
Abstract
Background:
Involvement of interferon regulatory factor 6 (IRF6) gene polymorphisms in nonsyndromic cleft palate (NSCP) risk remains controversial. This investigation was performed to evaluate the relationship between IRF6 gene polymorphisms and NSCP risk.
Materials and Methods:
Two hundred forty-one patients with NSCP (including 103 complete trio families) were recruited, and 242 unaffected individuals were included as controls. Polymorphisms for the IRF6 rs2235371, rs801619, rs642961, rs44844880, and rs8049367 loci were characterized in both groups. Furthermore, eligible studies were identified from the databases through June 1, 2017, and were included in a meta-analysis to enhance the robustness of our conclusions.
Results:
The IRF6 rs2235371 A allele and AA genotype in the case group were found at higher frequencies than in the control group (A allele: p < 0.0016; AA genotype: p < 0.0049). The IRF6 rs801619 AA genotype and G allele were associated with NSCP risk (G allele: p < 0.0061; AA genotype: p < 0.0195). At the IRF6 rs642961, rs44844880, and rs8049367 loci genotype and allele frequencies were not statistically different between the NSCP group and normal controls. In the meta-analysis, the IRF6 A/G gene polymorphism (rs2235371) and IRF6 A/G gene polymorphism (rs642961) were associated with NSCP risk in the general population, whereas the IRF6 A/C gene polymorphism (rs2013162) was not.
Conclusion:
The IRF6 A/G gene polymorphisms at rs2235371 and rs642961, but not the IRF6 A/C gene polymorphism rs2013162, were associated with NSCP risk.
Introduction
Nonsyndromic cleft palate (NSCP) is one of the most common congenital craniofacial deformities, accounting for about 33% of cleft lips and palates (Stanier and Moore, 2004; Zhou et al., 2013). The etiology of cleft palate is complex and largely unknown, but is currently believed to be mainly caused by both genetic and environmental factors and their interaction (Stanier and Moore, 2004; Zhou et al., 2013). The development of the palate is a programmed event that includes the expression of genes, regulation of transcription, and the participation of related factors (Meng et al., 2009). Interference of palatal fusion can lead to cleft palate if the tight regulatory network is disturbed (Stanier and Moore, 2004). There have been attempts to identify disease genes associated with nonsyndromic cleft lip with or without cleft palate (NSCL/P), as identification of disease genes may shed light on the etiology of the condition and facilitate efforts at prevention of the disease (Zucchero et al., 2004; Srichomthong et al., 2005).
Interferon regulatory factor 6 (IRF6) is a key element in oral and maxillofacial development, and the IRF6 gene is located on chromosome 1q32.3-q41, and has been strongly associated with oral-facial cleft risk (Birnbaum et al., 2009). Gene polymorphisms are reported to be involved in the pathogenesis of some diseases (Ratheesh et al., 2018; Xia et al., 2018; Zhou et al., 2018a, 2018b). Mutations in the IRF6 gene are associated with autosomal-dominant Van der Woude syndrome, which has the cardinal signs of cleft lip with or without cleft palate (CL/P) and/or cleft palate only (CPO) with dental anomalies and pitted lips (Richardson et al., 2009), and rs2013162 and rs2235375 polymorphisms are associated with NSCL/P in an Italian population (Scapoli et al., 2004). Srichomthong et al. (2005) suggested that IRF6 rs2235371 (V274I) is responsible for 16.7% of the genetic contribution to CL/P, and large studies in different populations have provided further evidence that IRF6 is important in the etiology of NSCL/P (Egger et al., 1997; Jugessur et al., 2008).
IRF6 gene polymorphisms were later identified by (Zucchero et al., 2004), and subsequently in both studies of individuals and genome-wide association studies, to be associated with NSCL/P (Zucchero et al., 2004; Ali et al., 2009; Birnbaum et al., 2009; Pan et al., 2010; Paranaíba et al., 2010). Animal studies also indicate that IRF6 is involved in proliferation and differentiation of keratinocytes (Richardson et al., 2009), and hyperproliferation of the epidermis may result in failure of terminal differentiation and multiple epithelial adhesions leading to CL/P (Carter et al., 2010; Shi et al., 2011).
Several independent studies have replicated the effects of IRF6 gene polymorphisms, at rs2235371 and rs642961, on NSCL/P, and their effects were later pooled by a meta-analysis (Wang et al., 2012). However, we perform a meta-analysis to include more studies to extend the robustness of the polymorphism data.
Materials and Methods
Patient samples
This study was approved by the Ethics Committee of the Second Hospital of Shantou University Medical College. The subjects of this study were recruited from the Cleft Lip and Palate Treatment Center of the Second Hospital of Shantou University Medical College in Guangdong, China. Two hundred and forty-one patients with NSCP (including 103 complete trio families) were selected, and informed consent was obtained. Subjects with known teratogenic exposure and other recognized syndromes, as well as children with other major or multiple minor defects and/or developmental delay, as determined from demographic details, perinatal history, teratogenic exposure, and family history, were excluded. Two hundred and forty-two unaffected individuals from the same geographic area, who had no craniofacial anomaly or other congenital disease and no family history of craniofacial malformation, were included in the study as controls. There were 94 men and 147 women in case group and 103 men and 139 women in control group, and the difference was not statistically different (p = 0.426). The cases and controls are unrelated. Informed consent was given for each study participant for both the blood collection and subsequent genotyping.
