
Abstract
Background:
The protein AXIN2 is involved in the negative feedback regulation of the Wnt/β-catenin signaling pathway; it functions by promoting β-catenin degradation. AXIN2 mutations have been studied in various cancers. In this study, we genotyped three single nucleotide polymorphisms in the AXIN2 gene and investigated their association with the risk of breast cancer (BC) in the Chinese Han population.
Methods:
In a population of 415 BC patients and 528 controls the expression of AXIN2 was measured using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry and compared with the overall survival (OS) of BC patients analyzed through Oncomine and Kaplan-Meier plotter databases. Bioinformatic analyses demonstrated that AXIN2 mRNA levels were downregulated in BC patients; this in turn correlated with a poorer survival rate for BC patients.
Results:
The polymorphisms rs11079571 and rs3923087, but not rs3923086, were associated with an increased risk of BC. The minor allele containing genotypes of polymorphism rs3923087 were positively associated with lymph node metastases. A haplotype analysis demonstrated that the ATA haplotype was correlated with an increased risk of BC.
Conclusion:
In conclusion, the downregulation of AXIN2 is related to poorer OS for BC patients. Its polymorphisms rs11079571 and rs3923087 confer susceptibility to BC. These findings should be confirmed with larger studies that include more diverse ethnic populations.
Introduction
Breast cancer (BC) is the world's most frequently occurring cancer in women and has become a major public health concern (Tao et al., 2015). In 2017, about 255,180 new BC cases and 41,070 BC deaths were reported for women in the United States (Siegel et al., 2017). Evidence demonstrates that those with a high body mass index, low education level, low fruit intake, and sedentary lifestyles could be at risk for BC (Fu et al., 2015). Genetic risk factors also play important roles in the pathology of BC, whereas the most BC-linked genes recognized thus far are BRCA 1/2 (Lynch et al., 2015).
The Wnt/β-catenin signaling pathway reportedly contributes to human tumor progression (Polakis, 2007). AXIN2/Conductin/Axil are negative regulators of the Wnt signaling pathway, and promote the phosphorylation and degradation of β-catenin (Jho et al., 2002). An AXIN2-null mice model presented high susceptibility to cancers after exposure to carcinogenic matter (Aristizabal-Pachon et al., 2015). The AXIN2 gene, located on chromosome 17q24.1, has 15 exon counts. Mutation in the AXIN2 gene may lead to different cancers due to the increased transcription of Wnt target genes (Liu et al., 2000, 2014). Moreover, AXIN2 gene polymorphisms (rs11079571, rs3923087, and rs923086), whose minor allele frequencies are >0.05 in the dbSNP database, have been studied in various diseases, such as ovarian cancer (Mostowska et al., 2014), papillary thyroid carcinoma (Liu et al., 2016), and tuberculosis (Zhou et al., 2016). However, they were less studied in BC. Few studies reported the association between three AXIN2 gene polymorphisms (rs11079571, rs3923086, and rs3923087) and BC development in various ethnicities, and no consistent conclusion reached (Wang et al., 2008; Alanazi et al., 2013). None similar studies had even been published in Chinese populations. Therefore, this case-control study was conducted to evaluate the association of three AXIN2 gene polymorphisms with the risk of BC along with the clinicopathological features of BC in Chinese participants.
Patients and Methods
Study subjects
In total, this study included 415 BC patients, who were treated at the Affiliated Changzhou No. 2 People's Hospital of Nanjing Medical University, between August 2012 and January 2017. All patients signed a free informed consent form before their participation, and all procedures were conducted in accordance with the approval standards of the ethics committee from the hospital. No patient received chemotherapy or radiotherapy before surgery. Pathological tumor staging and grading were further evaluated according to the tumor node metastasis (TNM) classification. Demographic data on sex and family history were obtained from a standardized questionnaire. Information regarding the estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) were also collected from patient medical records.
