
Abstract
Objective:
To investigate the association between polymorphisms in the rs2010963 and rs69947 loci of the vascular endothelial growth factor A (VEGFA) gene; the rs4646994 locus of the angiotensin I converting enzyme (ACE) gene; and the rs4880 locus of the superoxide dismutase 2 (SOD2) gene with genetic susceptibility to type 2 diabetic nephropathy (T2DN) in the Chinese Han population.
Methods:
A total of 650 Chinese Han patients with T2DN and 580 non-nephropathy patients with type 2 diabetes were enrolled in this study. Sanger sequencing was used to detect the genotypes of the rs2010963 and rs69947 loci within VEGFA, the rs4646994 locus of for the ACE gene, and the rs4880 locus of the SOD2 gene in all subjects. Enzyme-linked immunosorbent assays were used to detect VEGFA, ACE, and SOD2 levels in serum.
Results:
The risk of T2DN was significantly increased (odds ratio [OR] = 1.15, confidence interval [95% CI]: 1.03-1.30) in patients with the GC/CC genotypes compared to those with the GG genotype at the rs2010963 locus of the VEGFA gene under the dominant model of inheritance. Similarly, the risk of T2DN was significantly increased (OR = 1.17, 95% CI: 1.05-1.31) in patients with the CA/AA genotypes compared to those with the CC genotype at the rs69947 locus of the VEGFA gene under the dominant model of inheritance. In addition, the risk of T2DN was increased (OR = 1.57, 95% CI: 1.37-1.74) in patients with the AA genotype compared to the CC/CA genotypes under the recessive model of inheritance. The risk of T2DN was also significantly increased (OR = 1.54, 95% CI: 1.24-1.97) in patients with the ID/DD genotypes compared to those with the II genotype at the rs4646994 locus of the ACE gene under the dominant model; and (OR = 1.41, 95% CI: 1.26-1.57) for DD genotype compared to the II/ID genotypes under the recessive model. We also found the risk of T2DN was significantly increased (OR = 1.25, 95% CI: 1.11-1.39) under the dominant model in patients with the TC/CC genotypes compared to the TT genotype, and for the CC genotype (compared to the TT/TC genotype) (OR = 1.45, 95% CI: 1.18-1.66) under the recessive model at the rs4880 locus of the SOD2 gene rs4880. The haplotypes GAC (OR = 1.17, 95% CI: 1.04-1.29), CAT (OR = 1.12, 95% CI: 1.03-1.60), and CAC (OR = 1.13, 95% CI: 1.01-1.24) constructed from VEGFA gene rs2010963 and rs69947 loci, and the SOD2 gene rs4880 locus were associated with a higher risk for T2DN. Finally, we found that VEGFA protein levels from subjects with the rs2010963 GG genotype and the rs69947 CC genotype were higher in both case groups and the control group than in subjects with rs2010963 GA/AA genotypes and rs69947 CA/AA genotypes, respectively (p < 0.05). The ACE protein levels for variants at the rs4646994 locus showed that the case group and control group subjects with the DD genotype had the highest levels, followed by the ID genotype and the II genotype (p < 0.05).
Conclusion:
Genetic variation in the VEGFA gene at the rs2010963 and rs69947 loci, the ACE gene at the rs4646994 locus, and the SOD2 gene at the rs4880 locus may increase the risk of developing T2DN.
Introduction
Diabetic nephropathy (DN) is a chronic disease characterized by proteinuria, glomerular hypertrophy, decreased glomerular filtration rate, and renal fibrosis accompanied by renal dysfunction (Gnudi et al., 2016). DN is the main cause of end-stage renal disease, and hyperglycemia is the driving factor in the development of DN (Cao et al., 2016). DN is often underdiagnosed and undertreated, and there is a lack of awareness of the pathophysiologic mechanisms that contribute to this disease. There is currently much evidence showing that DN morbidity may be related to genetic factors (Gong et al., 2016), renal hemodynamics abnormalities (Mora-Gutiérrez et al., 2017), vasoactive substances metabolism disorders (Han et al., 2016), hyperglycemia metabolic disorders (Ji et al., 2016), hypertension (Giunti et al., 2006), and other factors.
Vascular endothelial growth factor A (VEGFA) is a protein secreted by podocytes that is necessary for the survival of endothelial cells, podocytes, and mesangial cells (Guangqi et al., 2012). Chronic hyperglycemia induces excessive VEGFA production and low endothelial nitric oxide, which aggravates the development and progress of DN (Tufro and Veron, 2012). Recent studies have revealed that VEGFA may be a new potential target for treating DN (Li et al., 2017; Stevens and Oltean, 2018).