Sample and baseline data
Peripheral blood samples (10 mL from each case) were collected by venipuncture. Total genomic DNA was extracted from blood samples, SNPs were genotyped by matrix assisted laser desorption/ionization time of flight mass spectrometry (MALDI-TOF-MS), and genetic analysis was performed. There was no significant difference between the groups regarding sex and age (p > 0.05).
Search strategy for the relationship between IRF6 gene polymorphisms and NSCP risk
Association reports were searched from the electronic databases of PubMed and the Cochrane Library on June 1, 2017. The retrieval strategy using “(interferon regulatory factor 6 or IRF6) and (polymorphism or polymorphisms or genotype or genotypes or allele or alleles) and (cleft lip or cleft palate)” was entered into these databases mentioned above. Additional studies were identified by references cited in included articles.
Inclusion and exclusion criteria
Inclusion criteria
(1) The study should provide data for IRF6 rs2235371, rs642961, and rs2013162 genotype distribution (Garcia-Gonzalo and Izpisúa Belmonte, 2008); (2) there were at least two groups (case vs. control groups); and (3) the outcome was NSCP risk.
Exclusion criteria
(1) Review articles, editorials, or case reports (Garcia-Gonzalo and Izpisúa Belmonte, 2008); (2) preliminary results did not concern IRF6 rs2235371, rs642961, or rs2013162 gene polymorphisms or outcome; and (3) investigated the role of IRF6 gene expression to disease.
Data extraction
The following information from each included study was extracted independently by two investigators: first author's surname, ethnicity, year of publication, control source of the control group, and the number of cases and controls for IRF6 rs2235371, rs642961, and rs2013162 genotypes. From the corresponding genotype distribution, frequencies of the A allele of IRF6 rs2235371, rs642961, and rs2013162 were calculated for the case and control groups. The results were compared and disagreement was resolved by discussion.
Statistical analysis
Data were analyzed by bivariate and multivariate statistics. Allele frequencies and genotype frequencies were calculated by direct counting of alleles and genotypes and were compared between the patients and the controls using a chi-squared test. SPSS 16.0 software was used for the statistical analysis.
The available data from each investigation were extracted and calculated using Cochrane Review Manager Version 5 (Cochrane Library, UK). The pooled statistic was counted by the fixed effects model, but a random effects model was used when the p value of the heterogeneity test was <0.1. Results were expressed as odds ratios (ORs) for dichotomous data, and 95% confidence intervals (CIs) were also calculated. p < 0.05 was required for the pooled OR to be statistically significant. I2 was used to test the heterogeneity among the included studies. The Begg adjusted rank correlation test (Begg and Mazumdar, 1994) and the Egger regression asymmetry test (Egger et al., 1997) were used to assess publication bias (p < 0.1 was considered significant).
Results
Genotype frequencies of IRF6 rs2235371 in the case group were as follows: GG genotype 23.7%, AG genotype 49%, and AA genotype 27.4%. Genotype frequencies in the control group were as follows: GG genotype 32.6%, AG genotype 51.2%, and AA genotype 16.1%. There were significant differences in the genotypes (p = 0.0049) and allele frequencies (p = 0.0016) for IRF6 rs2235371 between NSCP and control groups. The distribution of the A allele and AA genotype in the case group was higher than that in the control group, and the OR (95% CI) was 1.504 (1.167-1.940) and 1.963 (1.259-3.062), respectively (Table 1).
IRF 6 Genotype and Allele Distribution in Patients with Nonsyndromic Cleft Palate and in Controls
CI, confidence interval; IRF6, interferon regulatory factor 6; NSCP, nonsyndromic cleft palate; OR, odds ratio.
The genotype frequencies of IRF6 rs801619 in the case group were as follows: AA genotype 70.5%, GA genotype 27.4%, and GG genotype 2.1%. Correspondingly, the genotype frequencies in the control group were as follows: AA genotype 58.7%, GA genotype 37.2%, and GG genotype 4.1%. There were significant differences in the genotypes (p = 0.0195) and allele frequencies (p = 0.0061) for IRF6 rs801619 between NSCP and control groups. The G allele in the case group was significantly lower than that in the control group, and the OR (95% CI) was 0.637 (0.460-0.880). Also, we found that the dominant model (GA+GG vs. AA) comparison had significant differences between the two groups, with an OR (95% CI) of 0.593 (0.406-0.864), corresponding to the (AA vs. GA+GG) under the mode of OR (95% CI) 1.686 (1.563-2.463) (Table 1).
At rs642961, rs44844880, and rs8049367, in the IRF6 locus, genotype, and allele frequencies were not statistically different between the NSCP group compared with normal controls (Table 1).
