
Abstract
Aims:
Cytochrome P450 2C19 (CYP2C19) genotypes are associated with differential drug metabolism. The aim of this study was to establish a reliable assay for CYP2C19 genotyping based on a polymerase chain reaction/ligase detection reaction (PCR-LDR).
Materials and Methods:
Specific primers and probes were designed to detect CYP2C19*1, *2, *3, and *17. A control for each allele was prepared and used for performance evaluation. A total of 200 clinical samples were analyzed using the PCR-LDR assay and Sanger sequencing.
Results:
The detection limit of the PCR-LDR assay was 2 ng/μL of genomic DNA. Common interfering substances in the blood did not affect the results of the detection. For the clinical samples, the results of the PCR-LDR and the Sanger sequencing were identical. Among the 200 patients, 104 (52%) were wild type (*1/*1), 64 (32%) were *1/*2, 16 (8%) were *1/*3, 8 (4%) were *2/*2, 7 (3.5%) were *2/*3, and 1 (0.5%) was *1/*7. No *3/*3 genotype was detected in these patients.
Conclusion:
This PCR-LDR assay is reliable for the detection of CYP2C19 genotypes in a clinical setting. It will be a useful tool to screen for CYP2C19 loss-of-function alleles in patients before clopidogrel and proton pump inhibitor treatment.
Introduction
G
CYP2C19 is responsible for metabolizing commonly used drugs, including clopidogrel, proton pump inhibitors (PPIs), and some antidepressants (Zhou et al., 2009). Patients with the homozygous *1 allele have an active enzyme and are regarded as extensive metabolizers (EMs). Patients with two loss-of-function alleles (*2 or *3) do not express any functional CYP2C19 and are regarded as poor metabolizers (PMs). Individuals with either of the *2 or *3 variants in combination with the *1 allele are considered to be intermediate metabolizers (IMs). Patients with the homozygous *17 allele or the *17 allele in combination with the *1 allele are regarded as ultrarapid metabolizers (Desta, 2002).
Several methods have been used for the detection of CYP2C19 polymorphisms (Hogan et al., 2009; Buchan et al., 2011; Cervinski et al., 2013; Jeong et al., 2014). Although real-time polymerase chain reaction (PCR) methods are simple and easy to perform, at least three assays are needed to detect the *2, *3, and *17 alleles (Jeong et al., 2014). Microarray technologies offer the advantage of allowing the simultaneous detection of various alleles, but these assays are too expensive to be used in resource-limited areas (Buchan et al., 2011). Recently, rapid testing methods for CYP2C19 genotyping have been reported, but the performance of these methods has not been fully evaluated (Marziliano et al., 2015; Wirth et al., 2016).The PCR-ligase detection reaction (PCR-LDR) method has been widely used for the detection of gene polymorphisms (Xu et al., 2011; Zhou et al., 2016). In this method, target DNA sequences were amplified by using a multiplex PCR; then, two specific oligonucleotide probes were ligated when they were completely complemented with the target DNA sequence and no gap existed between the two probes. Because the PCR amplification is sensitive, and the LDR process is specific, PCR-LDR is a sensitive and specific method for detection of DNA polymorphisms. In the current study, we established a PCR-LDR assay for simultaneous detection of the *1, *2, *3, and *17 alleles, and evaluated its performance in a clinical setting.
Materials and Methods
Patients and samples
Whole blood samples were collected from 200 patients who were receiving clopidogrel treatment in Dalian Central Hospital. All of the patients were between 20 and 60 years old, and included 175 men and 25 women. All the samples were stored at −20°C until use.
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and the principles of Good Clinical Practice. All patients gave their informed consent.
Primers and probes
Specific primers and probes were designed to recognize CYP2C19 wild-type (*1), *2, *3, and *17 alleles. At least three sets of primers and probes were tested for each allele and the set with the best performance was selected for the final assay. The primers and probes used in the assay are summarized in Table 1.
PCR, polymerase chain reaction; SNP, single nucleotide polymorphism.