Multiple polymorphic sites of the VEGFA gene are associated with the development of disease. Polymorphisms at the rs2010963 and rs69947 loci may be associated with complications of preterm birth (Langmia et al., 2015). However, it is unclear whether genetic polymorphisms of the VEGFA gene are related to the risk of DN. The role of angiotensin I converting enzyme (ACE) is to catalyze the production of angiotensin II by angiotensin I. In the kidneys of diabetic patients, the role of angiotensin II is mainly to increase the glomerular pressure and the glomerular filtration rate (Chow et al., 2016). The relationship between the insertion and deletion mutations of ACE gene and coronary heart disease has been reported (Fang et al., 2015). However, whether ACE gene insertion-deletion mutations affect the occurrence of DN is still lacking sufficient evidence to support it. Superoxide dismutase (SOD) is an antioxidant enzyme with high catalytic activity exhibiting for superoxide anion radical scavenging activity. This enzyme can clear mitochondrial reactive oxygen species (ROS) and is the first line of key antioxidant defense enzymes (Mccord and Edeas, 2005). SOD has three forms: SOD1 (in plasma), superoxide dismutase 2 (SOD2) (in mitochondria), and SOD3 (in the extracellular matrix). Clinical studies have confirmed that SOD protects cells and extracellular components from damage associated with the inflammatory process and has a protective effect in many diseases (Robbins and Zhao, 2014). Studies have confirmed that the occurrence of type 2 diabetes mellitus (T2DM) is associated with oxidative stress (Muriach et al., 2014). SOD2 may also play an important role in the development of DN, and polymorphism of the rs4880 locus of the SOD2 gene is associated with the occurrence of various diseases (Xu et al., 2015). It is not clear whether this polymorphism is related to the occurrence of DN.
In this study, 650 patients with type 2 diabetic nephropathy (T2DN) and 580 patients with non-nephrotic T2DM were included as controls by case-control. The relationship between T2DN susceptibility and the rs2010963 and rs69947 loci of the VEGFA gene, rs4646994 locus of the ACE gene, and rs4880 locus of the SOD2 gene were analyzed.
Materials and Methods
General information
Patients with T2DM who were treated in our hospital (n = 1230) were recruited into the study between August 2014 and December 2017. Patients were diagnosed with DN according to the American Diabetes Association diagnostic criteria for diabetes. All subjects were of the Chinese Han population, among which 650 patients with T2DN were recruited as the case group for this study and 580 patients with non-nephrotic T2DM were used as the control group and excluded other complications of proteinuria and renal insufficiency. All T2DM patients were evaluated for their estimated 24-h albumin excretion rate (AER) or urinary albumin-to-creatinine ratio (ACR). AER or ACR measurements were taken twice, and the average for each patient was recorded. Diabetic nephropathy can be diagnosed in patients with microalbuminuria (AER = 30 − 300 mg/24 h or ACR = 30 − 300 mg/g), and accompanied with diabetic retinopathy or proteinuria (AER ≥300 mg/24 h or ACR ≥300 mg/g) or starting renal replacement therapy for at least 5 years before diagnosis of advanced kidney disease. The following individuals were excluded from the study: those with (1) gestational diabetes mellitus (DM); (2) secondary DM; (3) mitochondrial disease (mitochondrial myopathy, encephalopathy, lactic acidosis, and apoplexy); or (4) immune system disease. All subjects signed written informed consent and the study protocol was approved by the Medical Ethics Committee of our hospital.
Clinical data collection
All subjects' age, sex, DM course, smoking, alcohol consumption, hypertension, and DM family history were investigated. At the same time, fasting serum biochemical indexes including HbA1c, total cholesterol (mM), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglycerides were tested. The test instrument used was the cobas c8000 clinical Chemistry System (Roche, Basel, German). Early morning urine samples were collected and the urinary albumin and creatinine concentrations were determined by the Afinion AS100 Analyzer (Alere Afinion, Chicago). The urinary ACR was defined as the urinary albumin value divided by the creatinine concentration (mg/g).