Haplotype analysis
Three sites rs2235371, rs861019, and rs642961 constitute Block 1, and there were significant difference for haplotype of TAG and CGG distribution between the two groups (p < 0.05; Block 1; Table 2 and Fig. 1).

Association of IRF6 A/G gene polymorphism on NSCP risk in overall populations. The haplotypes block was defined by using the default setting of the Haploview software. There were three variants: rs2235371, rs861019, and rs560426 which showed significant LD with each other and highly strong D′ (D′=1), and spanned 25κb in block 1. Block colors indicate the LD status of SNPs; light red box means high linkage between two SNPs, white box indicates low linkage, and pink box indicates moderate linkage. IRF6, interferon regulatory factor 6; LD, linkage disequilibrium; NSCP, nonsyndromic cleft palate. Color images are available online.
The Result of Haplotype Analysis
Transmission/disequilibrium test analysis
The analysis indicated that the T allele of the rs2235371 polymorphic locus and the A allele of the rs861019 polymorphic locus were overtransferred to the offspring (Z > 0, p < 0.05; Table 3).
Transmission/Disequilibrium Test Analysis Results
Study characteristics
Thirty-three studies were included from the databases (Fig. 2). Twenty-one studies (Stokes et al., 2001; Srichomthong et al., 2005; Jugessur et al., 2008; Ali et al., 2009; Birnbaum et al., 2009; Huang et al., 2009; Tang et al., 2009; Carter et al., 2010; Pan et al., 2010; Paranaíba et al., 2010; Shi et al., 2011; Letra et al., 2012; Li et al., 2012; Gurramkonda et al., 2013; Meara et al., 2013; Song et al., 2013; Yao et al., 2014; Ibarra-Arce et al., 2015; Jafary et al., 2015; Mijiti et al., 2015; Xu et al., 2016) (including our study) reporting the relationship between IRF6 rs2235371 gene polymorphism and NSCP risk were recruited into this meta-analysis. The data of interest were extracted, and the frequencies of the A allele of IRF6 rs2235371 for the case and control groups were calculated. The study characteristics of the included studies are presented in Table 4. The 22 investigations contained 4525 NSCP patients and 5980 non-NSCP controls.
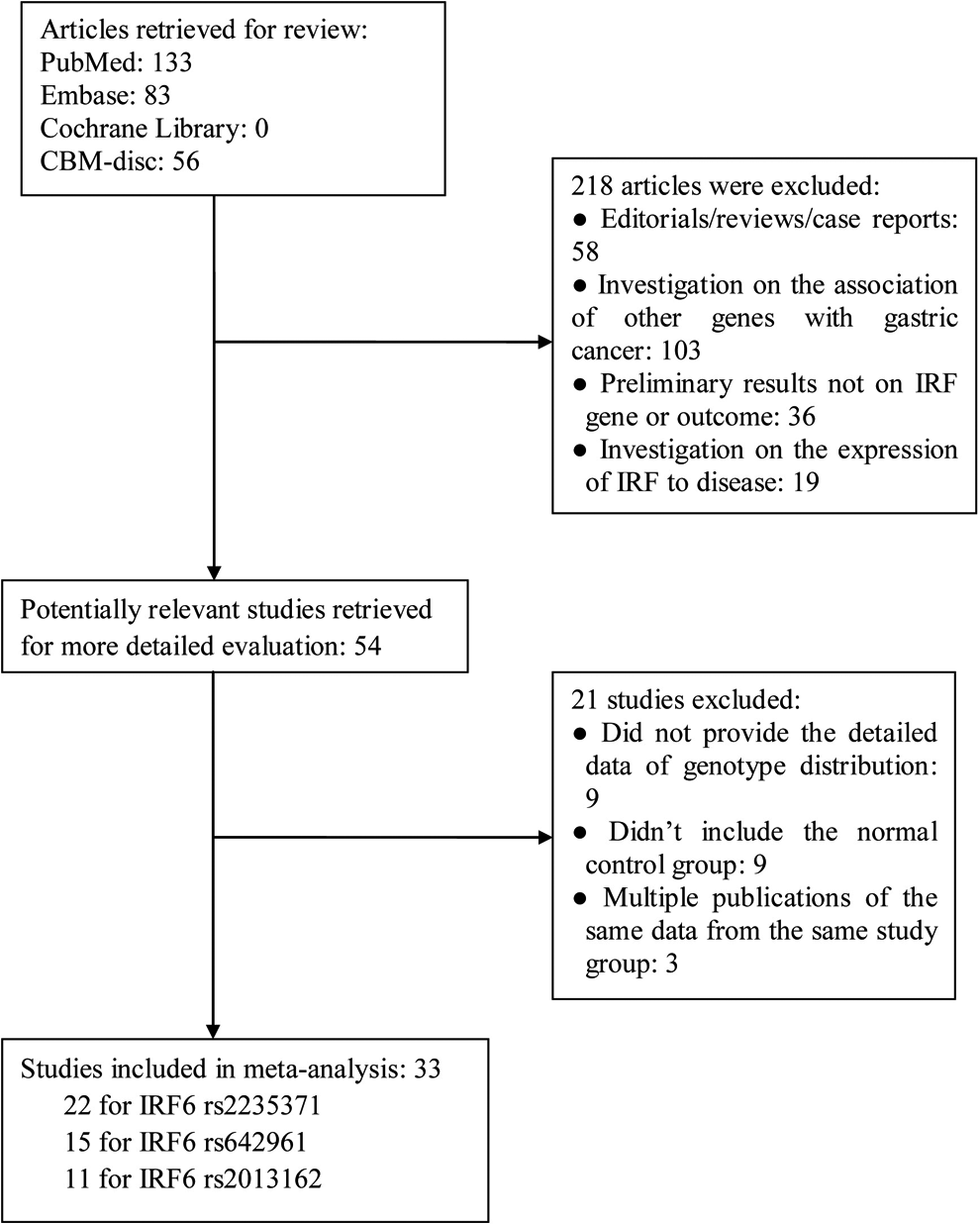
Flow chart of the study search and selection.