PCR-ligase detection reaction
The process of PCR-LDR is shown in Figure 1. PCR amplifications were carried out in a volume of 50 μL that contained 10 mmol/L Tris-HCl (pH 8.3), 50 mmol/L KCl, 2 mmol/L MgCl2, 200 μmol/L dNTPs, 300 nmol/L for each primer, 1.5 units of Gold DNA polymerase (Qiagen), and 3 μL of DNA template. The amplifications were performed in a PE 9600 Thermal Cycler (Applied Biosystems, Foster City, CA) by heating the samples to 95°C for 10 min, cycling for 35 cycles at 95°C for 30 s, 54°C for 50 s, and 72°C for 60 s, and then performing a final extension at 72°C for 10 min. LDRs were carried out in a volume of 20 μL that contained 20 mmol/L Tris-HCl (pH 7.6), 10 mmol/L MgCl2, 100 mmol/L KCl, 10 mmol/L DTT, 1 mmol/L EDTA, 1 mmol/L NAD+, 12.5 nmol/L each probe, 3 μL of PCR product, and 0.1 mmol/L DNA ligase. The LDR was performed in a PE 9600 Thermal Cycler by incubating the samples at 95°C for 2 min and cycling for 30 cycles at 95°C for 30 s and 65°C for 4 min. The reaction was stopped by adding 0.5 μL of 0.5 mmol/L EDTA. Aliquots of 2.5 μL of the LDR products were mixed with an equal volume of loading buffer containing 80% formamide, 10 mmol/L EDTA, and 1.2% blue dextran. The mixture was denatured at 94°C for 2 min, chilled rapidly on ice before loading on a ABI3130POP-7 gel (Applied Biosystems), and electrophoresed using an ABI 3130 DNA Sequencer (Applied Biosystems) for 30 min. The results were analyzed using GeneMapper software (Applied Biosystems).
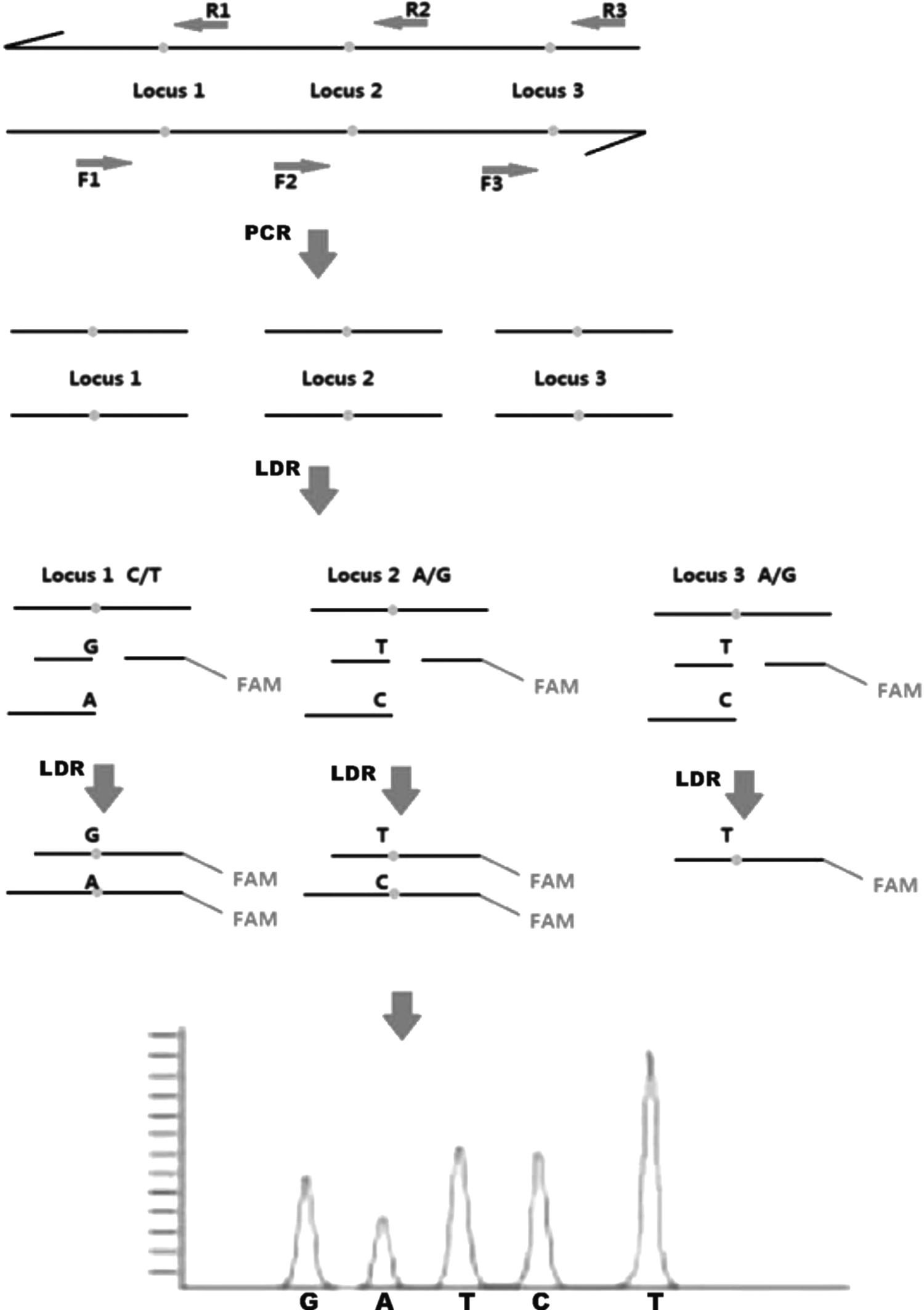
Schematic demonstration of the PCR-LDR assay. PCR-LDR, polymerase chain reaction/ligase detection reaction.
DNA sequencing
DNA sequencing was completed by the Thermo Fisher Company in Shanghai.
Preparation of controls
Genomic DNA from HEK239T cells was used as a control for wild type. Plasmids containing the rs12248560: T, rs2986893: A, and rs4244285: A mutant alleles were mixed with wild-type plasmid (1:1) and served as controls for the *2, *3, and *17 alleles, respectively. All the controls were diluted using fetal bovine serum (FBS) to a working concentration of 10 ng/μL.