In addition, 528 healthy controls who had a checkup at the same institution during the same time period were recruited. None of the controls had an autoimmune or inflammatory bowel disease or a history of cancer. After the questionnaire was provided, 5 mL of peripheral blood was then collected from each subject.
Oncomine analysis
The AXIN2 mRNA levels between BC and normal breast issues were analyzed on Oncomine—(Mangogna et al., 2018; Zhu and Dong, 2018), a cancer microarray database and web-based data mining platform, which integrates RNA and DNA data from sources such as Gene Expression Omnibus, The Cancer Genome Atlas (TCGA), and published literature. The search parameters were AXIN2; analysis type: cancer versus normal analysis; cancer: breast cancer; sample type: clinical specimen; and data source: TCGA breast.
The Kaplan-Meier plotter
The prognostic significance of the AXIN2 expression (high vs. low expression) and survival in BC patients was analyzed by the Kaplan-Meier plotter (Gyorffy et al., 2010). The hazard ratios (HRs) with 95% confidence intervals (CIs) and log-rank p-values were additionally computed.
Isolation of DNA and genotyping
Genomic DNA from the peripheral blood was isolated using a QIAamp DNA blood mini-kit (Qiagen, Hilden, Germany) according to the manufacturer's instructions. The concentration and purity of DNA were determined at a 260/280 nm using a NanoDrop instrument. Genotyping was conducted by a matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOFMS), which was examined by using a MassARRAY system (Sequenom, San Diego, CA). Completed genotyping reactions were further spotted onto a 384-well spectroCHIP system (Sequenom) using a MassARRAY nanodispenser (Sequenom) and was then analyzed by MALDI-TOFMS. Genotypes were called in real time with MassARRAY RT 3.1 and analyzed on MassARRAY Typer 4.0 (both Sequenom). About 5% of the samples were randomly selected for a blinded retest.
Quantitative real-time reverse transcription polymerase chain reaction
The 60 BC patients were selected from the case group (with 20 patients of each genotype). The total RNA of each participant was extracted from peripheral blood using a Qiagen RNA extraction kit (Qiagen, Germany). The mRNA was reverse transcribed into a cDNA by using an oligo primer and SuperscriptII (Invitrogen). Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was chosen as an internal reference gene. The primers used for reverse transcription-polymerase chain reaction (RT-PCR) were as follows: AXIN2, 5′- CACGGAAACTGTTGACAGTGGATAC-3′ (forward), and 5′- GGTGGCTGGTGC AAAGACATAG-3′ (reverse); GAPDH, 5′- GCACCGTC AAGGCTGAGAAC-3′ (reverse); and 5′- GTGA AGACGCCAGTGGA-3′ (reverse). Gene expression levels were then normalized to that of GAPDH, whereas fold changes were calculated using the 2−δδCT method.
Statistical analyses
Differences of clinical characteristics between groups were evaluated using either a Student's t-test or chi-squared test. The Hardy-Weinberg equilibrium (HWE) was tested by comparing the observed and expected genotype frequencies in the control group using a goodness-of-fit chi-squared test. Odds ratios (ORs) and 95% CIs were calculated to estimate the strength of the association between the AXIN2 gene polymorphisms and the risk of BC by logistic regression analyses. To account for multiple comparisons, a false discovery rate was applied according to the Benjamini-Hochberg procedure (Hochberg and Benjamini, 1990). The statistical significance of the correlation between polymorphisms and clinicopathological parameters was examined through a chi-squared test and analysis of variance (ANOVA). All statistical analyses were performed on a SAS package 9.1.3 (SAS Institute, Cary, NC). p < 0.05 was furthermore considered to be significant.
Results
Oncomine analysis and prognosis analysis
AXIN2 gene mRNA levels in BC were investigated using the Oncomine database (Fig. 1). Three types of BC (invasive, invasive ductal, and invasive lobular) with a larger sample size may present more reliable data. Overall, AXIN2 gene levels were downregulated in all types of BC compared with normal breast issues.