Genotype detection analysis
Blood samples (5-6 mL) from the elbow veins were collected from the subjects, 2 mL of which were extracted with EDTA anticoagulant and genomic DNA was obtained. The remaining blood samples were centrifuged at 3000 rpm for 4 min at 20 min and stored at −70°C for testing. Genomic DNA was amplified by PCR according to the primer sequence information provided in Table 1. The final volume of the PCR was 25 μL containing 1.5 mM MgCl2, 50 mM KCl, 10 mM Tris-HCl (pH = 8.3), 0.2 mM dNTP, 0.8 U Taq polymerase, and 50 ng genomic DNA. After PCR, the products were sequenced by the Sanger method, and the genotype information of each polymorphic locus was analyzed. A 20% sample was selected for verification and the results were confirmed.
Single Nucleotide Polymorphism Site Information and Polymerase Chain Reaction Amplification Primers
ACE, angiotensin I converting enzyme; MAF, minor allele frequency; SOD2, superoxide dismutase 2; VEGFA, vascular endothelial growth factor A.
Serum VEGFA and ACE protein detection
The serum VEGFA protein detection kit from Cloud-Clone Corp., catalog number SEA143Hu, was used. The ACE test kit was from Ek-Bioscience, product number EK-H11882. Proteins were detected by enzyme-linked immunosorbent assays (ELISA) using a standard curve calculation. All operating methods were performed in strict accordance with the kit instructions.
Statistical analysis
The results for continuous variables were expressed as mean ± SD, and t-tests were used for statistical analysis. The categorical variable was expressed as n (%), and the chi-square test (χ2) was used to compare categorical variables. Whether the genotype frequency was consistent with Hardy-Weinberg equilibrium was verified by the χ2 test. The odds ratios (ORs) and their 95% confidence interval (CI) were calculated by unconditional logistic regression to estimate the effect of polymorphisms at the VEGFA gene rs2010963 and rs69947 loci, ACE gene rs4646994 locus, and SOD2 gene rs4880 locus on T2DN risk. Adjust age, gender, BMI, DM course, smoking, alcohol consumption, HbA1C, total cholesterol, triglycerides, HDL-C, LDL-C, hypertension, and DM family history. Haplotype analysis was performed using the online software SHEsis, gene-environment interactions were determined using multifactor dimensionality reduction (MDR) software, and statistical analysis was performed using SPSS 20.0 (IBM Corp., Chicago, IL). All tests were two-tailed, and p < 0.05 indicated that the difference was statistically significant.
Results
General information of case and control groups
The general clinical data of 650 patients with T2DN (case group) and 580 non-nephropathy patients with type 2 diabetes (control group) recruited in this study are shown in Table 2. There was no significant difference in the age, gender, DM course, smoking, alcohol consumption, triglyceride levels, LDL-C, or family history of DM between the case group and the control group (p > 0.05). The BMI, HbA1c, and total cholesterol levels in the case group were higher than those in the control group, and HDL-C levels were lower in the case group than in the control group (p < 0.05). Hypertension was a risk factor for T2DN (OR = 2.47, 95% CI: 1.95-3.12).
Demographic and Clinical Characteristics of Case and Control Group
CI, confidence interval; DM, diabetes mellitus; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; OR, odds ratio.
VEGFA, ACE, and SOD2 gene polymorphisms and T2DN risk
The VEGFA loci rs2010963 and rs69947, ACE locus rs4646994, and SOD2 locus rs4880 were all out of Hardy-Weinberg equilibrium in the 580 controls (p > 0.05). There was a risk of T2DN for GC and CC genotypes of the VEGFA gene rs2010963 locus, and the risk of T2DN in the GC/CC genotypes was significant increased compared to GG genotype (OR = 1.15, 95% CI: 1.03-1.30). There was no risk of T2DN in the CC genotype compared to GG/GC genotypes (OR = 1.11, 95% CI: 0.96-1.26). AA genotype at the rs69947 locus of the VEGFA gene represented a risk of T2DN, and CA/AA genotypes compared to AA genotype (OR = 1.17, 95% CI: 1.05-1.31) and the AA genotype compared to CA/CC (OR = 1.57, 95% CI: 1.37-1.74) suggested higher T2DN risk. The ACE gene rs4646994 locus ID and DD genotype had higher T2DN risk, and this gene locus ID/DD genotype compared to II (OR = 1.54, 95% CI: 1.24-1.97) and DD genotype compared to ID/II (OR = 1.41, 95% CI: 1.26-1.57) showed T2DN risk. TC and CC genotypes of the rs4880 locus of the SOD2 gene were related to risk for T2DN. The same TC/CC genotypes compared to TT genotype (OR = 1.25, 95% CI: 1.11-1.39) and CC genotype compared to TT/TC genotypes (OR = 1.45, 95% CI: 1.18-1.66) also suggested higher T2DN risk (Table 3).