Detection limit
Both the controls for wild type and mutant type were diluted using FBS to a concentration of 5 ng/μL, 2 ng/μL, or 1 ng/μL. Each dilution was tested using the PCR-LDR assay 20 times. The lowest concentration at which the controls were detectable was defined as the detection limit.
Precision assessment
Wild and mutant controls were tested in three lots using the PCR-LDR assay. Each control was tested 20 times in each lot.
Anti-interference assessment
Human albumin (50 mg/mL), bilirubin (1.7 μM), hemoglobin (150 mg/mL), triglycerides (1.7 mM), heparin sodium (20 mg/mL), EDTA (2 mg/mL), omeprazole (1.1 mg/L), and clopidogrel (2.5 ng/mL) were added into 2 ng/μL of the mutant-type control and tested using the PCR-LDR assay.
Testing of clinical samples
DNA was extracted from 200 μL of whole blood sample using Whole Blood DNA Extraction Kits (Shanghai Fosun Med-Tech Co., Ltd., Shanghai, China) on an automated DNA extractor (Tibead, Taiwan, China). Extracted DNA was tested using the PCR-LDR assay and Sanger sequencing.
Statistical analyses
Statistical analyses were performed using the Statistical Program for Social Sciences (SPSS 19.0 for Windows; IBM, Corp., Armonk, NY). The differences in the frequencies of genotype distribution were tested by the chi-square test. Statistical significance was defined as a p < 0.05.
Results
Detection limit
The wild-type and mutant-type controls at concentrations of 5 and 2 ng/μL were successfully detected all 20 times. The wild-type control at the concentration of 1 ng/μL could not be detected. Thus, the detection limit of the PCR-LDR assay was 2 ng/μL of genomic DNA. Figure 2 shows the results of the PCR-LDR assay in detecting 2 ng/μL of the mixed controls.

Results of PCR-LDR for the detection of mixed controls.
