Statistical analysis
To compare the mean values between genotypes, one-way analysis of variance was applied followed by Tukey's honest significant difference test for multiple pairwise comparisons. To evaluate mean values between test and control groups, independent samples t-test was applied. To compare proportions between test and control groups and to assess Hardy-Weinberg equilibrium (HWE), Chi-square test was applied. Univariate logistic regression analysis was performed to estimate the odds ratios of the genotypes and allele associated with periodontitis. Significance level was predetermined as 5% (α = 0.05).
Results
The present study was undertaken to investigate the role of CD14 rs2569190 gene polymorphism in patients with GCP in a South Indian population of Tamil ethnicity and compare it with periodontally healthy subjects. Intra-examiner variability and reliability were assessed by intraclass correlation coefficients using a two-way random effects model. An intraclass correlation coefficient of >0.85 was found.
The demographic data of the study population are summarized in Table 1. There was a statistically significant difference in the PI, GI, and PPD between the test and the control groups. The association of CD14 rs2569190 genotypes (CC, CT, and TT) and the alleles (C and T) with GCP is shown in Table 2. The genotype distribution was found to be in HWE in the test and control groups. Logistic regression analysis was used to evaluate statistical significance of the association of genotype with GCP. The homozygous CC genotype was present in 30.2% (29 out of 96) periodontally healthy subjects and 22.9% (22 out of 96) in subjects with GCP. The distribution of the heterozygous CT genotype was 53.1% (51 out of 96) and 44.8% (43 out of 96) in periodontally healthy and GCP subjects, respectively. The homozygous TT genotype occurred in 16.7% (16 out of 96) of periodontally healthy subjects and 32.3% (31 out of 96) of chronic periodontitis subjects. It was observed that the TT genotype of CD14 rs2569190 was significantly associated with GCP (odds ratio [OR], 2.55; 95% confidence interval [CI], 1.13-5.79; p-value 0.025).