Characteristics of the Studies Evaluating the Effects of IRF 6 A/G Gene Polymorphism (rs2235371) on Nonsyndromic Cleft Palate Risk
Fifteen studies (Rahimov et al., 2008; Birnbaum et al., 2009; Huang et al., 2009; Mostowska et al., 2010; Pan et al., 2010; Paranaíba et al., 2010; Shi et al., 2011; Brito et al., 2012; Ren et al., 2012; Gurramkonda et al., 2013; Aldhorae et al., 2014; Krasone et al., 2014; do Rego Borges et al., 2015; Kerameddin et al., 2015; Tian et al., 2015) (including our study) reporting the relationship between IRF6 rs642961 gene polymorphism and NSCP risk were recruited into this meta-analysis. The data of interest were extracted, and the frequencies of the A allele of IRF6 rs642961 for the case and control groups were calculated. The study characteristics of the included studies are presented in Table 5. The 15 investigations contained 3483 NSCP patients and 5499 non-NSCP controls.
Characteristics of the Studies Evaluating the Effects of IRF 6 A/G Gene Polymorphism (rs642961) on Nonsyndromic Cleft Palate Risk
Eleven studies (Jugessur et al., 2008; Birnbaum et al., 2009; Huang et al., 2009; Carter et al., 2010; Weatherley-White et al., 2011; Letra et al., 2012; Meara et al., 2013; do Rego Borges et al., 2015; Ibarra-Arce et al., 2015; Mijiti et al., 2015; Xu et al., 2016) reporting the relationship between IRF6 rs2013162 gene polymorphism and NSCP risk were recruited into this meta-analysis. The data of interest were extracted, and the frequencies of the A allele of IRF6 rs2013162 for the case and control groups were calculated. The study characteristics of the included studies are presented in Table 6. The 11 investigations contained 2596 NSCP patients and 3957 non-NSCP controls.
