
Abstract
Background:
Peritoneal carcinomatosis (PC) is an important cause of morbidity and mortality among patients with gastric cancer. Thus, it is important to identify an ideal biomarker for PC.
Methods:
Plasma and ascites samples were collected from gastric cancer patients with PC and a control group. Lysophosphatidic acid (LPA) levels were tested and analyzed.
Results:
The plasma LPA levels of gastric cancer patients with PC were significantly higher than those in gastric cancer patients after radical resection (p = 0.046) and healthy volunteers (p < 0.001). Besides, plasma LPA levels were statistically lower after chemotherapy in gastric cancer patients with PC (p = 0.028). Furthermore, the ascites LPA levels were significantly higher in gastric cancer patients with peritoneal carcinomatosis than those in liver cirrhosis patients (p < 0.001). Moreover, ascites LPA levels were statistically lower after intraperitoneal chemotherapy injection than before (p < 0.001). In addition, the plasma LPA levels were significantly associated with serum CA125 levels (p = 0.032) and TNM stage in gastric cancer patients (p = 0.009). Individuals with plasma LPA levels >20,000 ng/mL had significantly worse overall survival (OS) than those with plasma LPA levels <20,000 ng/mL group (p = 0.006). In addition the group with ascites LPA levels >24,000 ng/mL showed significantly worse progression-free survival (PFS) and OS (p < 0.001 in PFS and OS).
Conclusions:
This study demonstrated that LPA levels in plasma and ascites may be useful diagnostic biomarkers for PC of gastric cancer and that higher levels are associated with poor prognosis.
Introduction
P
Materials and Methods
Patients and plasma collection
We enrolled gastric cancer patients diagnosed with PC and after radical surgery at the Xiangya Hospital of Central South University from 2013 to 2014. All the patients were confirmed by histological examination. The disease status of patients was assessed according to the American Joint Commission on Cancer (AJCC)/International Union against Cancer (UICC) TNM classification (7th edition) (Edge and Compton, 2010).
Patients with a history of previous malignancy, autoimmune connective tissue disease, taking antiplatelet drug within 1 month, or uncontrolled infection were excluded from the study.
Control blood samples were collected from healthy volunteers. Negative control ascites samples were collected from patients with liver cirrhosis. Also, positive control ascites samples were collected from patients with ovarian cancer at the same hospital.
Blood samples were collected from venous blood on empty stomach at early morning and stored into EDTA-anticoagulant tubes. Ascites samples collected from patients and controls were stored into dry tubes. Samples were centrifuged at 1,000 g for 10 min within 30 min of sampling and stored at −80°C until analysis.
The study was performed according to the guidelines of the Medical Ethics Committee of the Xiangya Hospital of Central South University in compliance with Helsinki Declaration of 1964 and later versions. All patients gave their signed informed consent.
Assay procedure to determine the levels of LPA
The LPA levels was measured by enzyme-linked immunosorbent assay (ELISA) using a commercial kit (CUSABIO) according to the manufacturer's instructions. Results were expressed in nanograms per milliliter (ng/mL).
Detection of serum tumor markers
Serum levels of carcinoembryonic antigen (CEA) and CA125 before treatment were routinely measured in patients with gastric cancer at Xiangya Hospital of Central South University. Serum CEA levels less than 5 ng/mL and serum CA125 levels less than 35 U/mL were considered to be normal values as per the manufacturer's protocol.
Statistical analysis
Statistical analyses were performed with the Statistical Package for Social Sciences (SPSS) statistical software version 17.0. Continuous data were described using median values (±standard deviation). Mann-Whitney U test or Kruskal-Wallis H test was used for nonparametric comparisons of continuous data. Wilcoxon signed-rank test was used to compare the LPA values in plasma and ascites of the same patient. We used the one-way analysis of variance of repeated measure to compare the LPA levels before and after treatment. Spearman rank correlation analysis was used for evaluation of the correlation between LPA values and patients' clinical pathological data. Kaplan-Meier curves were used to estimate survival outcomes, and comparisons were made using the log-rank test. Multivariate analysis was performed using Cox regression hazard model analysis. p-Values lower than 0.05 were considered statistically significant.
Results
Patient characteristics
Patient demographics and clinical characteristics are summarized in Table 1. The plasma LPA levels statistically correlated with TNM stage and serum CA125 levels (Table 1). Ascites LPA levels did not correlate with any of the patients' clinical pathological factors described above (Table 1).
CEA, carcinoembryonic antigen; LPA, lysophosphatidic acid; PC, gastric cancer patients with peritoneal carcinomatosis; RS, gastric cancer patients who have underwent radical surgery; SRCC, gastric signet-ring cell carcinoma.