Denotes statistical significance.
CAL, clinical attachment loss; GI, gingival index; PI, plaque index; PPD, probing pocket depth.
p < 0.05 indicates statistical significance.
CI, confidence interval; HWE, Hardy-Weinberg equilibrium; OR, odds ratio.
When proportions of the C and T alleles were compared between test and control groups, it was observed that frequency of both C and T alleles were statistically significant (p-value 0.025). However, the distribution of T allele was found to be higher (55.9%) compared with C allele (44%) in subjects with GCP. It was observed that the T allele of CD14 rs2569190 was strongly correlated with GCP (OR, 1.59; 95% CI, 1.06-2.37; p-value 0.025) (Fig. 3).
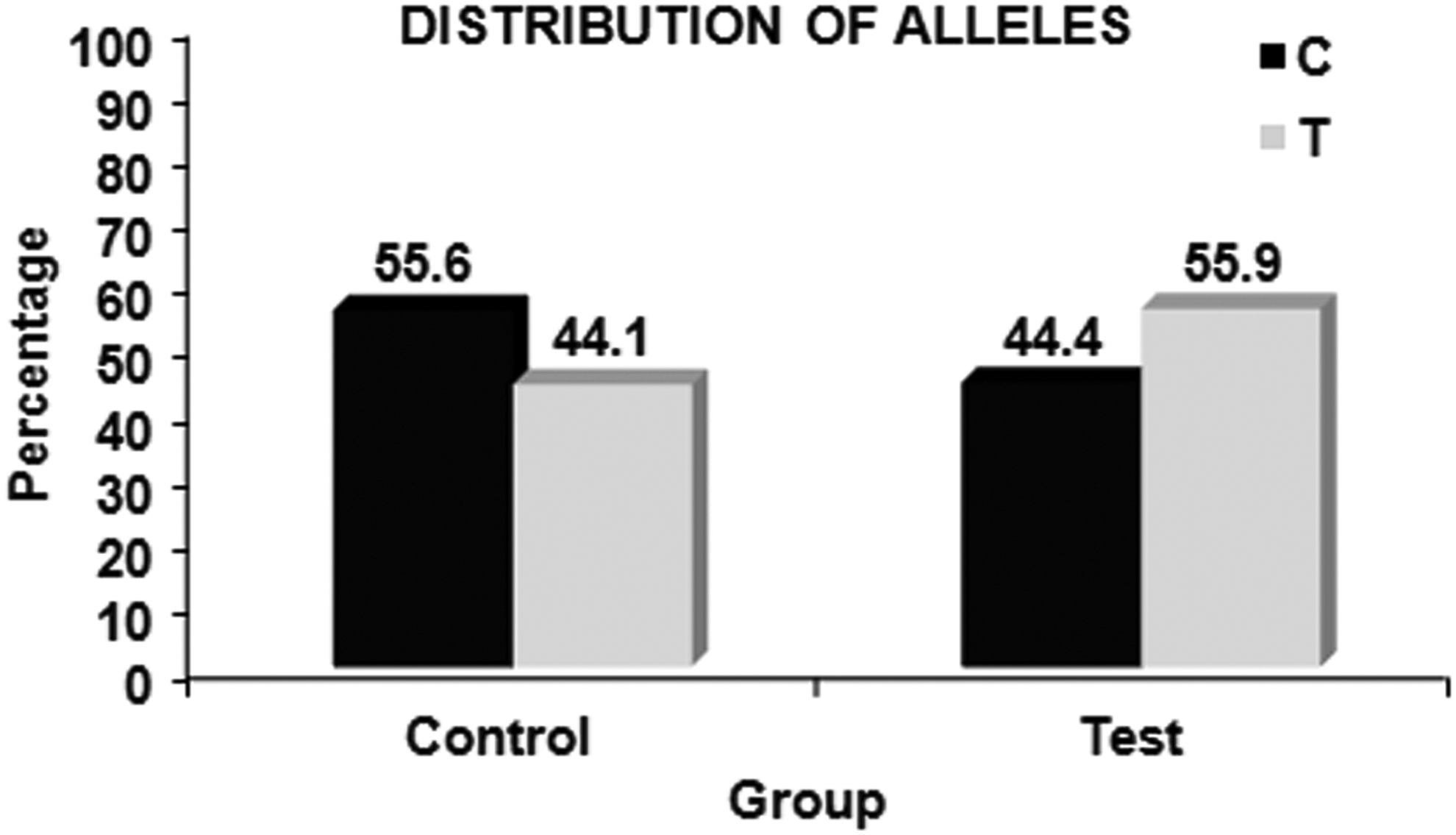
Distribution of allele frequencies between groups.
Discussion
The association of CD14 rs2569190 with GCP susceptibility was assessed in the present study. The CD14 PRR has a unique ability to bind LPS that are expressed by the Gram-negative bacteria. CD14 interacts exclusively with bacterial LPS that are bound with high affinity to the systemically circulating LPS-binding protein (LBP) (Wright et al. 1990). The signal transduction of the LPS/LBP/CD14 ternary complex on effector cells is then transferred through the TLR4/MD-2 (da Silva Correia et al. 2001). Upon stimulation, the TLR4/MD-2 complex leads to the activation of innate host defense mechanisms through the nuclear factor-κB pathway and the engagement of this complex results in release of proinflammatory cytokines, such as TNF-α, IL-β, IL-6, and interferon-δ (Antal-Szalmas, 2000; Medzhitov and Janeway, 2000; Aderem et al., 2000). It has been reported that the mechanisms involved in CD14/TLR-mediated intracellular signal transduction consisted of the activation of IκB kinase (IKK)-NF-κB pathway and three mitogen-activated protein kinase pathways (ERK, JNK, and p38) (Guha and Mackman, 2001).