AXIN2 gene expression analysis in breast cancer (Oncomine database). X-axis represents normal (left plot) and cancer tissue (right plot). Y-axis represents the median intensity, 10th and 90th percentile data.
The association between a participant's AXIN2 gene expression overall survival (OS) was evaluated using a Kaplan-Meier plotter. Survival curves were then plotted for all patients (Fig. 2). A higher AXIN2 expression in a subject was related to a higher OS rate (HR = 0.64; 95% CI = 0.53-0.77; p = 3.0 × 10−6). We hypothesize that AXIN2 is a tumor suppressor gene. This hypothesis will, however, require further examination with future studies.
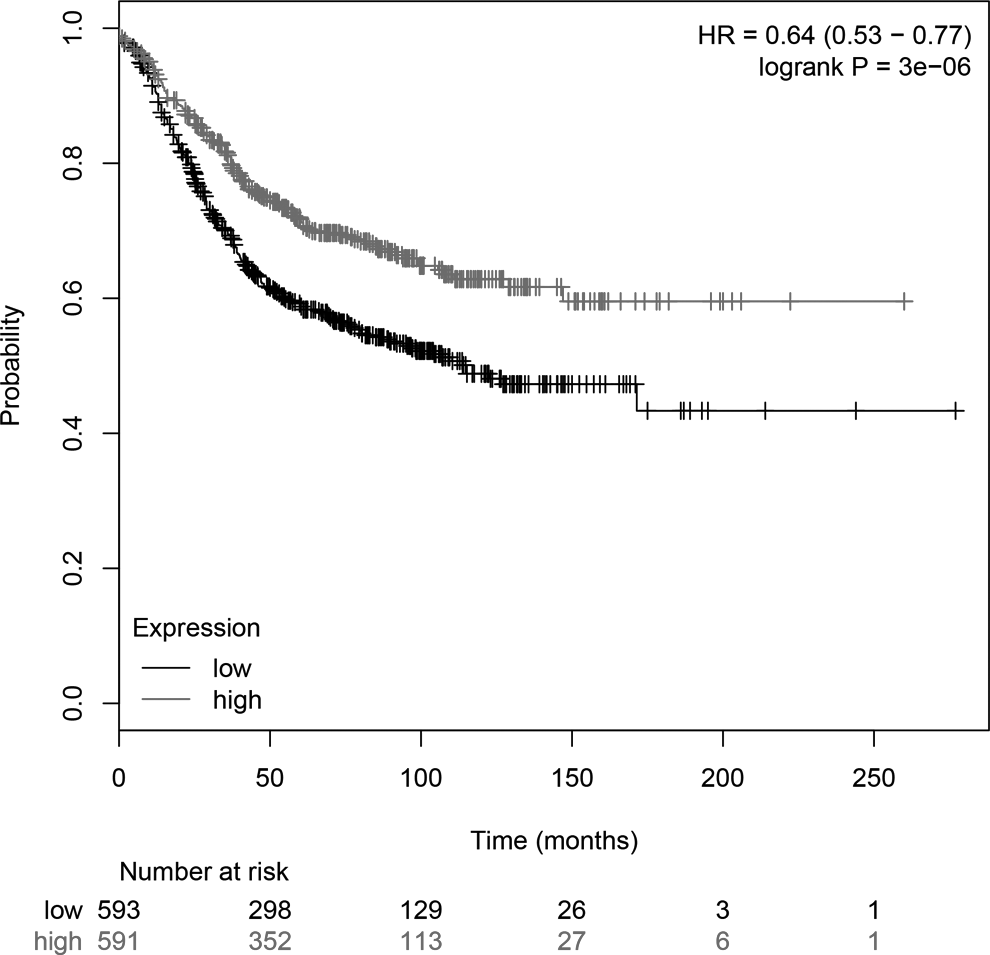
The prognostic value of AXIN2 expression (high expression vs. low expression). Survival curves were plotted using the Kaplan-Meier plotter.