Characteristics of the Studies Evaluating the Effects of IRF 6 A/C Gene Polymorphism (rs642962) on Nonsyndromic Cleft Palate Risk
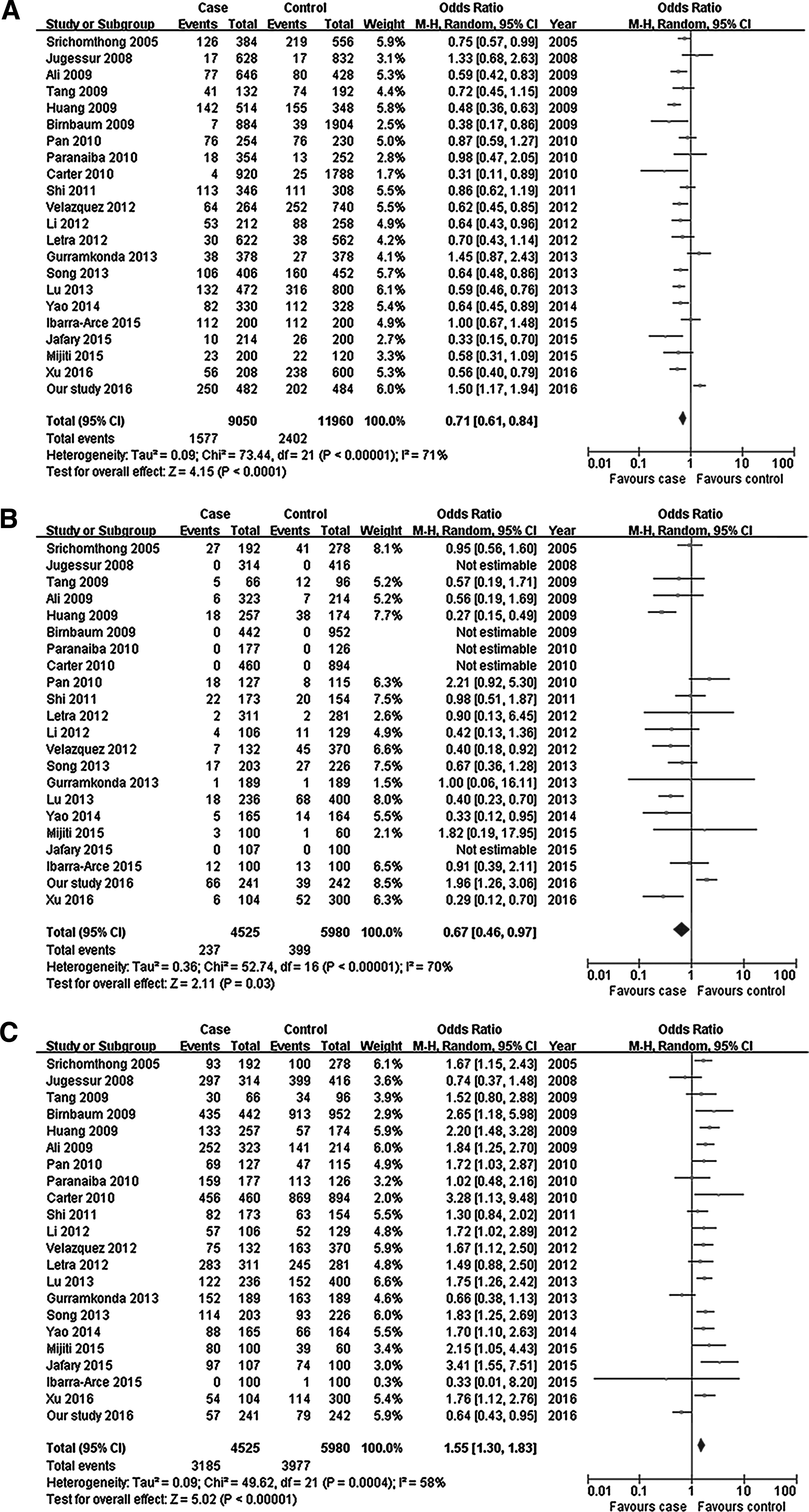
The IRF6 A/G gene polymorphism (rs2235371) is associated with NSCP risk
In this meta-analysis, we found that the IRF6 A/G gene polymorphism (rs2235371) was associated with NSCP risk (A allele: OR = 0.71, 95% CI: 0.61-0.84, p < 0.0001; AA genotype: OR = 0.67, 95% CI: 0.46-0.97, p = 0.03; and GG genotype: OR = 1.55, 95% CI: 1.30-1.83, p < 0.00001; Fig. 3 and Table 7). In the subgroup analysis according to ethnicity, this meta-analysis indicated that the IRF6 A allele and GG genotype were associated with NSCP risk in the Asian population, but not the AA genotype. Interestingly, the IRF6 A/G gene polymorphism rs2235371 was not associated with NSCP risk in Caucasians (Table 7).
Association of IRF6 A/C gene polymorphism (rs2013162) on NSCP risk in overall populations.
Meta Analysis of the Association of IRF 6 Gene Polymorphism with Nonsyndromic Cleft Palate Risk
The IRF6 A/G gene polymorphism rs642961 is associated with NSCP risk, but not in Caucasians or Asians
In this meta-analysis, we found that the IRF6 A/G gene polymorphism rs642961 was associated with NSCP risk (A allele: OR = 1.50, 95% CI: 1.28-1.75, p < 0.00001; AA genotype: OR = 2.01, 95% CI: 1.40-2.88, p = 0.0001; GG genotype: OR = 0.66, 95% CI: 0.56-0.78, p < 0.00001; Fig. 4 and Table 7). In subgroup analysis according to ethnicity, the results indicated that IRF6 A/G gene polymorphism (rs642961) was not associated with NSCP risk in Asians and in Caucasians (Table 7).
