
Abstract
Aims:
The prognostic significance of murine double minute 2 (MDM2) expression remains unknown in patients with upper tract urothelial carcinoma (UTUC). This study was designed to evaluate MDM2 expression and its association with clinicopathological characteristics and tumor outcomes in UTUC patients.
Materials and Methods:
Expression levels of MDM2 and p53 were determined by immunohistochemistry in a cohort of 341 UTUC patients. Associations of MDM2 and p53 expression levels with clinicopathological characteristics, disease-free survival (DFS), cancer-specific survival (CSS), and intravesical recurrence-free survival (IVRFS) were analyzed.
Results:
Nuclear expression of MDM2 and p53 were detected in the tumor cells of 129 (37.8%) and 203 (59.5%) patients, respectively. Decreased p53 expression was associated with positive MDM2 staining in tumor cells (p = 0.002). MDM2 expression was correlated with the exposure to aristolochic acids (p = 0.020), better preoperative renal function (p = 0.016), ureter location (p = 0.002), higher pathological T stage (p = 0.006), high tumor grade (p < 0.001), presence of glandular differentiation (p = 0.036), and sarcoma differentiation (p = 0.020). Kaplan-Meier analysis showed that positive MDM2 staining was associated with shorter CSS (p < 0.001), DFS (p < 0.001), and IVRFS (p = 0.020); MDM2+/p53− was associated with shorter CSS (p < 0.001) and DFS (p < 0.001), but not IVRFS (p = 0.145); while CSS, DFS, and IVRFS did not differ significantly between the p53+ and p53− patients (p = 0.307, 0.089, and 0.198, respectively). Multivariate analyses revealed that MDM2 expression in tumor cells independently predicted shorter CSS (p < 0.001; hazard ratio [HR] = 2.600; 95% confidence interval [CI]: 1.625-4.161) and DFS (p < 0.001; HR = 1.863; 95% CI: 1.314-2.641), excepting IVRFS (p = 0.092; HR = 1.590; 95% CI: 0.928-2.726).
Conclusions:
UTUC patients with elevated MDM2 expression may exhibit more aggressive biological features of the tumor and tend to have shorter CSS and DFS.
Introduction
Upper urinary tract urothelial carcinoma (UTUC), any carcinoma that arises from the urothelium of the urinary tract from the renal pelvis to the distal ureter, is relatively rare and accounts for only 5-10% of all urothelial carcinomas (Rouprêt et al., 2018; Siegel et al., 2019). However, UTUC has a high incidence in China and is often complicated by chronic tubulointerstitial disease or chronic kidney disease (CKD), possibly related to exposure to aristolochic acids (AAs) (Stiborova et al., 2016; Bara et al., 2017).
Radical nephroureterectomy (RNU) with excision of the bladder cuff is the standard procedure for UTUC patients (Li et al., 2008). Unfortunately, at the time of surgery, many UTUC patients are shown to have local advanced (60%) and high-grade (70%) tumors (Holmang and Johansson, 2005; Lughezzani et al., 2010). Previous studies have indicated that 5-year cancer-specific survival (CSS) ranges from 50% to 80% (Margulis et al., 2009; Favaretto et al., 2010). Developing novel treatments is crucial for UTUC patients, especially for those patients who are not suitable for chemotherapy. Investigators are anticipating that emerging targeted therapies may be an effective and promising treatment strategy for a number of malignancies.
It is known that tumorigenesis is a selection process encompassing both epigenetic and genetic changes that allow evasion of cell death-inducing and antiproliferative mechanisms (Bartkova et al., 2005). The majority of these genetic changes impact on the tumor suppressor p53-related pathway that guards against DNA damage and maintains genetic stability (Vogelstein et al., 2000). Murine double minute 2 (MDM2), a negative regulator of p53, suppresses the transcriptional activity of p53 inhibiting the p53-dependent cell cycle arrest and apoptosis. MDM2 expression is related to tumor grade and recurrence in superficial urothelial carcinoma of bladder (UCB) and the MDM2 gene expression is significantly associated with high tumor grade (Tuna et al., 2003). Recently, several inhibitors of the MDM2-p53 interaction have been identified, some of them are already in Phase I clinical trials (NCT01677780, NCT00559533, NCT01143740, NCT01164033, and NCT00623870) (Karni-Schmidt et al., 2016).
Therapies targeting the MDM2-p53 pathway are currently being evaluated for several malignancies. In contrast to the well-known tumorigenic connection of the MDM2-p53 pathway in various malignancies, the clinical value of the MDM2-p53 pathways has not been well reported in UTUC. As one of the largest urological institutes in China, we have conducted this study to identify the clinicopathological and prognostic significance of p53 and MDM2 expression in a cohort of UTUC patients in China.
