
Abstract
Background:
Birt-Hogg-Dube syndrome (BHDS) is an autosomal dominant disease characterized by hair follicle hamartomas, kidney tumors, and spontaneous pneumothorax; its cause is a heterozygous mutation in the FLCN gene. Colorectal polyps and carcinoma have also been reported in BHDS. FLCN mutations can be detected in patients with isolated primary spontaneous pneumothorax (PSP), so PSP may present as part of BHDS. The aim of this report is to enhance awareness that patients presenting with spontaneous PSP should be evaluated for FLCN mutations.
Materials and Methods:
A 44-year-old woman with PSP and her parents were analyzed for FLCN mutations. One of the patient's paternal aunts had a PSP and two of her paternal aunts had colon cancer diagnosed at early ages.
Results:
A novel in-frame deletion in the FLCN gene, c.932_933delCT (P311Rfs*78), was detected in the proband and in her unaffected father.
Conclusions:
We recommend that molecular analysis of the FLCN gene be performed in patients with PSP and their families, and that mutation carriers be examined for kidney and colon tumors.
Introduction
B
BHDS is caused by a heterozygous mutation in the FLCN gene encoding folliculin (Nickerson et al., 2002). This gene is expressed in lung, kidney, skin, and brain tissues. It is thought to be part of the AMPK (AMP-activated protein kinase) and mTOR (mammalian target of rapamycin) signaling pathway, and to play a role as a tumor suppressor in the kidney (Nickerson et al., 2002; Khoo et al., 2003; Baba et al., 2006). The pathway associated with spontaneous pneumothorax is unclear (Kennedy et al., 2016).