Precision assessment
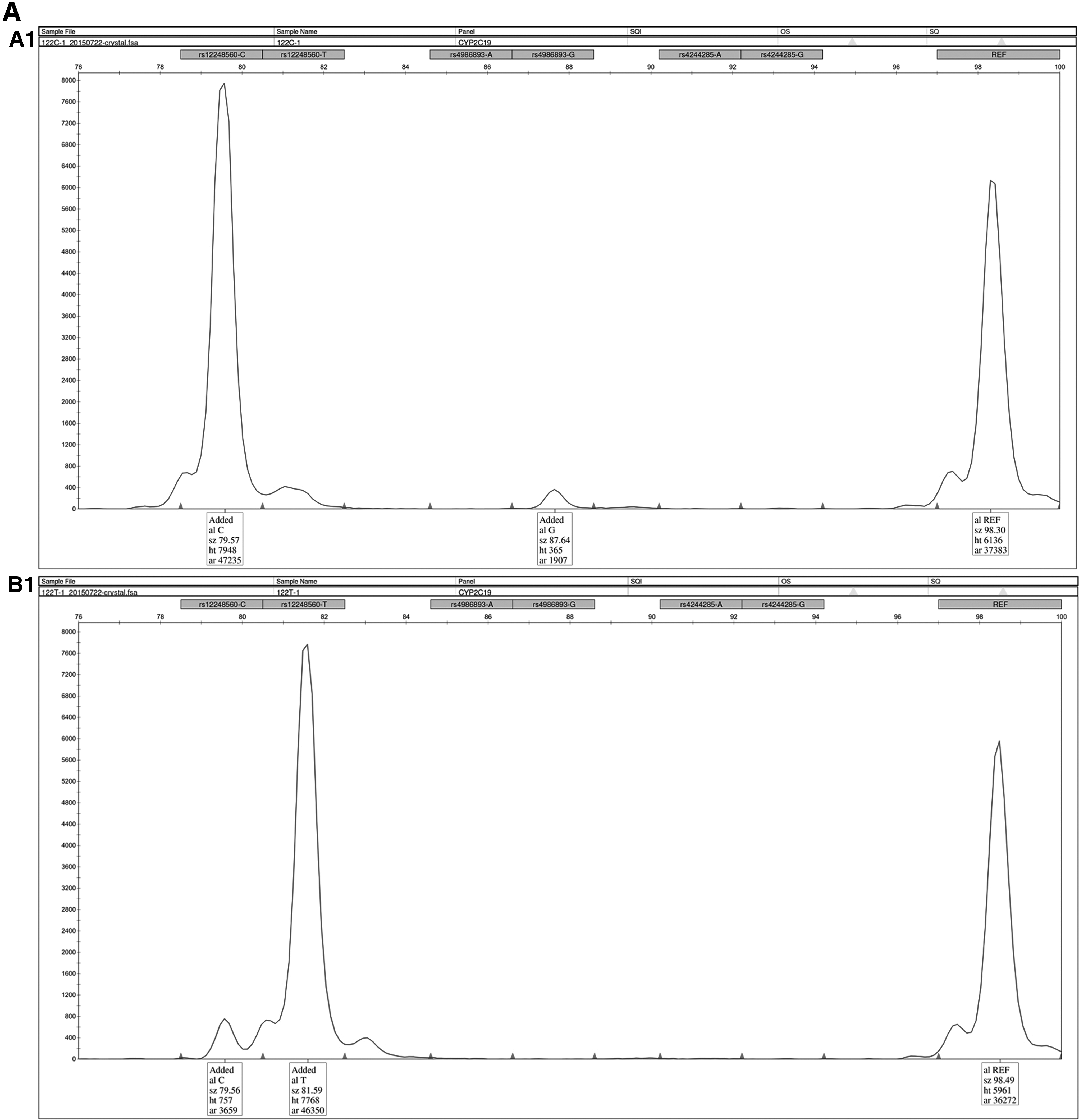
Three different lots of the PCR-LDR assay were used for the precision test. All of the controls were detected correctly in each test. The PCR-LDR and sequencing results for a group of controls are shown in Figure 3A, B.
Anti-interference assessment
When 2 ng/μL of mutant-type control was mixed with human albumin (50 mg/mL), bilirubin (1.7 μM), hemoglobin (150 mg/mL), triglycerides (1.7 mM), heparin sodium (20 mg/mL), EDTA (2 mg/mL), omeprazole (1.1 mg/L), and clopidogrel (2.5 ng/mL), and tested using the PCR-LDR assay, all the mixtures were correctly detected. A typical result of anti-interference experiments is shown in Figure 4.