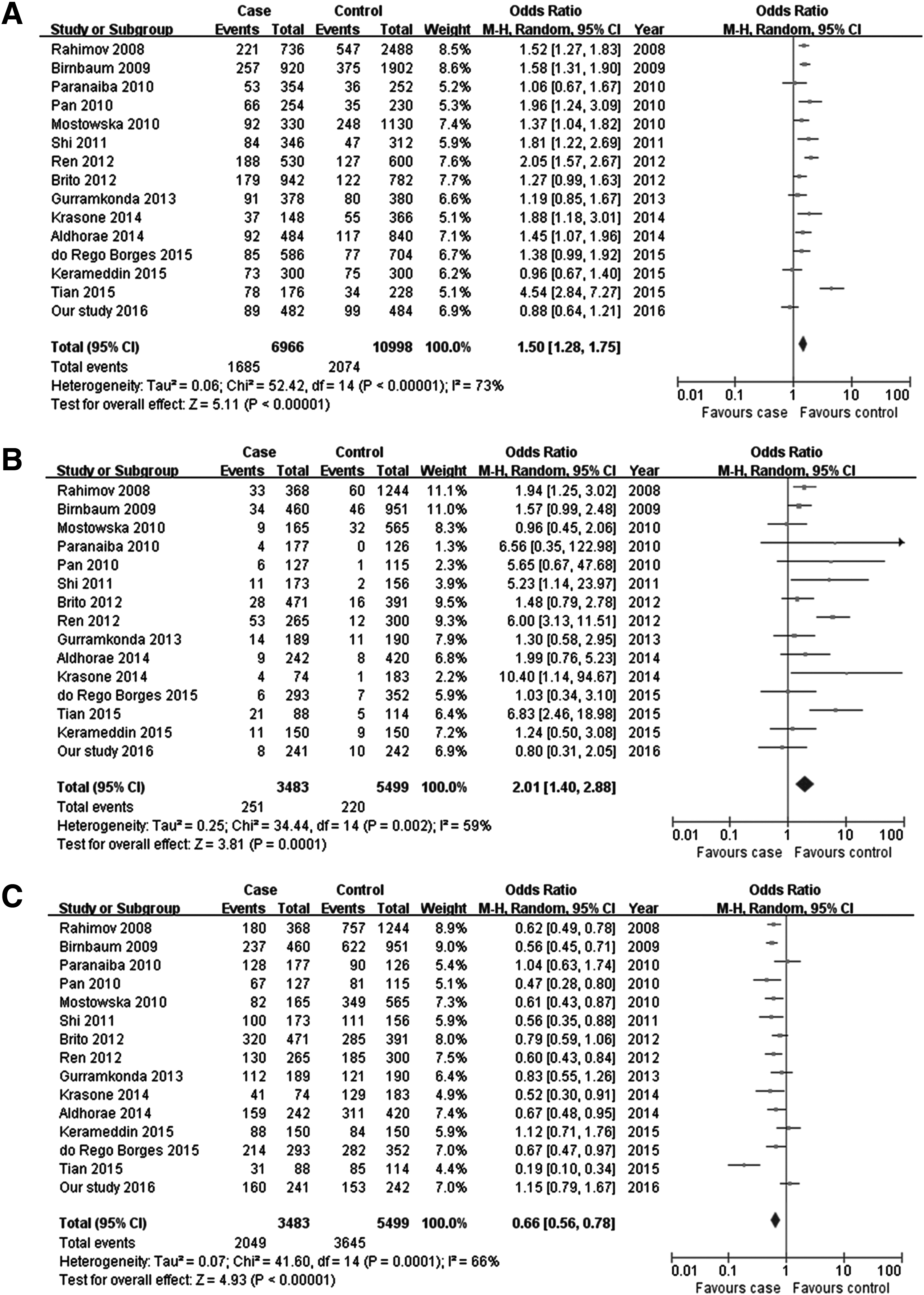
Association of IRF6 A/G gene polymorphism (rs642961) on NSCP risk in overall populations.
The IRF6 A/C gene polymorphism (rs2013162) is associated with NSCP risk in Caucasians, but not Asians
In this meta-analysis, we found that the IRF6 A/C gene polymorphism rs2013162 was not associated with NSCP risk (A allele: OR = 0.95, 95% CI: 0.80-1.12, p = 0.52; AA genotype: OR = 0.91, 95% CI: 0.69-1.20, p = 0.50; and CC genotype: OR = 1.05, 95% CI: 0.84-1.32, p = 0.64; Fig. 5 and Table 7). In subgroup analysis according to the ethnicity, the results indicated that IRF6 A/C gene polymorphism (rs2013162) was associated with NSCP risk in Caucasians, but not in Asians (Table 7).