FLCN gene mutations have also been identified in many patients with isolated primary spontaneous pneumothorax (PSP) (OMIM No. 173600). The finding of renal and cutaneous lesions in some of these patients' families suggests that PSP may be a part of BHDS and that renal or skin lesions may develop in BHDS patients. Unaffected individuals carrying FLCN mutations in BHDS families have also been reported. The disease may show intrafamilial clinical variability and incomplete penetrance (Gunji et al., 2007; Toro et al., 2008).
Materials and Methods
Patient data
A 44-year-old woman presented to the Chest Disease Department with a 1-week history of chest pain and dry cough. Her medical history included a right spontaneous pneumothorax 1 year previously, which was conservatively managed, and ex-tobacco use accruing ∼5 pack-years. Her parents were 78-years-old and had no consanguinity. The father was determined to be hypertensive, but had no additional findings. His two sisters had been diagnosed with colon cancer in the fourth decade and another one had a recurrent spontaneous pneumothorax starting at age 20 years (Fig. 1). The mother had type 2 diabetes mellitus. There was no history of renal neoplasms in the family.
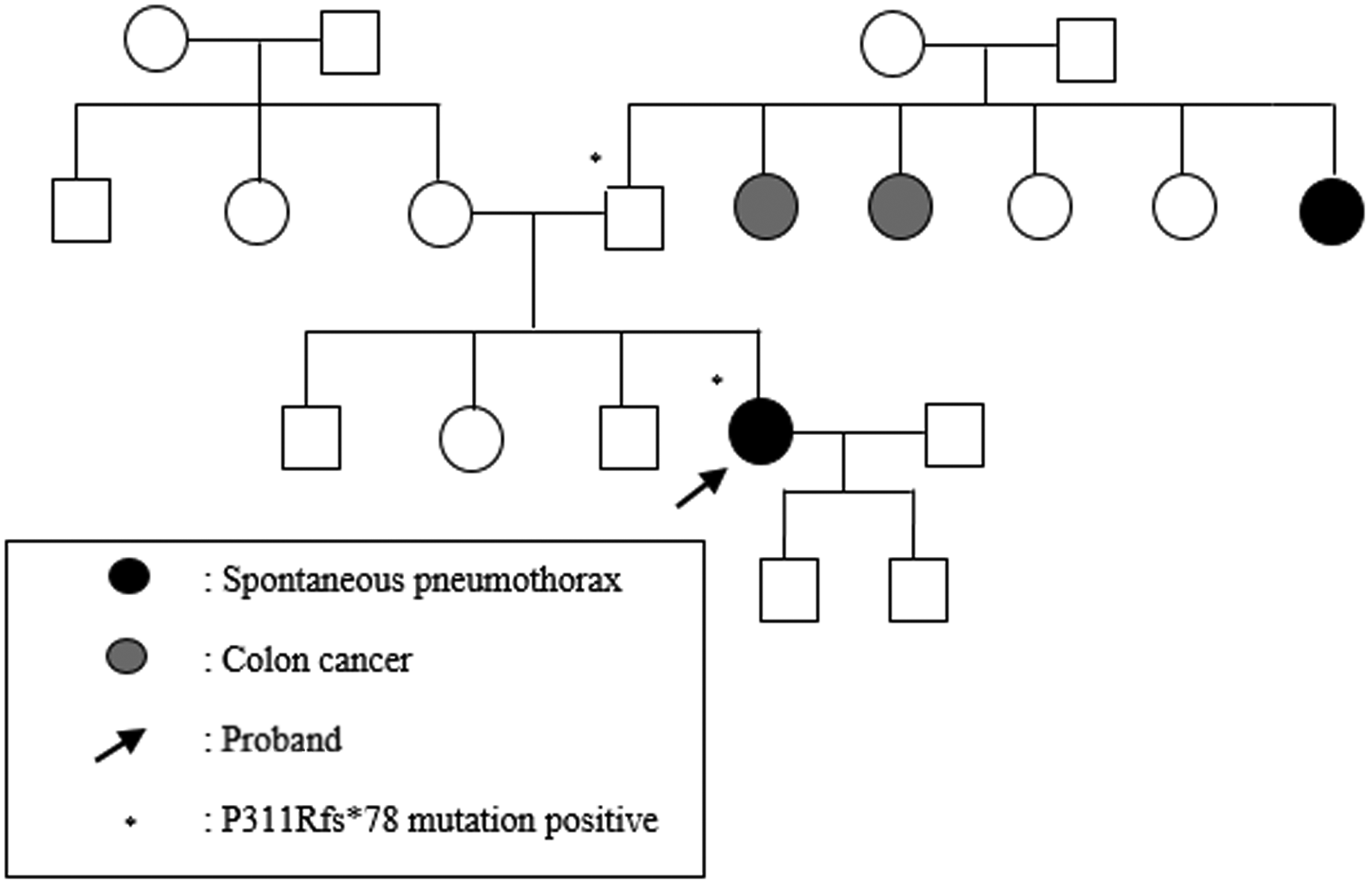
Pedigree of the family.
On examination, the patient's chest revealed hyperresonance and reduced breath sounds over the right lung. She showed no evidence of skin lesions, rheumatic diseases, abdominal masses, or hypertension. A chest X-ray showed a right-sided pneumothorax with nearly complete lung collapse. This was her second episode, so chest drainage was performed, followed by thoracoscopic pleurodesis (Fig. 2). Her chest computed tomography showed multiple bilateral sharply marginated pulmonary cysts. No subdiaphragmatic abnormalities were identified. Bronchoscopy performed for the differential diagnosis of cystic lung disease did not indicate specific pathology. The patient was referred to our Medical Genetics Department for genetic testing. The patient and her parents underwent sequence analysis of the FLCN gene.