Genotype Among Cases and Controls and Their Association with Type 2 Diabetic Nephropathy Risk
Adjusted for age, gender, BMI, DM duration, smoking, alcohol consumption, HbA1c, total cholesterol, triglycerides, HDL-C, LDL-C, hypertension, DM family history.
BMI, body mass index; SNP, single nucleotide polymorphism.
Stratified analysis of VEGFA, ACE, and SOD2 genotypes and T2DN risk
We hierarchically analyzed subjects' age (≤60, >60 years), sex (male and female), BMI (≤24, >24 kg/m2), DM course (≤10, >10 years), smoking (no, yes), drinking (no, yes), HbA1c (≤8, >8%), total cholesterol (≤5.0, >5.0 mM), triglycerides (≤1.7, >1.7 mM), HDL-C (≤1.0, >1.0 mM), LDL-C (≤3, >3.0 mM), hypertension (no, yes), and family history of DM (no, yes). Stratified analysis of the VEGFA gene rs2010963 and rs69947 loci, ACE gene rs4646994 locus, and SOD2 gene rs4880 locus polymorphisms were correlated with T2DN risk (Table 4). The increased risk of T2DN for the CC genotype in the rs2010963 locus of the VEGFA gene was associated with age, sex, BMI, DM course, total cholesterol, HDL-C, LDL-C levels, hypertension history, and DM family history. The T2DN risk for the CC genotype at the rs69947 locus of the VEGFA gene was higher in patients with higher age, BMI, DM course, smoking history, HDL-C, LDL-C levels, hypertension history, and DM family history. The high T2DN risk of the DD genotype in the ACE gene rs4646994 was related to the age, gender, BMI, and family history of DM. The higher risk T2DN of CC genotype in the rs4880 locus of the SOD2 gene was associated with the patient's age, BMI, DM disease history, smoking history, HbA1c, total cholesterol, triglycerides, HDL-C, LDL-C, hypertension history, and DM family history.
Stratification Analysis of the Five Single Nucleotide Polymorphisms and Diabetic Nephropathy Susceptibility
Adjusted for age, gender, BMI, DM course, smoking, alcohol consumption, HbA1c, total cholesterol, triglycerides, HDL-C, LDL-C, hypertension, and DM family history (the stratified factor in each stratum excluded).
Haploid typing and T2DN risk
Eight haplotypes (Table 5) were constructed from the VEGFA gene rs2010963 and rs69947 and SOD2 gene rs4880, and their correlation with T2DN risk was analyzed. The analysis showed that GAC (OR = 1.17, 95% CI: 1.04-1.29), CAT (OR = 1.12, 95% CI: 1.03-1.60), and CAC (OR = 1.13, 95% CI: 1.01-1.24) haplotypes were related with higher risk of T2DN, and no haplotypes were found to reduce the risk of T2DN.
Haplotype Analysis of Three Single Nucleotide Polymorphism Sites
VEGFA rs2010963/VEGFA rs699947/SOD2 rs4880.
VEGFA, ACE, and SOD2 gene interactions and T2DN risk
We used MDR to analyze the VEGFA gene rs2010963 and rs69947 sites, ACE gene rs4646994, and SOD2 gene rs4880 sites and the age, gender, BMI, DM disease history, smoking history, drinking history, HbA1c, total cholesterol, triglycerides, HDL-C, LDL-C, high blood pressure, family history of DM, and other factors were examined for the interaction between environmental factors affecting T2DN risk (Table 6). The optimal prediction model was the VEGFA gene rs2010963 site, SOD2 gene rs4880 site, BMI, and hypertension, in which T2DN risk increased 2.53 times (OR = 2.53, 95% CI: 2.20-2.75) (Table 6).
Interaction Results Between the Four Single Nucleotide Polymorphisms and Risk Factors by Multifactor Dimensionality Reduction
VEGFA and ACE gene polymorphisms and serum protein levels
We used ELISA to detect serum VEGFA and ACE protein levels in all subjects (Fig. 1). We found that the rs2010963 and rs69947 polymorphisms of the VEGFA gene were associated with serum VEGFA protein level in the case group and control group, and the wild-type VEGFA protein level was higher than the mutant type (p < 0.05). Serum VEGFA protein levels were lower in case patients than in controls (p < 0.001) (Fig. 1A, B). Similarly, the ACE protein level of individuals with the ACE gene rs4646994 polymorphism was found in the case group and control group, which was highest in DD genotype, followed by ID genotype, and lowest in genotype II (p < 0.05). The serum ACE protein level was higher in the case group than in the control group (p < 0.001) (Fig. 1C).