Characteristics of the study population
The baseline characteristics and description of the study population as well as other clinical parameters (e.g., ER, PR, HER2 status, lymph node metastasis, and TNM classification) are shown in Table 1. The 415 BC patients and 528 healthy controls were adequately matched for age and for a family history with cancer (both p > 0.05). There were no significant differences with regard to the menopausal status, drinking, and smoking. Those with BC were mainly enriched with invasive ductal carcinoma (44.6%), invasive lobular carcinoma (32.3%), and papillary carcinoma (18.5%).
Patient Demographics and Risk Factors in Breast Cancer
HER2, human epidermal growth factor receptor 2; TNM, tumor node metastasis.
Quantitative analysis
The genotypes and allele distributions of AXIN2 gene polymorphisms (rs11079571, rs3923087, and rs3923086) between BC patients and healthy controls are provided in Table 2. No significant deviation from HWE was found in any single nucleotide polymorphism (SNP) between participants with BC and control subjects (all p > 0.05), which further suggests that these controls could represent the total population of South China. The AA genotype versus the GG genotype of polymorphism rs11079571 was significantly associated with a 1.72-fold increased risk of developing BC (AA vs. GG: OR = 1.72, 95% CI = 1.03-2.89, p < 0.05). This significant association was also found in the dominant and allelic models (both p < 0.05). Similarly, polymorphism rs3923087 has been associated with an increased risk of BC in the homozygous and allelic models (both p < 0.05). Polymorphism rs3923086, however, was not significantly associated with the risk of BC in any of the five models. Notably, three SNPs were not significant after adjusting for multiple testing using the Bonferroni correction (p > 0.05).
Genotype Frequencies of AXIN2 Gene Polymorphisms in Cases and Controls
Bold values are statistically significant (p < 0.05).
p (FDR) values were calculated with FDR.
CI, confidence interval; FDR, false discovery rate; OR, odds ratio.
Stratified analyses were further conducted according to a participant's age, smoking, drinking, menopausal status, and family history with cancer (Table 3). The significant association between AXIN2 rs11079571 polymorphism and the risk of BC appeared stronger in the subgroups of premenopausal women and subjects with age ≥50. The increased risk of AXIN2 rs3923087 polymorphism in those with BC was more evident among premenopausal women, smokers, nondrinkers, and subjects with an age of <50.
Stratified Analyses Between rs11079571/rs3923087 Polymorphisms and the Risk of Osteoarthritis
Bold values are statistically significant (p < 0.05).
We proceeded to analyze the associations between polymorphism rs11079571 or rs3923087 along with the clinical characteristics of BC (Table 4). Results have shown that the TT genotype versus the CC genotype of rs3923087 increased lymph node metastasis in BC patients (Table 4). Furthermore, all three SNPs were located in one haplotype block (Fig. 3). Haplotype analysis suggested those with an ATA haplotype was more likely to develop BC (Table 5). We have further investigated the expression levels of AXIN2 in different genotypes of two polymorphisms using the RT-PCR method. Our results indicate that the AXIN2 expression level of AA genotype of rs11079571 polymorphism is significantly lower than the GG genotype (Fig. 4). A similar result was observed for rs3923087 (Fig. 4).

Linkage disequilibrium of the five SNPs in AXIN2 gene. SNP, single nucleotide polymorphism.