Typical results of anti-interference experiments.
Analysis of the clinical samples
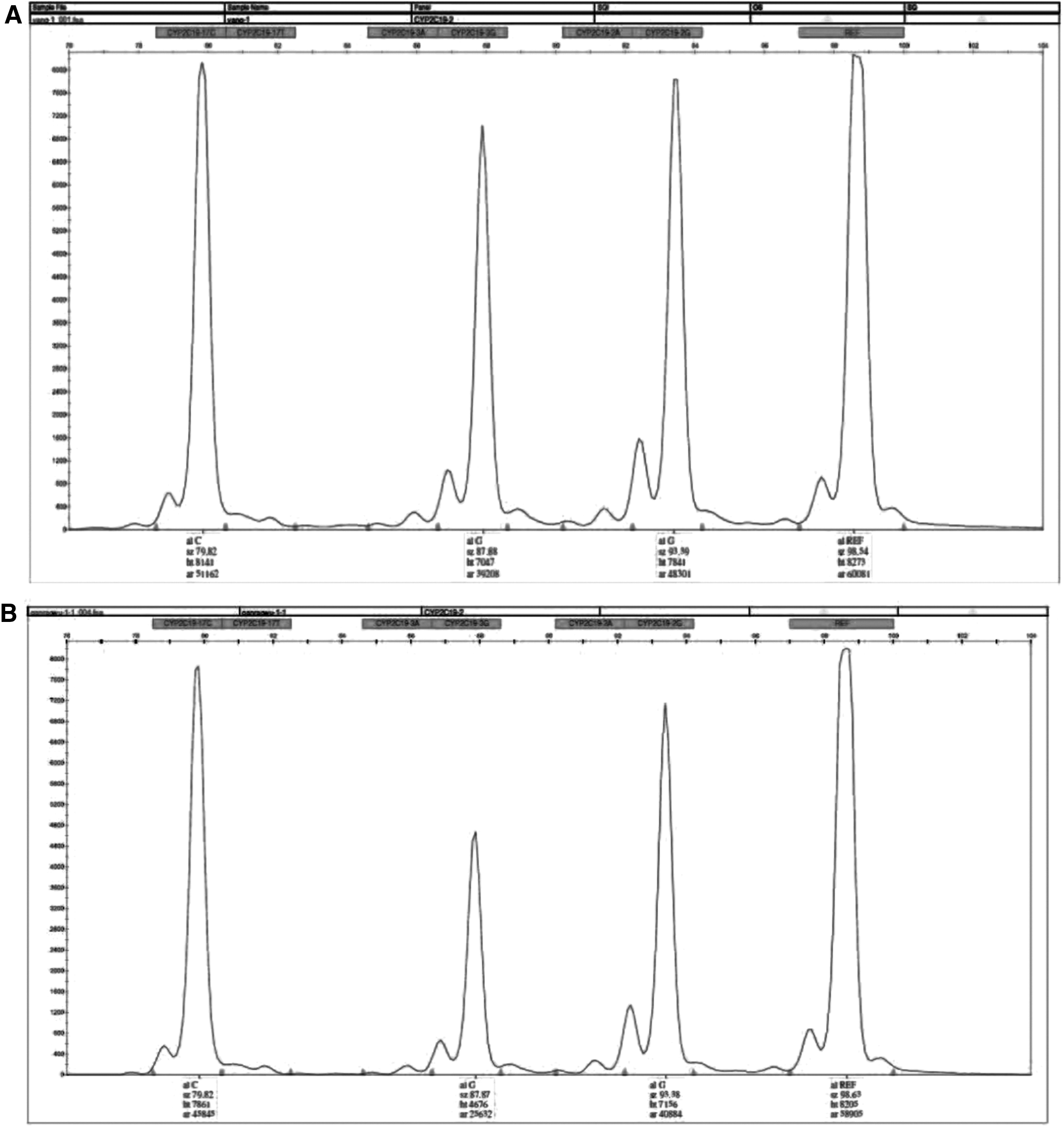
The 200 clinical samples were tested using the PCR-LDR assay and Sanger sequencing. All the results were concordant. Typical PCR-LDR and sequencing results of the samples are shown in Figure 5A, B, respectively. Among the 200 patients, 104 (52%) were wild type (*1/*1), 64 (32%) were *1/*2, 16 (8%) were *1/*3, 8 (4%) were *2/*2, 7 (3.5%) were *2/*3, and 1 (0.5%) was *1/*7. No *3/*3 or *17/*17 genotype was detected in these patients (Table 2). The characteristics and results of the patients are shown in Table 3. There were no significant differences in the distributions of EM, IM, and PM types in different groups of patients (p > 0.05).