Materials and Methods
Patient enrollment and evaluation
After approval by the internal Ethics Review Board of Peking University First Hospital (approval no. 2016[1253]), we retrospectively collected the records of 657 consecutive patients diagnosed histologically with UTUC, who received surgical treatment in Peking University First Hospital between January 2006 and December 2013. Three hundred sixteen patients were excluded from this study due to a lack follow-up data (n = 48); accompanying UCB (n = 79), and/or other malignancies (n = 13); receiving other treatment than RNU (n = 101); largest tumor size ≤15 mm (n = 75). Finally, 341 patients were enrolled. All of the patients underwent standard RNU with bladder cuff resection. Routine lymph node dissection was performed when enlarged lymph nodes were found via preoperative imaging or intraoperative observation.
Clinicopathological and follow-up data were collected and stored in a database containing the comprehensive medical records of UTUC patients. Exposure to AA was defined as a history of long-term exposure (>3 months) of intermittent intake of regular doses of AA-containing traditional Chinese medicine. Staging was assessed according to the 2002 Union for International Cancer Control (UICC) tumor, lymph node and metastasis classification guidelines. Patients were graded based on the World Health Organization (WHO) 2004 grading system. The estimated glomerular filtration rate (eGFR) was calculated using the modified GFR equation for Chinese patients [eGFR (mL/min/1.73 m2) = 175 × Scr-1.234 × age-0.179 ( × 0.79 if female)] (Ma et al., 2006). Preoperative renal function (PRF) was measured and recorded as no CKD (eGFR ≥60), early CKD (60 > eGFR ≥15), and end stage CKD (eGFR <15).
Follow-up protocol
For patients who underwent treatment at our institute, the follow-up regimen included cystoscopy every 3 months for the first 3 years. The cystoscopy intervals were extended to 1 year thereafter. Chest X-ray, urine cytology, serum creatinine test, and abdominal ultrasound or computed tomography (CT)/magnetic resonance imaging (MRI) were performed at the same time. CSS, disease-free survival (DFS), and intravesical recurrence-free survival (IVRFS) were determined at the last follow-up based on examination results. Overall survival was determined by review of the patient's medical records and from the Chinese National Statistical Office database.
Immunohistochemistry
Formalin-fixed paraffin-embedded (FFPE) blocks of 341 UTUC specimens were retrieved from the Department of Urological Pathology. Expression of MDM2 and p53 were evaluated by the standard immunohistochemistry (IHC) protocols. In cases where there were giant or multiple tumors, only the largest tumor specimen was processed for IHC analysis. In brief, 4 mm sections from all FFPE specimens were deparaffinized by xylene and rehydrated in decreasing concentrations of ethanol. Heat-induced antigen retrieval was performed using sodium citrate in a pressure-boiling container at 120°C for 20 min. After blocking endogenous peroxidase with 3% hydrogen peroxide in methanol, sections were incubated with 10% normal blocking serum in Tris-buffered saline for 20 min.
Based on preliminary evaluations, the sections were incubated overnight with an antibody against MDM2 (2A10, 1:2000; Abcam plc, Cambridge, UK) or an antibody against p53 (DO-1,1:2000; Abcam) followed by an incubation with a goat anti-rabbit IgG/horseradish peroxidase polymer (PV-9001, ZSGB-BIO, Beijing, China) for 20 min. The sections were then exposed to diaminobenzidine tetrahydrochloride solution and counterstained with hematoxylin.
Stained tissue sections were reviewed and scored by two independent urological pathologists who had no prior knowledge of the clinical data of this cohort (X.Y. and Q.H.). Reconciliation of disagreements was achieved by a multiheaded consensus review.
The German Immunoreactive Score (range 0-12) was calculated by multiplying the percentage of immunoreactive cells (0-5%, 0; 6-25%, 1; 26-50%, 2; 51-75%, 3; 76-100%, 4) by staining intensity (0, negative; 1, weak; 2, moderate; 3, strong) and specimens were considered negative (0, 0-1), weakly positive (+, 2-4), moderately positive (++, 6-8), or strongly positive (+++, 9-12). MDM2 and p53 positive was defined as + to +++ and ++ to +++, respectively.
Statistical analysis
All statistical tests were performed with SPSS 22.0 software (IBM Corp, Armonk, NY). Statistical significance was set as a p value <0.05. The Pearson's test and the chi-square test were used to determine the distribution of categorical variables and the Mann-Whitney U test was used for continuous variables. Survival curves of CSS, DFS, and IVRFS were plotted using the Kaplan-Meier method and analyzed by the log-rank test. Univariate analyses were assessed by the log-rank test, and multivariate analyses were evaluated using the Cox proportional hazard regression model.