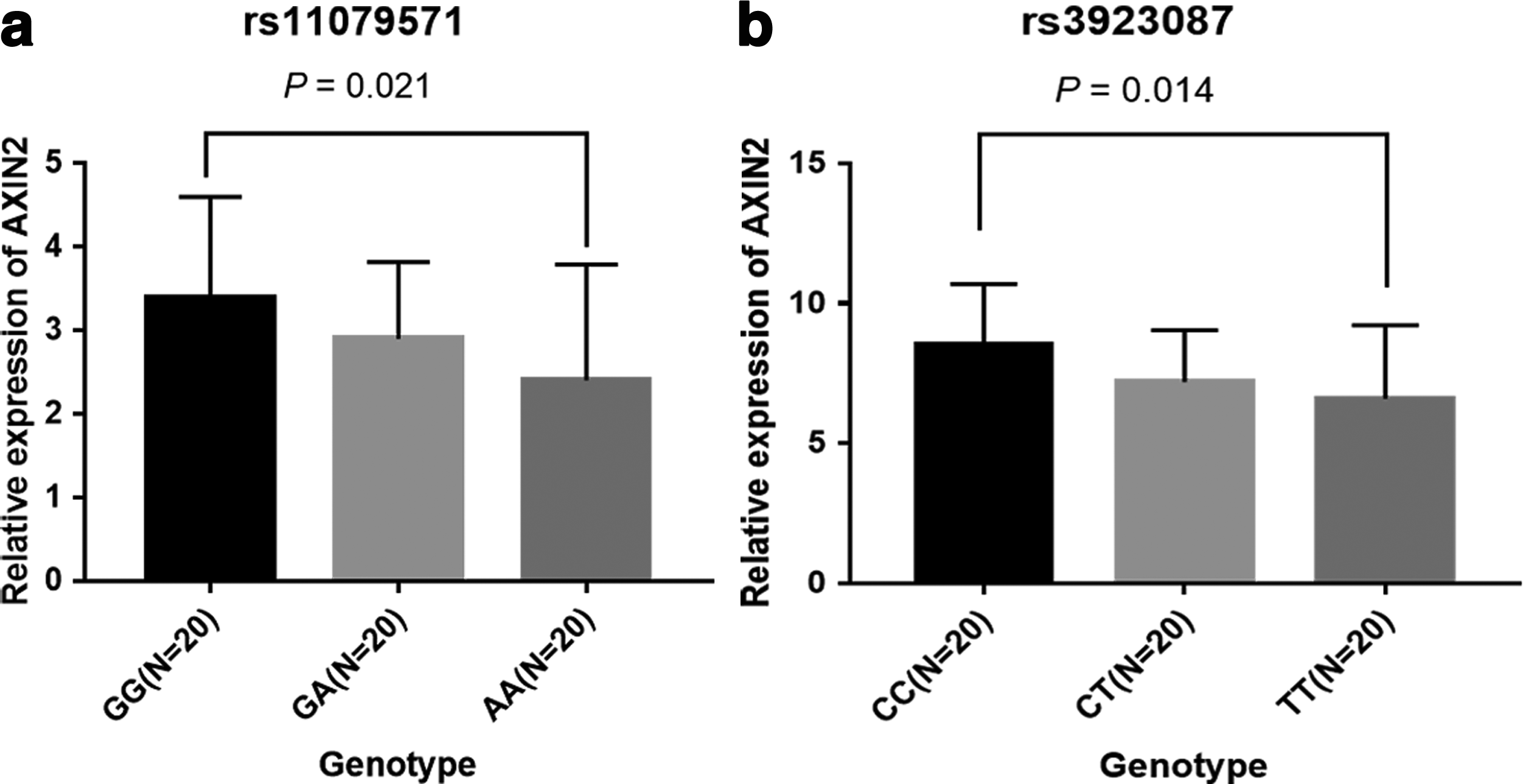
The relative expression of AXIN2 in BC patients.
The Associations Between AXIN2 rs3923087 Polymorphism and Clinical Characteristics of Breast Cancer
Bold values are statistically significant (p < 0.05).
ER, estrogen receptor; PR, progesterone receptor.
The Haplotype Frequencies of AXIN2 Gene Polymorphisms and Risk of Breast Cancer
Bold values are statistically significant (p < 0.05).
Discussion
Bioinformatics analysis suggests that the AXIN2 gene is downregulated in BC patients, and associated with a lower chance of OS. In addition, AXIN2 gene polymorphisms (rs11079571 and rs3923087) were associated with an increased risk of BC. The TT genotype of polymorphism rs3923087 was correlated with lymph node metastasis among BC patients.