Higher plasma LPA level was associated with gastric cancer with PC
Plasma LPA levels were statistically higher in gastric cancer patients with PC than those in gastric cancer patients after radical resection (p = 0.046) and healthy volunteers (p < 0.001, Table 2). Ascites LPA levels were statistically higher in gastric cancer patients with PC and ovarian cancer patients (positive control group) than in liver cirrhosis patients (negative control group) (p < 0.001, Table 2). Plasma LPA levels were higher than ascites LPA levels in the same gastric cancer patient with PC; however, there were no statistical differences (p = 0.069, Table 3).
Values are mean ± SD.
PC, gastric cancer patients with peritoneal carcinomatosis; RS, gastric cancer patients who underwent radical surgery.
Values are mean ± SD.
PC, gastric cancer patients with peritoneal carcinomatosis.
Lower LPA level as an indicator for effective chemotherapy
Plasma LPA levels were statistically lower after chemotherapy in gastric cancer patients with PC (p = 0.028, Table 4). Besides, ascites LPA levels were statistically lower after intraperitoneal chemotherapy injection than before (p < 0.001, Table 4).
Values are mean ± SD.
After IPC, 48 h after intraperitoneal chemotherapy injection; before IPC, before intraperitoneal chemotherapy injection; PC, gastric cancer patients with peritoneal carcinomatosis.
High level of plasma LPA associated with poor overall survival
The median progression-free survival (PFS) was 190 days (95% CI 161.9-411.1 days) and the median overall survival (OS) was 970 days (95% CI 667.6-1090.4 days) for gastric patients with PC whose plasma LPA levels <20,000 ng/mL. However, the median PFS was 150 days (95% CI 43.1-256.9 days) and the median OS was 235 days (95% CI 146.8-323.2 days) for gastric patients with PC whose plasma LPA levels >20,000 ng/mL. Kaplan-Meier PFS curves and OS curves were compared according to the plasma LPA levels in gastric patients with PC (Fig. 1). In this analysis, the plasma LPA levels >20,000 ng/mL group showed significantly worse OS than those of the plasma LPA levels <20,000 ng/mL group (p = 0.006). However, the PFS did not show statistical difference.

Progression-free and overall survival times according to plasma LPA levels. LPA, lysophosphatidic acid.
High level of ascites LPA associated with poor PFS and OS
Kaplan-Meier PFS curves and OS curves were compared according to the ascites LPA levels in gastric patients with PC. In this analysis, the ascites LPA levels >24,000 ng/mL group showed significantly worse PFS and OS than those of the ascites LPA levels <24,000 ng/mL group (p < 0.001 in PFS and OS) (Fig. 2).
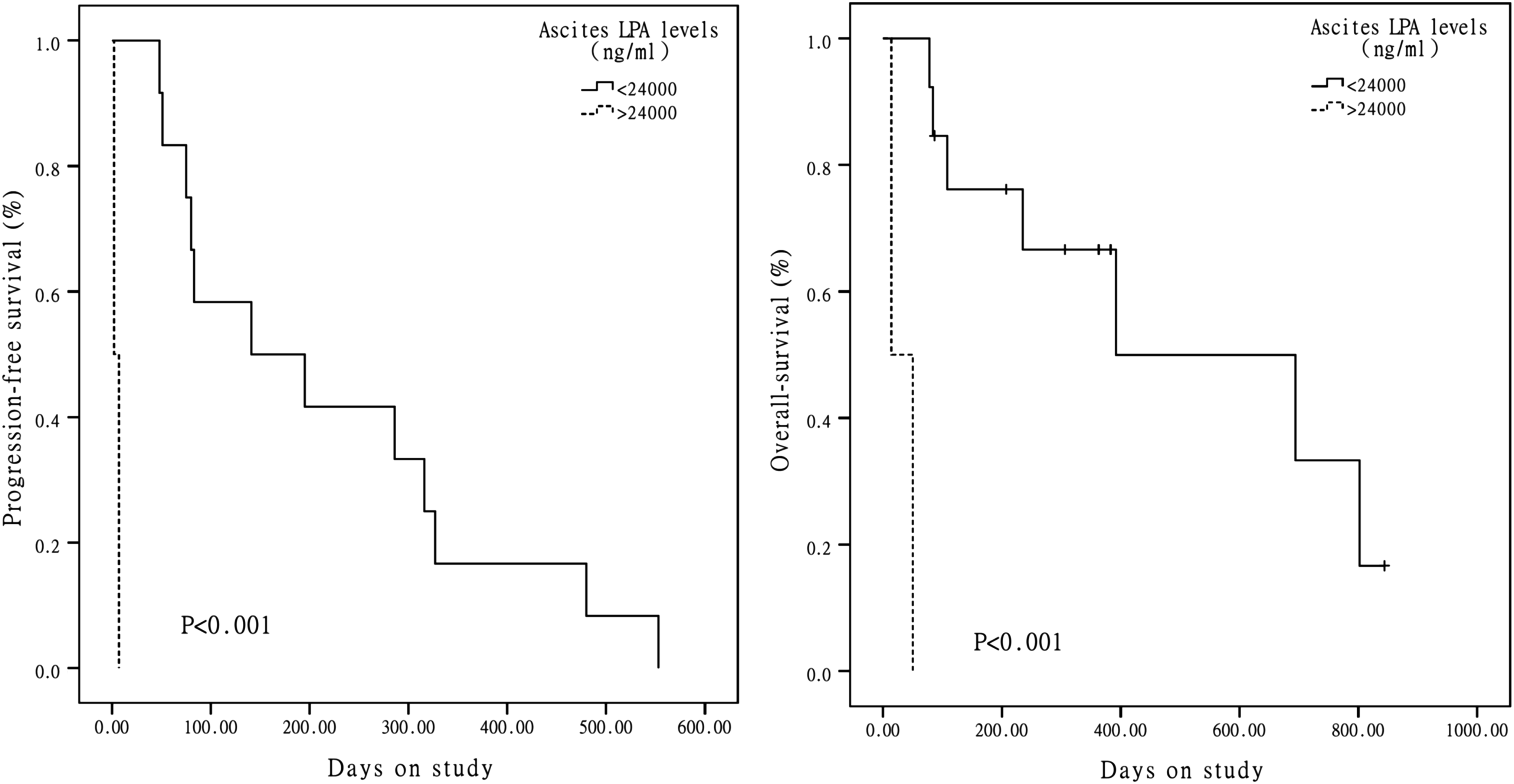
Progression-free and overall survival times according to ascites LPA levels.