Results
Associations of IHC-based expression levels of MDM2 and p53 with clinicopathological characteristics
The patient cohort included 190 men and 151 women with a median (range) age of 69 (29-86) years at the time of surgery and a median (range) follow-up of 51 (7-123) months after the surgery. The patient characteristics are summarized in Table 1. Nuclear expression of MDM2 and p53 was detected in the tumor cells of 129 (37.8%) and 203 (59.5%) patients, respectively (Fig. 1). Higher expression of MDM2 was correlated with lower expression of p53 (p = 0.002). The correlations of MDM2 and p53 expression levels with clinical characteristics of the patients are presented in Table 1. We found that being MDM2 positive was correlated with the exposure to AA (p = 0.020), better PRF (p = 0.016), ureter location (p = 0.002), higher pathological T stage (p = 0.006), high tumor grade (p < 0.001), presence of glandular differentiation (p = 0.036), and sarcoma differentiation (p = 0.020). Being p53 positive was significantly associated with female genders (p = 0.048), worse PRF (p = 0.040), and the presence of squamous differentiation (p = 0.007).
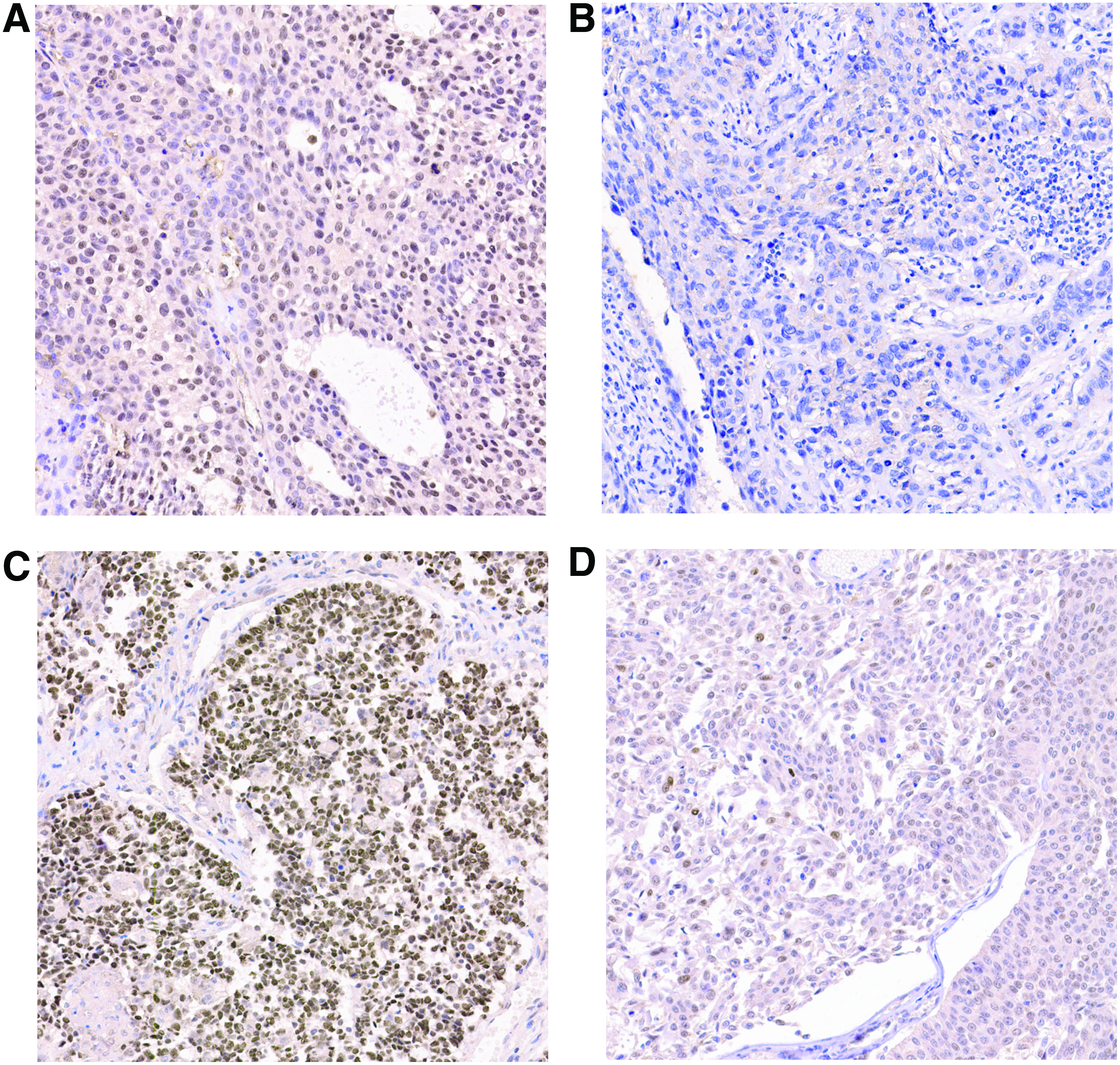
Representative cases of IHC expression (magnification 100 × ). Cases of IHC expression with
Associations Between MDM2 and p53 Expression and Clinicopathological Characteristics of the Patients
Statistically significant.