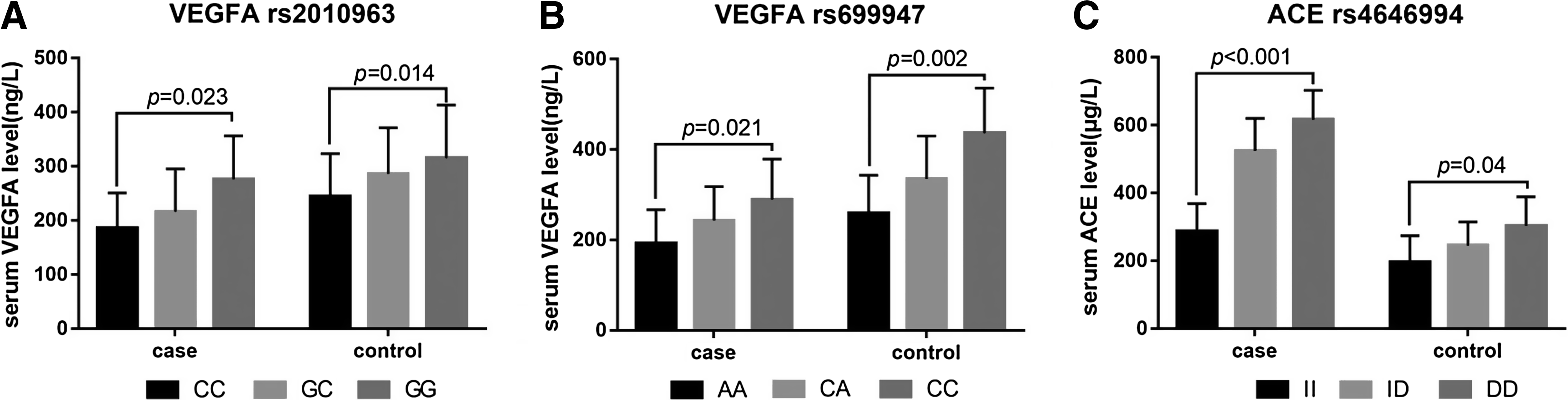
VEGFA, ACE gene polymorphisms and serum VEGFA protein and ACE protein levels.
Discussion
In this study, we investigated the association between genetic polymorphisms in VEGFA, ACE, and SOD2 genes and susceptibility to diabetic nephropathy in Han Chinese. We found that genetic variation in the VEGFA gene rs2010963 and rs69947 loci, ACE gene rs4646994 locus, and SOD2 gene rs4880 locus may increase the risk of developing T2DN.
More and more evidence shows that genetic factors play an important role in the occurrence and development of DN (Sandholm, 2014; Todd et al., 2015). VEGFA is an important angiogenic factor. Lindenmeyer et al. (2007) showed that upregulation of VEGFA in diabetic kidney can protect capillaries from damage. In diabetics, reduced VEGFA levels may lead to DN progression. Studies have shown that the rs2010963 and rs69947 polymorphisms of the VEGFA gene affect the expression of VEGFA protein and have an important influence on the development of diabetes (Lu et al., 2013). In this study, the rs2010963 and rs69947 polymorphisms of the VEGFA gene were also associated with high risk of T2DN. The risk of T2DN in the former dominant model was significant (OR = 1.15, 95% CI: 1.03-1.30), while the latter dominant model (OR = 1.17, 95% CI: 1.05-1.31) and the recessive model (OR = 1.57, 95% CI: 1.37-1.74) all had higher T2DN risk. In addition, the results of this study also showed that the rs2010963 and rs69947 polymorphisms of the VEGFA gene were associated with serum VEGFA protein expression, and the wild-type VEGFA protein level was higher than that of the mutant type. Langmia et al. (2015) also found that the rs2010963 and rs69947 polymorphisms of the VEGFA gene were associated with spontaneous preterm birth. It was also found that the levels of VEGF protein in peripheral blood of pregnant women with different genotypes differed significantly from each other. The difference is that frequencies of the G allele in the VEGFA gene rs2010963 loci are higher than those in the C allele in the Chinese population. Contrary to the results of this study, this difference may be related to the different ethnic groups examined.