LDR, ligase detection reaction.
EM, extensive metabolizer; IM, intermediate metabolizer; PM, poor metabolizer; PCI, percutaneous coronary intervention; SD, standard deviation; UM, ultrarapid metabolizer.
Discussion
CYP2C19 polymorphisms are associated with the differential metabolism of commonly used drugs, including clopidogrel, PPIs, and some antidepressants (Zhou et al., 2009). CYP2C19 genetic testing can identify subgroups of patients who will benefit from those drugs (Hulot et al., 2012). Johnson et al. (2015) estimated the financial impact of CYP2C19 genotyping in patients with acute coronary syndrome (ACS) who received percutaneous coronary intervention and coronary stent implantation and were treated with clopidogrel, prasugrel, or ticagrelor in a managed care setting. They found that genotyping-guided antiplatelet therapy could realize important financial benefits (Johnson et al., 2015). Compared with platelet reactivity testing-guided antiplatelet therapy for patients with ACS undergoing percutaneous coronary intervention, pharmacogenetic-guided therapy was the preferred option, with the lowest cost and the highest quality-adjusted life years gained (Jiang and You, 2016). In the case of PPIs, a meta-analysis has shown that an individualized dosing regimen based on CYP2C19 genotype might be a valid therapeutic strategy to overcome insufficient gastric acid inhibition (Ichikawa et al., 2016). Pharmacogenetic testing to help clinicians in selecting the best management strategy for individual patients has been recommended by several guidelines (Swen et al., 2011; Scott et al., 2013; Yancy et al., 2013). A reliable CYP2C19 genotyping assay would be helpful for decision-making before or during antiplatelet and PPI therapies. In the present study, we have established a reliable CYP2C19 genotyping assay based on PCR-LDR technology. This assay correctly detected different alleles and has a good anti-interference capability for common interfering substances in blood and common drugs.
One of the advantages of PCR-LDR is the capability to detect multiple single nucleotide polymorphisms in a single assay. In the current study, CYP2C19*1, *2, *3, and *17 alleles were detected in one assay with good performance. Compared with real-time PCR and point-of-care testing, this PCR-LDR assay detected all of the common variations of CYP2C19 related to drug metabolism in a single assay. This will simplify genotype testing and reduce its cost. Compared with DNA arrays, this PCR-LDR was more reliable and cheaper.
A total of 200 patients were tested using the PCR-LDR assay and Sanger sequencing. The results were identical between the two methods. Among those patients, 52% were CYP2C19*1/*1, 32% were *1/*2, 8% were *1/*3, 4% were *2/*2, 3.5% were *2/*3, and 0.5% were *1/*7. No *3/*3 or *17/*17genotype was detected. These results are similar to those of previous studies and meta-analysis results concerning Asian patients (Niu et al., 2015; Guo et al., 2016; Mao et al., 2016). Nearly half of the Chinese patients carry at least one of the loss-of-function alleles of CYP2C19. Those patients are PMs or IMs for drugs such as clopidogrel and PPIs. It is necessary for Chinese people to be screened for CYP2C19 alleles before they are treated with such drugs.
In conclusion, we have established a reliable PCR-LDR assay for the detection of CYP2C19 genotypes. It will be a useful tool for screening loss-of-function alleles of CYP2C19 in patients before clopidogrel and PPI treatment.
Footnotes
Acknowledgments
We would like to sincerely give our gratitude to Mr. P. X. Jiang for his constructive comments.
Author Disclosure Statement
No competing financial interests exist.