AA, aristolochic acid; BMI, body mass index; CKD, chronic kidney disease; LVI, lymphovascular invasion; MDM2, murine double minute 2; PRF, preoperative renal function.
MDM2 positive is an independent prognostic factor of poorer CSS and DFS
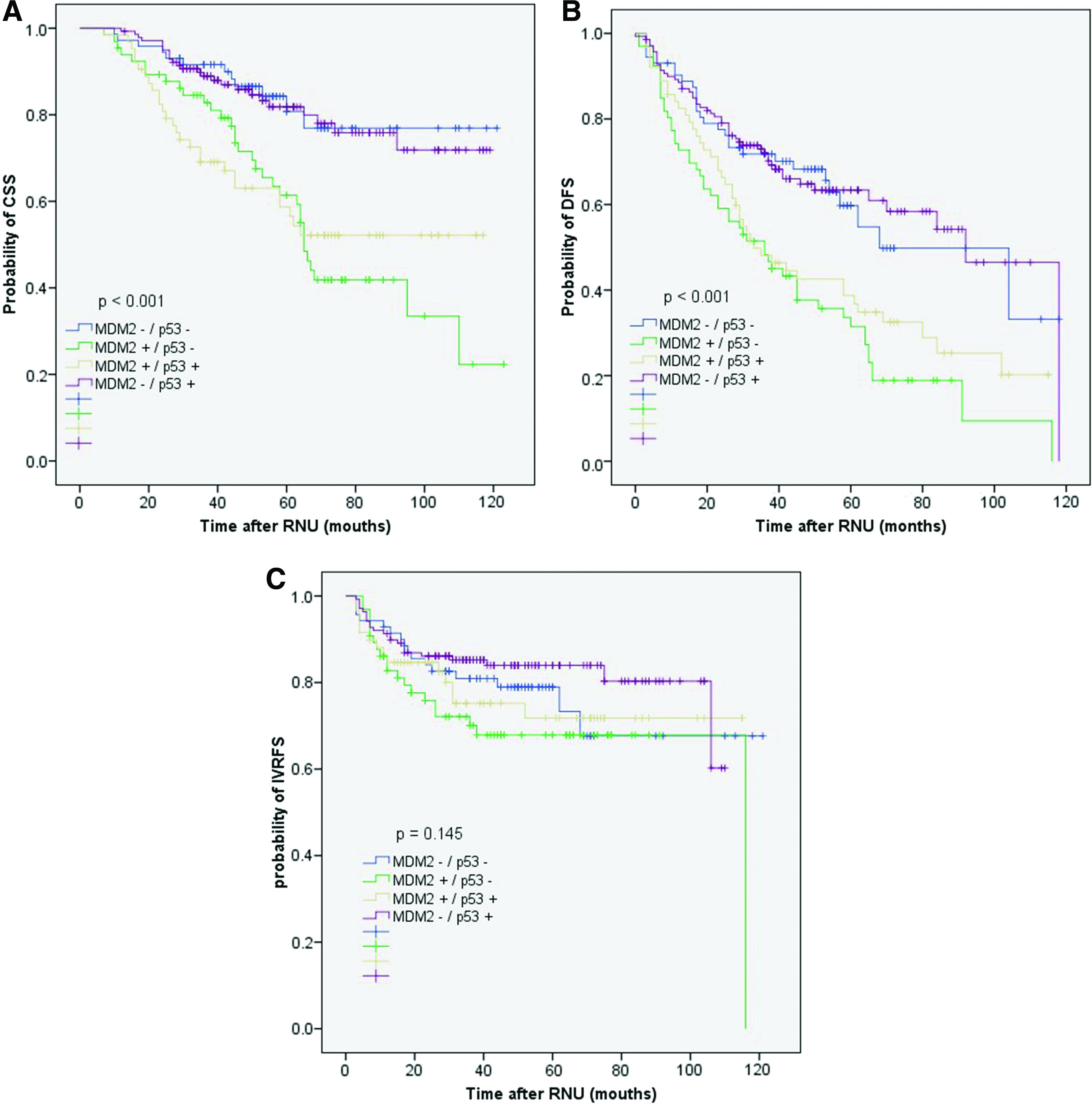
During the follow-up, 109 patients died (97 died due to UTUC-related causes) and intravesical and local recurrences occurred in 82 (24.0%) and 13 (3.8%) cases, respectively. Moreover, new contralateral UTUC occurred in 8 (2.35%) cases. Kaplan-Meier analysis showed that MDM2 positive was positively correlated with shorter CSS (p < 0.001), DFS (p < 0.001), and IVRFS (p = 0.020); MDM2+/p53− was associated with shorter CSS (p < 0.001) and DFS (p < 0.001), but not IVRFS (p = 0.145); while CSS, DFS, and IVRFS did not differ significantly between the p53-positive and p53-negative patients (p = 0.307 and 0.089, respectively) (Figs. 2-4). In the multivariate Cox model, adjusted for gender, pathological tumor stage, tumor grade, lymph node status, LVI, architecture, glandular differentiation, sarcoma differentiation, and exposure to AA, being MDM2 positive represented an independent risk factor for shorter CSS (p < 0.001; hazard ratio [HR] = 2.600; 95% confidence interval [CI]: 1.625-4.161) (Table 2). Furthermore, in the multivariate Cox model, adjusted for age, gender, tumor grade, lymph node status, and LVI, being MDM2 positive represented an independent risk factor for shorter DFS (p < 0.001; HR = 1.863; 95% CI: 1.314-2.641) (Table 3). In the multivariate Cox model, however, being MDM2 positive was not an independent risk factor for shorter IVRFS (p = 0.092; HR = 1.590; 95% CI: 0.928-2.726) (Table 4).
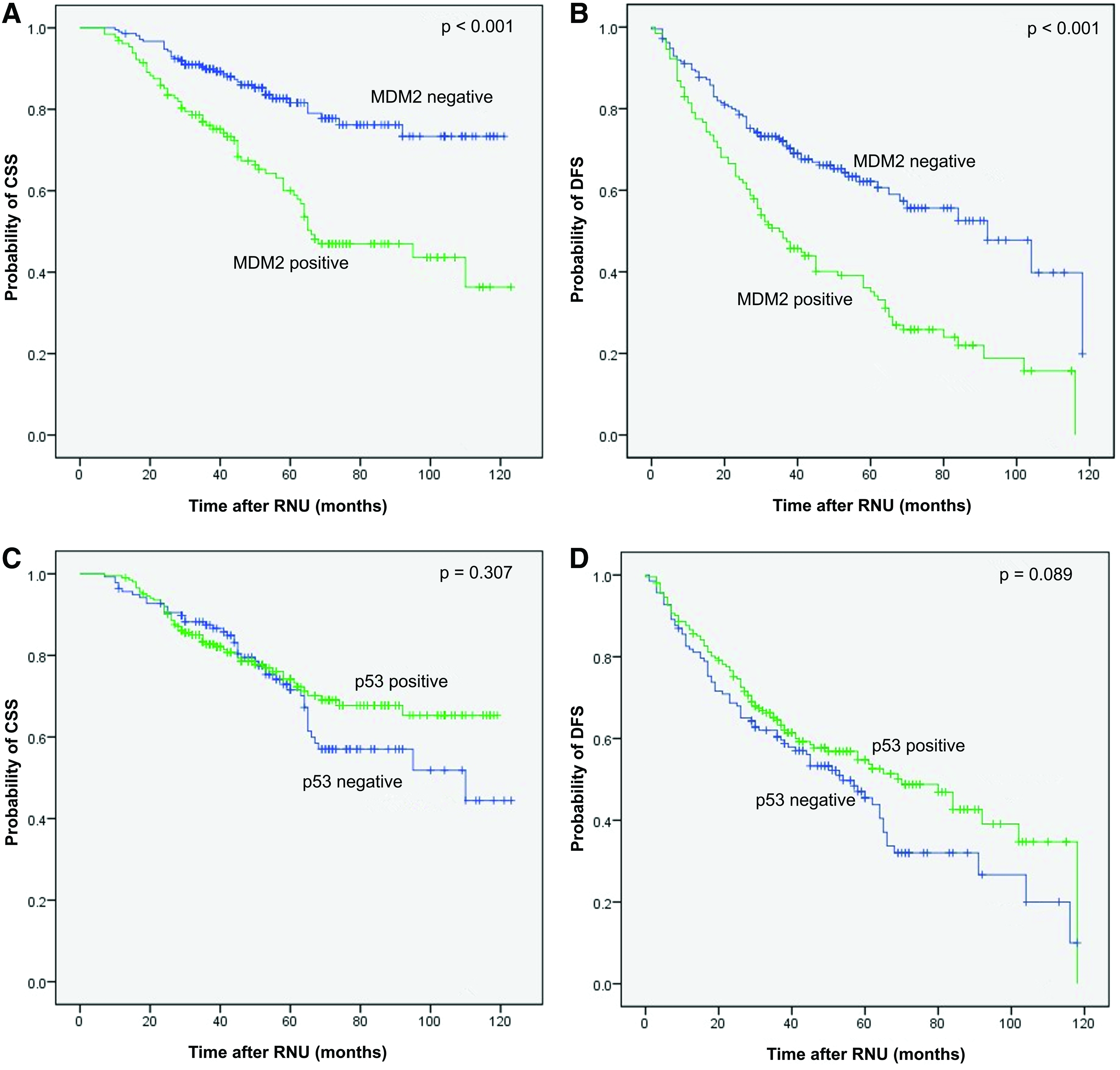
Survival curves for patients stratified with MDM2 and p53. The CSS curves stratified with
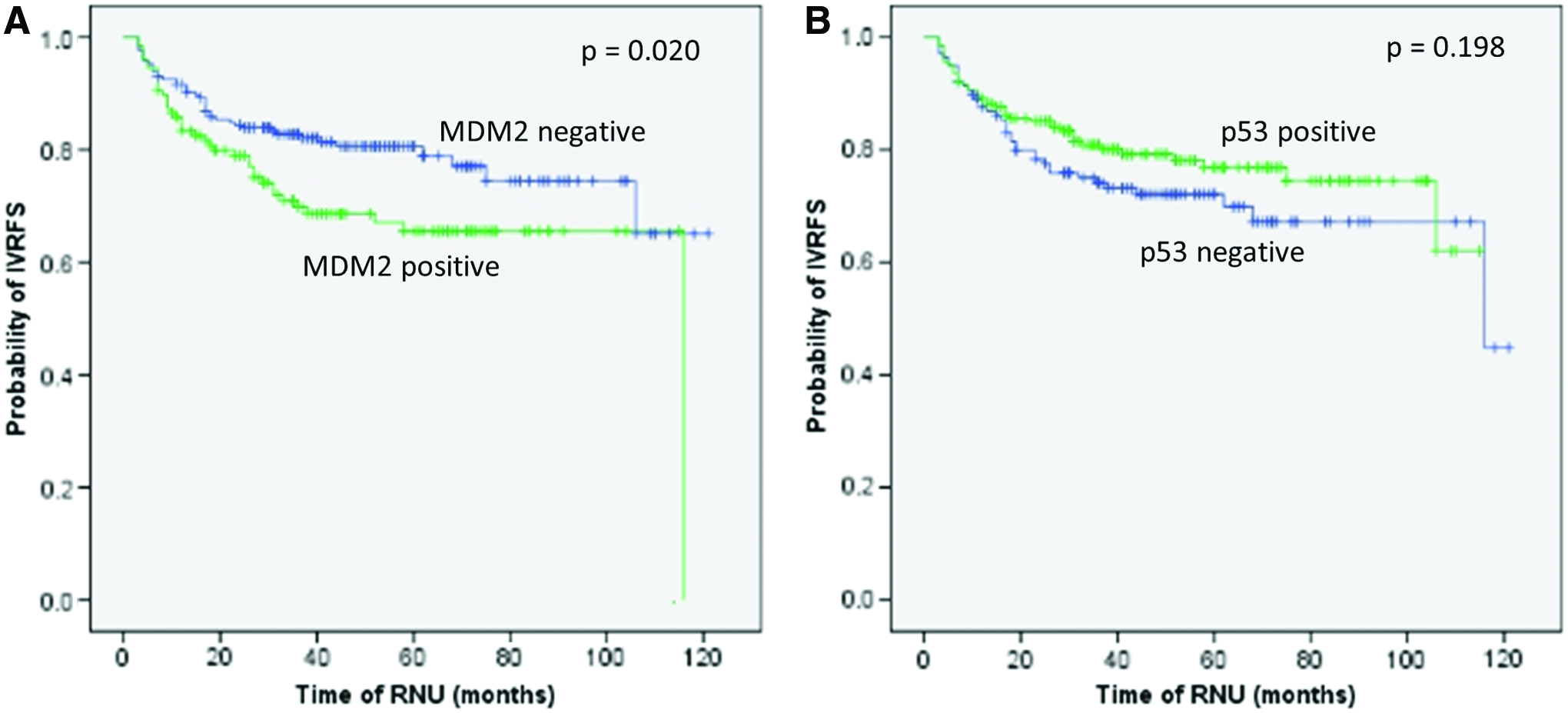
IVRFS curves for patients stratified with MDM2
CSS curves
Univariate and Multivariate Analyses of the Relationship Between MDM2 Expression and Cancer-Specific Survival in Patients With Upper Tract Urothelial Carcinoma
Statistically significant.