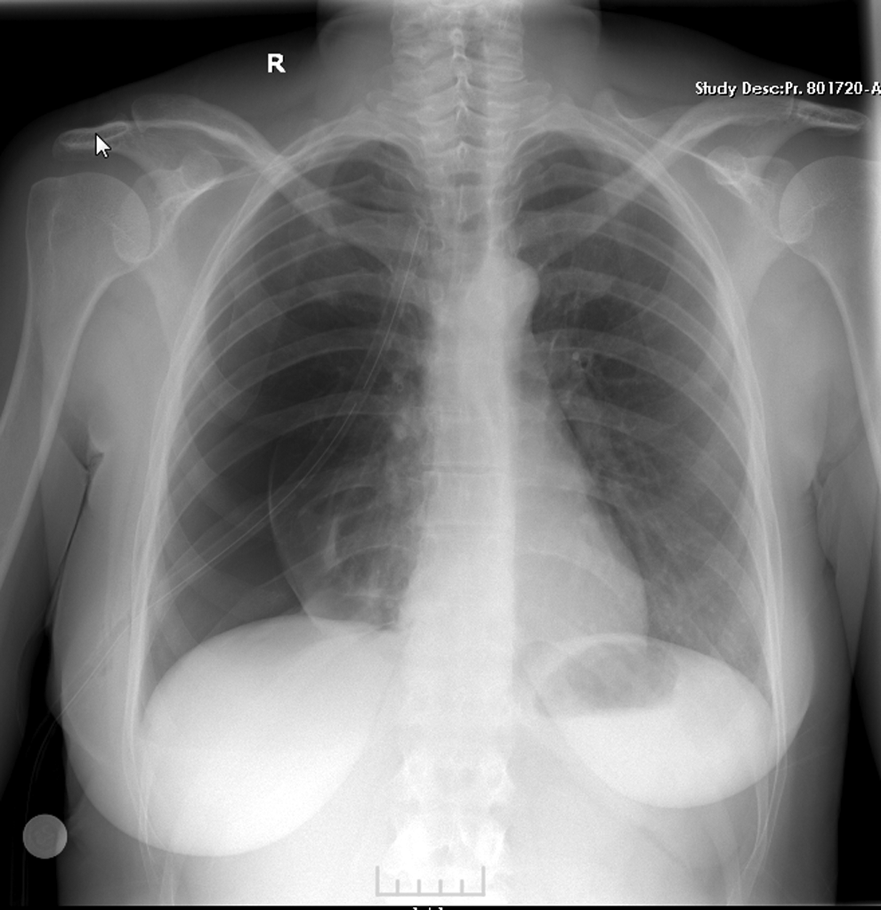
Chest X-ray of the proband showing a right-sided pneumothorax.
Sanger sequencing
The DNA was isolated, with consent, from blood samples from the proband and her parents. Bidirectional DNA sequencing of all the coding exons and flanking intronic regions of the FLCN (OMIM No. 607273) was performed. Sequencing reactions were conducted using a Genetic Analyzer 310 instrument (ABI/Life Technologies). The test could not be done for other likely affected individuals in the family because their DNA was not available.
Results
The DNA sequencing results from both the proband and her father revealed a novel heterozygous mutation in exon 9 of the FLCN gene, c.932_933delCT (NM_144997.5) (ClinVar ID: 373895), which may result in a frameshift mutation p.(P311Rfs*78) (NP_659434) (Fig. 3). The mother's results were normal.

Sequence analysis of the FLCN gene. The chromatograms showing the novel mutation in
Discussion
BHDS is a rare inherited genodermatosis characterized by hair follicle hamartomas, kidney tumors, and spontaneous pneumothorax. In this case, we suspected BHDS in a 26-year-old female who had a spontaneous pneumothorax and a family history of colon cancer.
We found a paternally inherited heterozygous deletion (932_933delCT) in exon 9 of the FLCN gene, which is predicted to result in a frameshift mutation and premature protein termination. The predicted lost amino acid sequence is mostly conserved in other species (Altschul et al., 1990). Based on the criteria of The American College of Medical Genetics and Genomics (Richards et al., 2015), this mutation is highly likely to be deleterious. The father carried the same mutation, but showed no clinical evidence of the disease; however, he has a sister with PSP and two sisters with colon cancer diagnosed at an early age. Protein-truncating mutations in FLCN genes have been identified in both BHDS and PSP families. BHDS is known to show intrafamilial phenotypic variability, and renal or cutaneous lesions have been reported in other family members of patients with isolated spontaneous pneumothorax (Baba et al., 2006; Gunji et al., 2007). In addition, BHDS families may show colorectal polyps and adenomas (Kahnoski et al., 2003). Somatic mutations of FLCN are also associated with colon cancer (Kahnoski et al., 2003; Nahorski et al., 2010). No molecular analyses were performed on the father's sibs, but the family pedigree suggests that the colon cancers and the spontaneous pneumothorax in the aunts may be related to this FLCN mutation.
In conclusion, our results support the contention that BHDS is a disease with intrafamilial variability and incomplete penetrance. Hence, FLCN mutation analysis should be performed in patients with PSP, and affected individuals should be investigated for kidney and colon manifestations of the disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.