Multivariate Cox proportional hazard regression analysis for PFS and OS in gastric cancer patients with PC
According to the Cox regression model, the histologic type (hazard ratio [HR] 63.234, 95% CI 2.938-1360.923, p = 0.008), TNM stage (HR 640336, 95% CI 112.767-3.636 × 109, p = 0.002), serum CA199 levels (HR 0.932, 95% CI 0.889-0.978, p = 0.004), serum CA242 levels (HR 1.226, 95% CI 1.070-1.405, p = 0.003), serum CA125 levels (HR 1.027, 95% CI 1.006-1.049, p = 0.010), plasma LPA levels (HR 1.103, 95% CI 1.043-1.214, p = 0.006), and ascites LPA levels (HR 2.014, 95% CI 1.885-2.416, p = 0.001) were significant independent prognostic factors (Table 5).
CI, confidence interval; HR, hazard ratio; OS, overall survival; PFS, progression-free survival.
Discussion
LPA is a lipid mediator that induces various cell responses through LPA receptors (LPARs). LPA has an important relationship to activated blood platelets (Boucharaba et al., 2004; Yao et al., 2014). Platelets directly and indirectly promote tumor growth, metastasis, and immune evasion (Lange et al., 2008; Goubran et al., 2014; Stegner et al., 2014). As have been reported, LPA induced cell proliferation, migration, and invasion in gastric cancer cells. LPA induces gastric cancer cell migration through LPAR2/Gq/11/p38 pathway in SGC-7901 cells (Yang et al., 2013), and by upregulating the urokinase-type plasminogen activator receptor in human gastric cancer AGS cells (Kim et al., 2008).
Besides, existing evidence suggests that LPA promotes the cancer cell growth and metastatic dissemination in ovarian cancer (Wu et al., 2011; Jeong et al., 2012, 2013), a cancer which also tends toward the development of PC. LPA presents at high levels in ascites of ovarian cancer patients (Mukherjee et al., 2012) and promotes ovarian cancer progression (Ren et al., 2006; Lange et al., 2008).In this study, plasma LPA levels were statistically higher in gastric cancer patients with PC than those in gastric cancer patients after radical resection and healthy volunteers. Ascites LPA levels were statistically higher in gastric cancer patients with PC than in liver cirrhosis patients. High levels of plasma and ascites LPA levels are associated with poor OS. Therefore, LPA acts as a biomarker of PC in gastric cancer.
It was previously shown that serum CEA (Mandorwski et al., 2002) and CA125 (Emoto et al., 2012) are markers in diagnosis of gastric patients with peritoneal dissemination; however, the sensitivity and specificity were questioned. In this study, the plasma LPA levels statistically correlated with serum CA125 levels, but not with serum CEA levels. In serum and plasma, LPA is mainly converted from lysophospholipids, which is irrelevant to serum CEA and CA125.