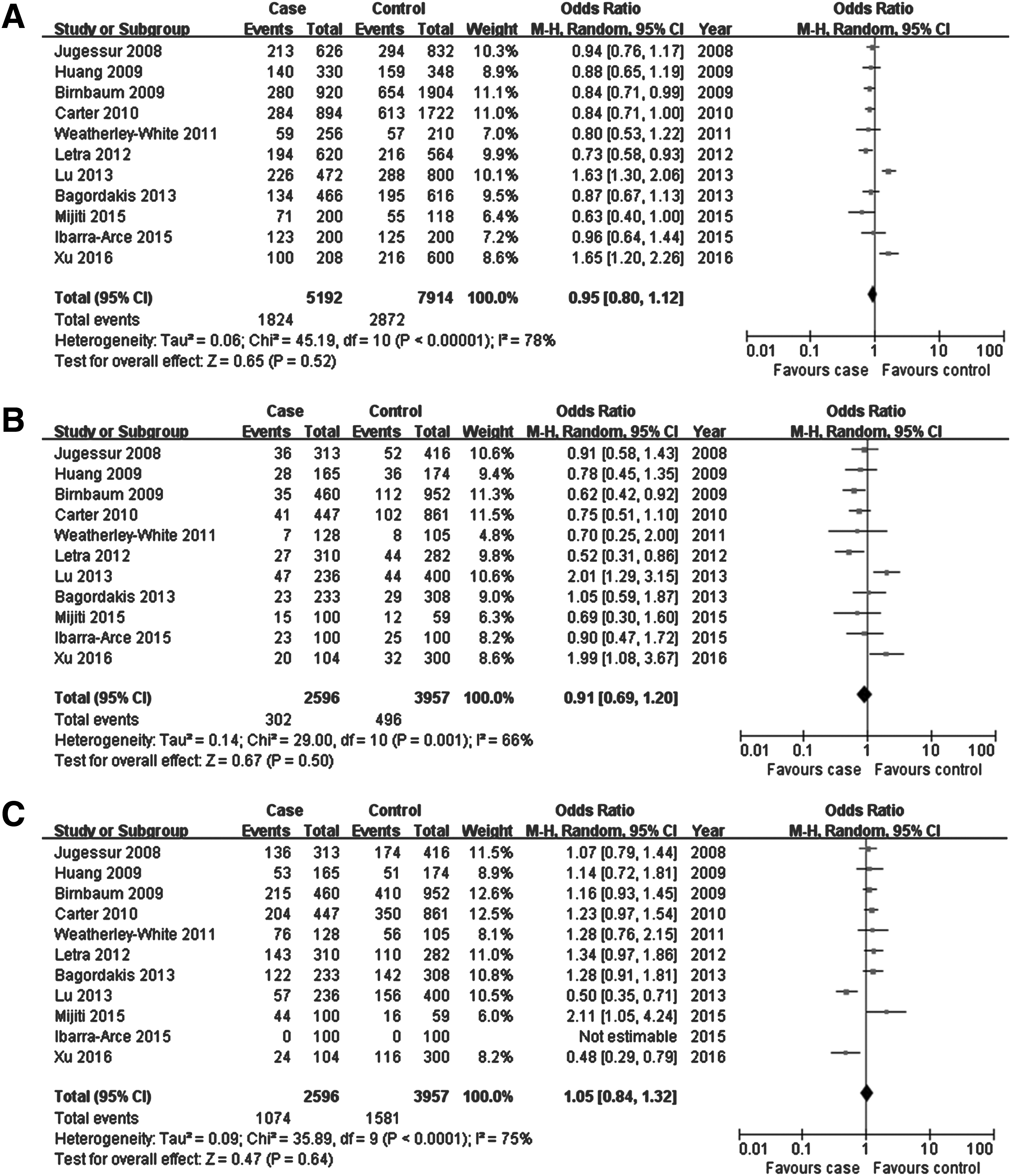
Association of IRF6 A/C gene polymorphism (rs2013162) on NSCP risk in overall populations.
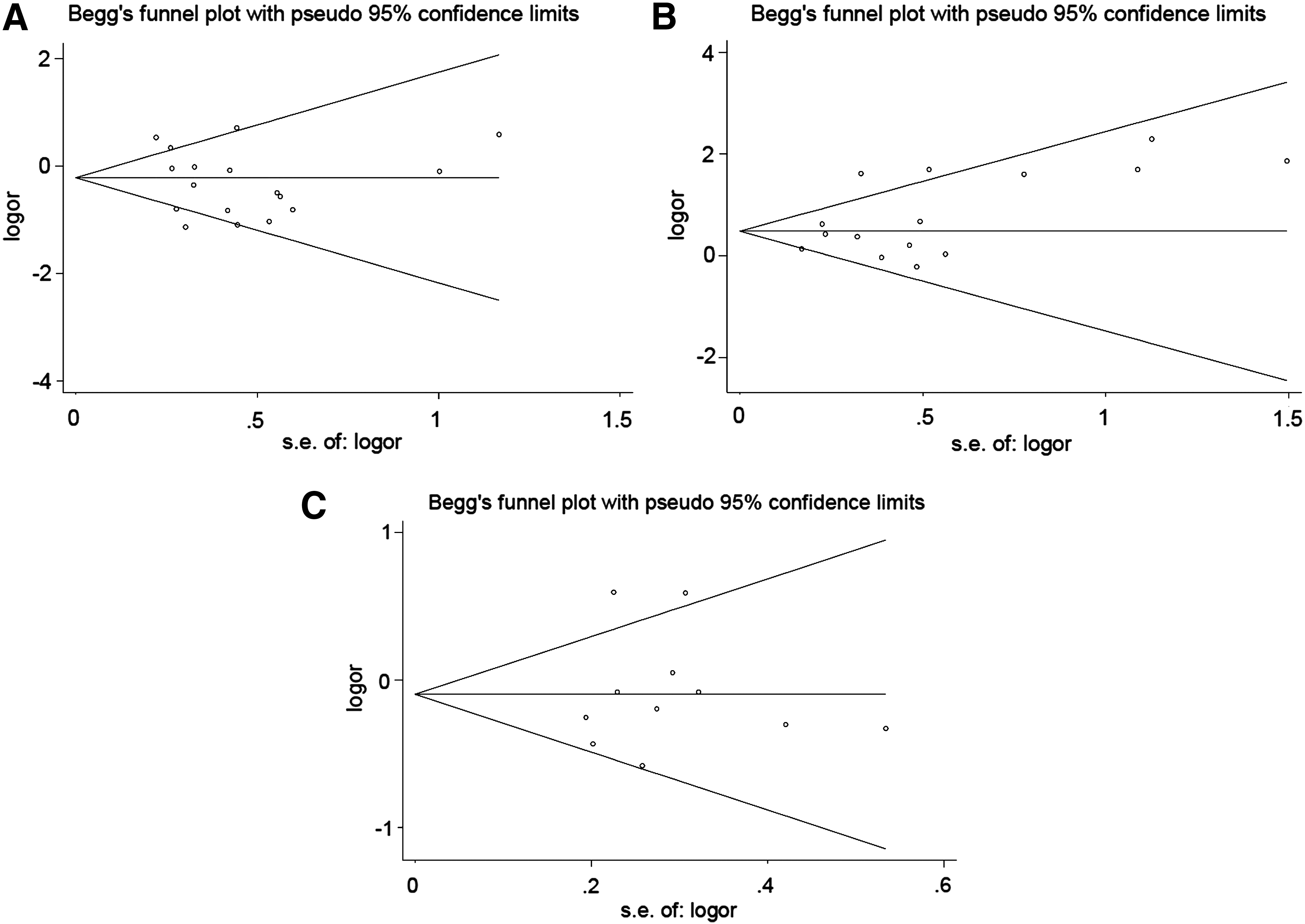
Evaluation of publication bias
Publication bias was detected and there was no publication bias for IRF6 rs2235371 gene polymorphism (Begg p = 0.510, Egger p = 0.616; Fig. 6A), IRF6 rs642961 gene polymorphism (Begg p = 0.181, Egger p = 0.785; Fig. 6B), and IRF6 rs2013162 gene polymorphism (Begg p = 0.876, Egger p = 0.845; Fig. 6C) with NSCP risk for overall population.
Publication bias was evaluated for the overall populations.
Discussion
In these studies, we selected 241 patients with NSCP (including 103 complete trio families), and 242 unaffected individuals from the same geographic area, who had no craniofacial anomaly or other congenital disease, and no family history of craniofacial malformation. We compared the IRF6 rs2235371, rs801619, rs642961, rs44844880, and rs8049367 polymorphisms between the two groups and show that the IRF6 rs2235371 A allele and AA genotype in the NSCP group are more highly represented than in the control group. The IRF6 rs801619 AA genotype and G allele are also associated with NSCP risk, but the rs642961, rs44844880, and rs8049367 polymorphisms were not statistically different between the NSCP groups. This study suggests that the IRF6 rs2235371 A allele and AA genotype, and the IRF6 rs801619 AA genotype and G allele are useful indicators for predicting NSCP risk in south China.
We further conducted a meta-analysis for rs2235371, rs642961, and rs2013162 polymorphisms, to enhance the robustness of our data, and report that the IRF6 A/G gene polymorphism (rs2235371) and IRF6 A/G gene polymorphism (rs642961) are associated with NSCP risk in the general population, whereas the IRF6 A/C gene polymorphism (rs2013162) is not.