CI, confidence interval; HR, hazard ratio.
Univariate and Multivariate Analyses of the Relationship Between MDM2 Expression and Disease-Free Survival in Patients with Upper Tract Urothelial Carcinoma
Statistically significant.
Univariate and Multivariate Analyses of the Relationship Between MDM2 Expression and Intravesical Recurrence Free Survival in Patients with Upper Tract Urothelial Carcinoma
Statistically significant.
Discussion
The biological behavior of UTUC is dependent on several prognostic factors, including age, gender, race, smoking habits, PRF, tumor location, tumor stage, tumor grade, status of lymph node, LVI, architecture, and tumor necrosis (Rouprêt et al., 2018). Although these factors have been found to be the most important in predicting the progression and recurrence of UTUC, the biologic basis for UTUC is not completely understood. To our knowledge, this is the first study to demonstrate an association of MDM2 expression levels with clinicopathological factors and oncological outcomes in Chinese UTUC patients. Our results demonstrated that nuclear expression of MDM2 was correlated with important clinicopathological features, including tumor stage, tumor grade, and the presence of glandular and sarcoma differentiation; MDM2 positive is an independent predictive factor for lower CSS and DFS. Interestingly, the expression of p53 was confirmed to be negatively correlated with the expression of MDM2 although p53 had no predictive value for oncological outcome. Thus, even though the p53 pathway has been investigated for many years, the clinical significance of MDM2 may be more important at least in UTUC. This fact may be very informative for clinicians.
The interaction between MDM2 and p53 has been analyzed in other tumors. As one of the most important tumor suppressors, the p53 protein plays important roles in DNA transcription, cell growth, and proliferation (Thorsten, 2007). The p53 protein can interact with other members of the checkpoint control mechanisms to provide sufficient time to repair damaged DNA by inducing cell cycle arrest (Zhao et al., 2016; Lieberman et al., 2017; Lützkendorf et al., 2017; Sun et al., 2017). The human MDM2 gene is located at 12q13-14 (Shariat et al., 2012) and contains a p53 binding domain. MDM2 protein is an E3 ubiquitin ligase of p53 that triggers p53 degradation thus negatively regulating the p53 function (Honda et al., 1997; Aberrhandan et al., 2003; Ganguli et al., 2014; Cevik et al., 2015). p53, however, also controls the transcription of MDM2 resulting in a self-regulated feedback loop (Aberrhandan et al., 2003; Ganguli et al., 2014). Thus, an imbalance of the MDM2-p53 levels can result in uncontrolled cell growth and malignant transformation. MDM2 gene expression may be an early event in urothelial tumorigenesis. Based on our results, inhibitors of the MDM2-p53 interaction should be considered for the treatment of UTUC.
The prognostic role of MDM2 has been investigated in superficial bladder cancer, and MDM2 expression was found to be more common in papillary Ta tumors and in low-grade tumors (Tuna et al., 2003). However, the overall significance of MDM2 expression levels for predicting clinical outcomes following a diagnosis of UCB remains unclear. In addition, since there are obvious differences in response rates to chemotherapy and etiology between UTUC and UCB, UTUC is recognized as an uncommon type of UC that is potentially distinct from UCB (Patel et al., 2014). Therefore, whether the clinical significance of MDM2 expression in UCB can be equally applied in UTUC remains unknown and warrants further study, which makes the present study more significant.
In China, the consumption of AA is an important risk factor for development of UTUC and renal insufficiency. Certain unique characteristics of Chinese UTUC patients may be related to AA exposure, including high prevalence of CKD, high proportion of female patients, and high possibility of bilateral synchronous or asynchronous UTUC (Chung-Hsin et al., 2013; Xiong et al., 2015; Bara et al., 2017; Zhong et al., 2017). AA has been shown to induce preferential A:T-to-T:A transversions in the p53 gene in cell cultures and in rodent models (Zhipei et al., 2004; Feldmeyer et al., 2006). This transversion type was confirmed in human tumor samples of AA-related UTUC in the Balkans and Taiwan (Masaaki et al., 2011; Chung-Hsin et al., 2012; Jelaković et al., 2012; Stiborova et al., 2016). For decades, researchers have tried to identify the biomarkers of AA-related pathologies in patients, in addition to sequencing and to find specific targeted treatment options.