The CD14 rs2569190 was researched in different populations across the world and resulted in contradictory results. The disparity in this association could be attributable to the ethnic differences among various populations. In the present study, all the polymorphic CD14 rs2569190 genotype (CC, CT, and TT) had a statistically significant difference between test and control groups. CC and CT genotypes were higher in the periodontally healthy subjects, whereas the TT genotype was higher in the subjects with GCP (Fig. 2). The results obtained in the present study is in accordance with Laine et al. (2005) who observed that CD14 rs2569190 TT genotype was established significantly more often than the C/T and C/C genotypes in periodontitis patients compared with controls among Dutch Caucasians, and Loo et al. (2012) who demonstrated that patients suffering from GCP presented more frequently with the −159 T/T genotype of the CD14 gene in Chinese subjects and contrasting with those obtained by Sahingur et al. (2011) who demonstrated that the CC genotype of the CD14 rs2569190 gene was associated with the susceptibility to GCP in Caucasians of New York.
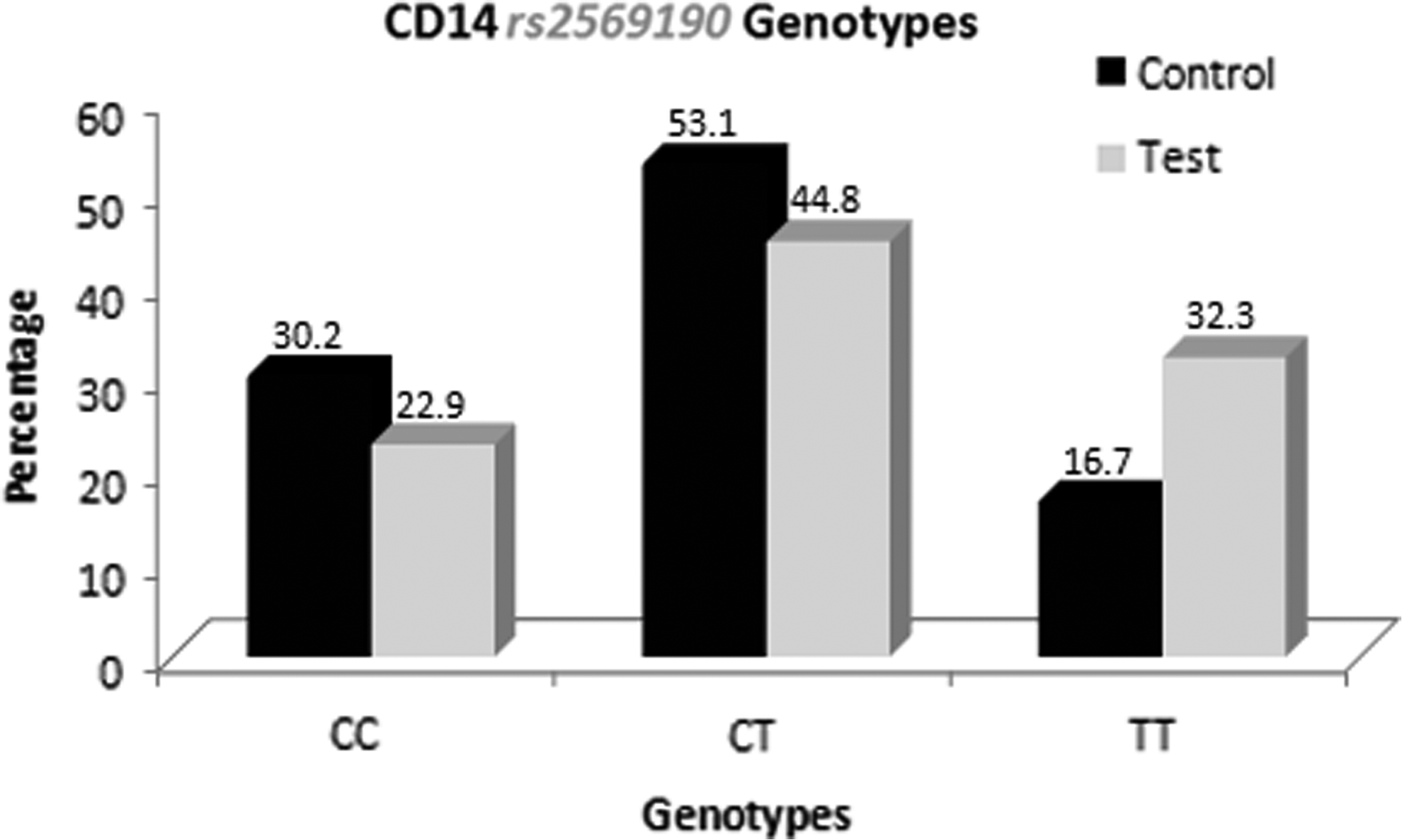
Comparative representation of polymorphic CD14 rs2569190 genotypes among test and control.