Similar to Caucasians, in Asians, the IRF6 rs2235371 A allele and GG genotype are associated with NSCP risk, but the AA genotype is not. Neither the IRF6 A/G gene polymorphism (rs642961) nor the IRF6 A/C gene polymorphism (rs2013162) is associated with NSCP risk for Asians. However, the IRF6 A/C gene polymorphism (rs2013162) has been associated with NSCP risk in Caucasians.
Previously, Wattanawong et al. (2016) conducted a meta-analysis and reported that for rs2235371, the AA and GA genotypes carry, respectively, 51% and 42% lower risks of NSCP than the GG genotype in Asians, but these genotypes were not significant in Caucasians. For rs2013162, the AA genotype was significant only for Caucasians, carrying 0.65 times lower odds than CC in Caucasians, but not for Asians. For rs642961, the AA and GA genotypes, respectively, carry 2.47 and 1.40 times higher odds in Asians, and 2.03 and 1.58 times higher odds in Caucasians, compared with the GG genotype. For rs987525, the AA and CA genotypes carry 2.27 and 1.34 times higher odds in Asians, 5.25 and 2.13 times higher odds in Caucasians, and 1.42 and 1.28 times higher odds in mixed ethnicities, compared with the CC genotype. Our meta-analysis includes more original studies to pool the OR, and thus, the results from our meta-analysis should be more robust.
There was limitation in this study. There were heterogeneities among the included studies, and the subgroup analysis did not eliminate the heterogeneity.
In conclusion, IRF6 A/G gene polymorphisms rs2235371 and rs642961, but not the IRF6 A/C gene polymorphism rs2013162, were associated with NSCP risk.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by funds from National Natural Science Foundation of China (81571920), Natural Science Foundation of Guangdong Province (2015A030313436, 2016A030313061), Shanfuke (2018) 157-45, Shan (2014) 242-56, Shanfuke (2012) 165, and STURCS-201813.