In the current study, patients with AA exposure tend to have higher possibility of positive p53 expression, although the differences were not statistically significant (71.8% vs. 57.9%, p = 0.097). It should, however, be noted that the expression of p53 was correlated with female gender and poor PRF which is in accordance with our previous findings which showed that female gender and poor PRF were associated with consumption of AA-containing herbs (Xiong et al., 2015). However, the expression of MDM2 was correlated with lower exposure to AA and relatively better PRF in agreement with the role of MDM2 as a negative regulator of p53. Considering possible high prevalence of AA exposure in Chinese patients (and in Balkan region), it can be postulated that the p53-MDM2 pathway plays an important role in carcinogenesis and the inhibitors of the MDM2-p53 interaction may be a useful treatment option.
In the present study, nuclear expression of P53 was detected in tumor cells of 203 (59.5%) patients, which is higher than 28-47% reported in previous studies (Lee et al., 2015). Our date indicated that CSS, DFS, and IVRFS did not differ significantly between the p53+ and p53− patients. Bagrodia et al. (2016) detected TP53/MDM2 alteration via next-generation exon capture sequencing in 83 patients with UTUC, and found that mutations in TP53 and TP53/MDM2 alteration significantly increased the risk of death from disease. A review conducted by Lughezzani et al. (2012) revealed that p53 was a prognostic predictor in univariate analyses, but it was not an independent prognostic factor after adjustment for other clinicopathological characteristics. Those studies were limited by small numbers and lack of validation. Routine laboratory tests have not been carried out to determine whether p53 is expressed in UTUC. Due to a small number of available patients and the lack of comparative studies on survival, p53 expression in UTUC has not been investigated extensively. There are two possible reasons for the release of various results in each report. First, sample size is a limiting factor in most of these studies. The average number of patients included in the existing studies was 90.91 (range 53 − 149). As a result, the statistical validity of these studies could be a matter of debate. Second, the analytical methods used to assess p53 expression differed between the studies, which may lead to potential statistical bias. Thus, further study is necessary to investigate the role of p53 in the carcinogenesis of UTUC.
In our study, we have optimized our IHC protocols by conducting preliminary tests and thus ensuring that the protocol was reliable and reproducible. The results of the study will be useful in investigation of the role of MDM2-p53 in carcinogenesis and in future targeted treatments. However, some important limitations should be noted. First, the study represents a retrospective review of the data at a single center and thus may be related to selective and recall bias and may require further external validation (especially from non-Chinese cohorts). Second, the accuracy of the study was affected by the use of a single method of IHC and other techniques (e.g., real time-polymerase chain reaction or sequencing of genetic mutations) may increase the significance of this work.
In conclusion, UTUC patients with elevated MDM2 expression have more aggressive biological features of the tumors and tend to have shorter CSS and DFS. We recommend validating the clinical significance of MDM2 expression in the studies in a large cohort of metastatic UTUC patients who are more likely to benefit from targeted therapies against MDM2; we anticipate clinical trials that will explore the efficacy and feasibility of targeted against MDM2 in UTUC patients.
Footnotes
Acknowledgments
The authors thank the entire staff of Department of Urology, Peking University First Hospital Structured data processing occurred partially using Medbanks' approach (Medbanks [Beijing] Network Technology Co., Ltd.).
Authors' Contributions
Z.B., S.H.: protocol/project development, data collection and management, drafting the article, and data analysis; D.F.: protocol/project development, revision of the article and supervision. B.G., L.Z., G.X.: data collection and management. X.Y., Q.H.: protocol/project development; X.L.: revision of the article. L.Z.: protocol/project development and supervision.
Ethical Approval
This study was approved by the Ethics Committee of Peking University First Hospital, Beijing, China (approval no. 2016[1253]). All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Research Committee and the 1964 Declaration of Helsinki and its later amendments.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Beijing Natural Science Foundation (L182004, 7152146), the clinical features research of Capital (no. Z151100004015173), the Capital Health Research and Development of Special (2016-1-4077), and the Peking University Medicine Fund of Fostering Young Scholars' Scientific and Technological Innovation (Fundamental Research Funds for the Central Universities, BMU2017PY009).