The AXIN2 expression is elevated in cancer with activating Wnt/β-catenin (Mazzoni and Fearon, 2014). AXIN2 gene polymorphisms play a large role in tumorigenesis along with dysregulation in cancer cells (Pinarbasi et al., 2011). AXIN2 gene polymorphisms (rs11079571, rs3923087, and rs3923086) were associated with an increased risk of BC in a Minnesota population with 798 cases and 843 controls (Wang et al., 2008). However, no significant association between AXIN2 polymorphisms rs11079571 or rs3923086 and risks of developing BC were found in a Saudi population (99 cases and 93 controls) (Alanazi et al., 2013). For rs3923087, the AG genotype but not GG genotype, was significantly correlated with a decreased risk of BC. Our study has indicated that AXIN2 polymorphisms rs11079571 and rs3923087, but not rs3923086, conferred susceptibility to BC in a Chinese population (with a total number of 412 cases and 528 controls). Our findings are similar to the results of Wang et al. (2008) but not Alanazi et al. (2013). The reason for this conflict may be that the sample size of the study from Alanazi et al. (2013) (99 cases and 93 controls) was not large enough to reach a convincing conclusion. A significant association between AXIN2 polymorphism rs3923086 and an increased risk of BC, found by Wang et al. (2008), was not identified in our study. A possible explanation for this concerns the ethnicity-specific effect of rs3923086. The allele frequency of the AXIN2 polymorphism differs among ethnic groups, as the C allele frequency in Caucasians is higher than in Asians (0.414 vs. 0.289). Furthermore, different genotyping methods, diet habits, and random errors may also explain the differences in findings between Asians and Caucasians.
AXIN2 is known as a tumor suppressor gene. Hu et al. (2016) has found that low AXIN2 is related to more aggressive prostate cancer, biochemical recurrence, and metastasis-free survival after radical prostatectomy. Few studies, however, have thrown light on the role of AXIN2 in the development of BC. Based on Hu et al.'s study, we have investigated the expression of AXIN2 in BC and its relationship with BC prognosis using the Oncomine database along with the Kaplan-Meier plotter. The bioinformatics analysis indicates that the downgrading of AXIN2 is harmful to the survival of BC patients, which was in accordance with the study conducted by Hu et al. AXIN2 expression levels have been confirmed by RT-PCR. However, a long-term follow-up of BC patients should be used to verify the relationship between high/low expression of AXIN2 and BC prognosis. AXIN2 in BC may be a potential marker of BC prognosis if the aforementioned findings are confirmed in the future. The three SNPs were all located on the intron region of AXIN2 gene, and thus the functional significance was unclear. Our results have shown that AXIN2 polymorphism rs3923087 increases the risk of an individual developing BC. This further reflects the linkage disequilibrium with another potential functional variant or the close link with an individual's susceptibility gene (Hu et al., 2016).
Several limitations of this study need to be addressed. The first includes authenticity not being validated in the database, despite the fact that expression and survival data of AXIN2 being collected. Second, this study's sample size was not sufficiently large, which provides for limited generalizability. Third, our findings were based on unadjusted estimates for confounding factors, which might have affected this study's overall results. Fourth, selection bias could not be avoided in this hospital-based case-control study. And finally, we cannot add the experimental results in vivo and in vitro due to this study's limited experimental conditions.
In sum, AXIN2 gene polymorphisms confer susceptibility to BC by altering the expression levels of AXIN2. Expression data and survival data of AXIN2 were, however, validated by this study's experiments. AXIN2 in BC, furthermore, may be a potential marker of BC prognosis if the aforementioned findings are confirmed in further findings.
Footnotes
Acknowledgment
This study was supported in part by Nanjing Medical University Science and Technology Development Fund (2016NJMUZD082).
Author Disclosure Statement
No competing financial interests exist.