In diabetic kidneys, angiotensin II increases glomerular pressure and glomerular filtration rate, and angiotensin II results from ACE catalyzing angiotensin I. The ACE gene is located on chromosome 17q23, which has multiple mutations, including rs464994, rs8066114, and rs4461142 (Wang et al., 2013). The insertion and deletion mutations in intron 16 are very important ones, namely rs464994, which is related to high ACE activity in serum (Saddick, 2015). The results of this study show that the rs4646994 locus deletion mutation in the ACE gene results in a high risk of T2DN, and both the dominant model (OR = 1.54, 95% CI: 1.24-1.97) and recessive model (OR = 1.41, 95% CI: 1.26-1.57) had a high risk of T2DN. Alharbi (2017) found that the missing genotype was associated with T2DN in the Arab region, which was consistent with the results of this study. In addition, the results of this study showed that the missing group serum ACE levels were significantly higher than those in the insertion mutation group, which is consistent with the results of the study by Saddick (2015). This indicates that the expression level and activity of ACE in patients with ACE-deficient T2DM are elevated, leading to the increased production of angiotensin II. On one hand, ACE deficiency causes vasoconstriction and sodium-water retention in the catheterization system in hypertensive blood pressure. On the other hand, it has a direct effect on the kidney, increasing glomerular pressure, filtration pressure and permeability, glomerular loss, causing proliferation, secretion, inflammation, and hardening of renal intrinsic cells and infiltrating cells, leading to progressive degeneration and loss of function in kidney tissue (Burns and Thomas, 2011; Alharbi, 2017).
Oxidative stress plays an important role in the occurrence and development of T2DN. The activation of the renin-angiotensin system exacerbates ROS-induced renal injury in diabetic nephropathy, and remission of ROS production can improve kidney damage caused by DN. SOD is an antioxidant enzyme that has high catalytic activity against superoxide anion radicals and participates in various biological processes induced by OS (McCord and Fridovich, 1969). In mitochondria, the SOD2 gene is the main isoform present, which is located on chromosome 6q25. The protein encoded by SOD2 is one of the major cellular defenses against oxidative stress. In recent years, genetic variations of the SOD2 gene have aroused the interest of researchers. Studies have shown that rs4880 gene polymorphisms are related to SOD2 transport efficiency and activity in mitochondria (Sutton et al., 2003). The results of this study showed that TC and CC genotypes of the rs4880 locus of the SOD2 gene are related with risk for T2DN. The dominant model (OR = 1.25, 95% CI: 1.11-1.39) and recessive model (OR = 1.45, 95% CI: 1.18-1.66) also were related with high T2DN risk. Unfortunately, this study did not detect a relationship between SOD2 protein expression and rs4880 gene polymorphism. Interestingly, however, Xu et al. (2015) investigated the relationship between the risk of hypertension and the polymorphism of the SOD2 gene rs4880 in China, and found that the frequency of CC and TC genotypes differed significantly between patients with hypertension and normal humans, and further studies in cell models found that the C allele decreased the expression of SOD2. Therefore, the authors believe that the decreased expression level of the SOD2 gene in C allele carriers leads to higher level of oxidative stress, and the final result is DN progression.
The haplotypes were further analyzed for the VEGFA gene rs2010963 and rs69947 loci and the SOD2 gene rs4880 located on the same chromosome. The results showed that the VEGF gene rs2010963 and rs69947 sites and the SOD2 gene rs4880 site constructed GAC (OR = 1.17, 95% CI: 1.04-1.29), CAT (OR = 1.12, 95% CI: 1.03-1.60), and CAC (OR = 1.13, 95% CI: 1.01-1.24) had a higher risk of T2DN in haploids. By analyzing gene-environment interactions, it was found that the rs2010963 locus of the VEGFA gene, rs4880 locus of the SOD2 gene, BMI, and hypertension had a significant interaction with T2DN.
There are some shortcomings in this study. First, limited by the sample size, we only found an interaction between the rs2010963 locus of the VEGFA gene and the rs4880 locus of the SOD2 gene when analyzing gene-gene interactions. Second, the potential reason for the analysis of SOD2 gene polymorphism and T2DN susceptibility is the lack of detection of SOD2 protein levels, and the failure to construct an in vitro expression model is the main reason. In addition, a larger sample size should be examined to study more sites of interest.
Conclusion
Based on the results of this study, we found that genetic mutations in the rs2010963 and rs69947 loci in the VEGFA gene, rs4646994 locus in the ACE gene, and rs4880 locus in the SOD2 gene may lead to an increased risk of T2DN. These genetic variations may be involved in the occurrence and development of T2DN by affecting the expression and activity levels of related proteins.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from Traditional Chinese Medical science and technology plan of Zhejiang Province (2019ZA025).