The association of various polymorphic genotypes in CD14 rs2569190 showed a strong correlation of the TT genotype with periodontitis (OR, 2.55; 95% CI, 1.13-5.79; p-value 0.025) which was statistically significant (Table 2). The results of the present study is comparable to Laine et al. (2005) who demonstrated that the CD14 rs2569190 TT genotype was significantly associated with periodontitis (OR, 2.0; 95% CI, 1.1-3.9; p-value 0.038) and contrasting to Yamazaki et al. (2003) who failed to find any association between CD14 rs2569190 TT genotype with periodontitis and Sahingur et al. (2011) who observed that the CC genotype of CD14 rs2569190 gene was correlated to the susceptibility to chronic periodontitis and the proportion of CD14 rs2569190 TT genotype was superior in the periodontally healthy subjects. In the present study, the polymorphic heterozygous CT genotype exhibited an OR of 1.11 (95% CI, 0.56-2.21), which was not statistically significant (p-value 0.763) (Table 2).
To corroborate the polymorphic allele associated with GCP, logistic regression analysis was performed, which revealed that the polymorphic T allele was significantly associated with GCP (OR, 1.59; 95% CI, 1.06-2.37; p-value 0.025) (Table 2). The results of the present study were comparable to those obtained by Tervonen et al. (2007) who demonstrated that the T-containing genotype of the CD14 rs2569190 was associated with advanced periodontal disease and distinct to those obtained by Sahingur et al. (2011) who demonstrated that the C allele of the CD14 rs2569190 gene polymorphism was associated with a twofold increased susceptibility to disease. It has been hypothesized by LeVan et al. (2001) that the changes in the T allele variant decreases affinity of Sp-binding protein, which enhances the transcriptional activity of Sp1, Sp2, and Sp3 in the CD14 promoter region. This variation of the CD14 gene plays a prominent role in the pathogenesis of allergy and inflammatory diseases. In the present study, despite harboring the polymorphic TT genotype, periodontally healthy subjects did not develop periodontitis as they maintained good oral hygiene at the time of evaluation.
The results of the present study were similar to those obtained by Tervonen et al. (2007), Raunio et al. (2009), and Laine et al. (2005); however, direct comparisons with these studies cannot be made due to ethnic differences in genotype distribution, sample size, environmental effects, and clinical heterogeneity. The findings of the present study suggested that the subjects with CD14 rs2569190 TT genotype polymorphism are more susceptible to develop GCP. Hence, the TT genotype and the T allele of the CD14 rs2569190 gene may be considered as a risk determinant for GCP. Clinical implications of the current observations could incorporate genetic tests to identify susceptible subjects at risk for periodontal disease and application of appropriate preventive strategies.
A larger sample size, categorization of the subjects in test group according to their disease severity (mild, moderate, and severe periodontitis), assessing the levels of mCD14 and sCD14 in various fluids, and involving diverse Indian ethnicities could have improved study results. Since the study was a cross-sectional observational study, it gives information about association of CD14 rs2569190 with GCP at a given time point. However, transition of healthy subjects to a diseased state (periodontitis), even though exhibiting a CD14 gene polymorphism, could not be evaluated as such observation requires a longitudinal study. Within the confines of the present study, it can be concluded that a SNP identified in the promoter region of CD14 rs2569190 is associated with GCP in a South Indian population of Tamil ethnicity.
Footnotes
Acknowledgments
The authors would like to acknowledge SRM Dental College, Ramapuram, Chennai and Dr. Arvind Ramanathan, BDS, MSc (Molecular Biology), PhD (Molecular Oncology, Tokyo, Japan), Director of Research, Enable BioLabs, for providing assistance in conducting the research.
Author Disclosure Statement
No competing financial interests exist.