Endoplasmic reticulum stress, epithelial-to-mesenchymal transition (Okugawa et al., 2013; Lai et al., 2014), CTGF-regulated adhesion (Jiang et al., 2011a; Chen et al., 2015), milky spot macrophages (Liu et al., 2013; Miao et al., 2014), CXCL12/CXCR4 axis (Yasumoto et al., 2011), mesothelial cells (Tsukada et al., 2012; Jiang et al., 2013; Lv et al., 2013), BDKRB2-dependent neovascularization (Jiang et al., 2011b), cancer-associated fibroblasts (Kurashige et al., 2015), HOTAIR (one kind of lncRNA) (Okugawa et al., 2014), microRNA miR-516a-3p (Takei et al., 2011), DJ-1 (Zhu et al., 2014), and c-Met (Wang et al., 2012) play important roles in the development of PC in gastric cancer, although with these mechanisms of research, it is difficult to detect PC noninvasively. Laparoscopic narrow-band imaging (Kikuchi et al., 2014), multimodality imaging consisting of fluorescence imaging with NIR-labeled EGFR or CEA antibody (Ito et al., 2014), and oral 5-aminolevulinic acid-mediated photodynamic diagnosis (Kishi et al., 2012, 2014) could be useful tools for the diagnosis of PC in gastric cancer during staging laparoscopy.
Peritoneal cytology using conventional staining is an important tool for detection of PC; however, the role remains unclear and controversial (Cotte et al., 2013; Mezhir et al., 2013). Therefore, recently, novel approaches of testing peritoneal lavage fluid have made a figure. Tumor cells/leukocytes ratio (Kitayama et al., 2015) and polymerase chain reaction detection of tumor markers in peritoneal lavage fluid (Wong et al., 2012; Fujiwara et al., 2014; Nakabayashi et al., 2015) have been studied as a potential method. Zinc-finger E-box binding homeobox 1 (ZEB1) mRNA levels (Yabusaki et al., 2015), MMP-7mRNA levels (Li et al., 2014), combined analysis of CEA/CA72-4 levels (Yamamoto et al., 2014), combined analysis of CEA/CK20 mRNA levels (Takata et al., 2014; Tamura et al., 2014), CK19 mRNA by reverse RT-LAMP (Yoneda et al., 2014), IMP-3 (one kind of oncofetal protein) mRNA levels (Okada et al., 2012), low IL-17 mRNA expression (Iida et al., 2014), combination expression of CK20, FABP1, and MUC2 (Satoh et al., 2012), and DNA methylation of BNIP3, CHFR, CYP1B1, MINT25, SFRP2, and RASSF2 (Hiraki et al., 2011) in peritoneal lavage fluids from gastric cancer patients were reported to add valuable information to conventional peritoneal washing cytology as a prognostic determinant in gastric cancer. Furthermore, CEA protein (Xiao et al., 2014) in the peritoneal lavage fluids of gastric cancer patients has been reported as an indicator for peritoneal recurrence. In this study, ascites LPA levels were statistically higher in gastric cancer patients with PC and positive control group than in the negative control group.
Furthermore, it has been reported that cytology of peritoneal lavage fluid often changes to negative following combination chemotherapy, including intraperitoneal paclitaxel. Periodic cytological examination of peritoneal lavage fluid is clinically useful to evaluate the efficacy of treatment as well as to predict the outcome of gastric cancer patients with PC (Emoto et al., 2015). In this study, ascites LPA levels were statistically lower after intraperitoneal chemotherapy injection than before. These results suggest that ascites LPA levels were positively correlated with and may be an ideal biomarker of PC in gastric cancer.
No previous observation showed relationship between plasma LPA levels and ascites LPA levels. In our study, plasma LPA levels were statistically same as ascites LPA levels in the same gastric cancer patient with PC.
Taken together, this study showed that the plasma and ascites LPA levels may be useful biomarkers for PC in gastric cancer patients. And higher LPA levels in plasma and ascites correlated with shorter PFS and OS. Further studies with a greater number of patients are required to confirm the diagnostic importance of plasma and ascites LPA levels for PC detection and prognosis. Furthermore, investigating the mechanism that LPA mediates PC in gastric cancer is of great importance.
Footnotes
Acknowledgments
This work was supported by Education Department Foundation of Hunan Province (8749824).
Author Disclosure Statement
No competing financial interests exist.
Ethical Standards
This study was approved by the medical ethics committee of Xiangya Hospital, Central South University (No. 201301012). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964, and later versions. Informed consent or substitute for it was obtained from all patients for being included in the study.