
Abstract
Introduction:
Interleukin-6 (IL-6) is a circulating proinflammatory cytokine that fulfills an important role in the survival and proliferation of cancer cells. Overexpression of IL-6, possibly due to the −174G>C and −596G>A polymorphisms in the IL6 gene, has been shown to be related to breast cancer (BC) and a more aggressive course of the disease.
Aim:
To determine the influence of the −174G>C and −596G>A polymorphisms of the IL6 gene on the circulating levels of IL-6 in BC patients from Jalisco, México.
Methodology:
Genotyping of the two polymorphisms was carried out on 208 BC patients and 219 healthy controls through polymerase chain reaction-restriction fragment length polymorphism analyses. In addition, the plasma IL-6 concentration levels were measured in the BC patients.
Results:
There was no significant association between BC and the IL-6 alleles and genotypes (−174G>C, p = 0.276; −596G>A, p = 0.762) under study. Similarly, there were no significant differences in the mean plasma IL-6 concentrations associated with the polymorphisms that were analyzed (−174G>C, p = 0.839; −596G>A, p = 0.848).
Conclusions:
No evidence was found that the analyzed polymorphisms are associated with the IL-6 expression or concentration in patients suffering from BC from Jalisco, Mexico.
Introduction
The incidence of breast cancer (BC) continues to rise on a worldwide basis (Bray et al., 2018); in 2014 the “Instituto Nacional de Estadistica Geografia e Informatica” identified BC as the leading cause of cancer-related deaths for women in México (INEGI, 2018). Several studies have contributed to establish the tumor microenvironment as a heterogeneous population of neoplastic and stromal cells recruited by cancer clones. The stromal cells respond to localized hypoxia and necrosis by producing growth factors, chemokines, and cytokines that favor tumor progression (Bussard et al., 2016). Among the produced proinflammatory cytokines, interleukin 6 (IL-6) is thought to play a major role in mediating the cancer-inflammation relationship (Grivennikov et al., 2010). Furthermore, pleiotropic effects of IL-6 have been shown that favor angiogenesis, cellular proliferation and survival, evasion of immunological surveillance, and stimulation of estrogen synthesis in malignant tissue (Purohit et al., 2002; Fisher et al., 2014). In BC, IL-6 is associated with lymph node infiltration, an advanced tumor stage and recurrence, and has even been suggested as a predictive factor for endocrine therapy (Cho et al., 2013; Ma et al., 2017; Raghunathachar Sahana et al., 2017; Milovanovic et al., 2018). In addition, increased serum levels of IL-6 have been shown to be related to high levels of nuclear factor kappa beta (NF-κβ) light chain enhancer of activated B cells, which may be associated with tumor resistance to treatment. Moreover, IL-6 stimulates aromatase expression in adipose tissue, which then stimulates estrogen synthesis that can promote progression of BC (Markkula et al., 2014). IL-6 gene expression is NF-κβ dependent, upregulated by adipokines, interleukin-1beta (IL-1β), tumor necrosis factor-alpha(TNF-α), transforming growth factor-beta1 (TGF-β 1), and other transcription factors such as JunD, Cyclic AMP-Responsive Element-Binding Protein 1 (CREB1), and c-Jun depending on cell type and the microenvironment (Gyamfi et al., 2018).
In this study, we investigated the −174G>C and −596G>A polymorphisms of the IL6 gene (rs1800795 and rs1800797, respectively), which have been associated with alterations to transcription factor binding motifs and which may explain the differences in cytokine concentrations in BC patients from Jalisco, Mexico.
Materials and Methods
This study was carried out on 218 Mexican women aged ≥18 years who had been diagnosed with BC (BC group). All BC patients were histologically confirmed as part of the “ELLA Binational Breast Cancer Study,” a multicenter study designed to look for breast tumor molecular markers, clinicopathological characteristics, and risk factors in women of Mexican descent (Martínez et al., 2012). A control group of 209 healthy women (HCs) aged 18-60 years without any history or laboratory evidence of infectious, inflammatory, cardiac, and renal diseases were also enrolled. All study participants were born in the state of Jalisco.
After providing signed consent, DNA was extracted from peripheral blood specimens of all study participants according to the method described by Miller et al. (1988). In brief, cells were disrupted with a lysis buffer and digested overnight at 37°C using sodium dodecyl sulfate and protease K solutions. DNA purification was achieved through protein precipitation with a saturated sodium chloride solution. The supernatant containing the DNA was then precipitated with absolute ethanol. DNA was dissolved at 37°C and quantified (reagents purchased from IBI Scientific, Dubuque, IA). Polymerase chain reaction (PCR) was performed with the following primers (−174F-AATGACGACCTAAGCTGCACT, −174R-TTGAGACTCATGGGAAAATCC; −596F-GAGACGCCTTGAAGTAACTG, −596R-GTTCTGAACTGAGTTTCCTCTGACTC; Invitrogen, Waltham, MA). Each reaction comprised 20 ng of genomic DNA, 2 mM MgCl2, 1 × reaction buffer, 10 nM of each dNTP, 500 nM of each primer pair, and 1 U of recombinant Taq DNA Polymerase (all reagents were purchased from Invitrogen). PCRs were carried out after an initial denaturation step at 94°C for 5 min, followed by 31 amplification cycles (94°C for 30 s, 60°C for 30 s, and 72°C for 30 s) and then a final extension step at 72°C for 7 min on a Veriti 96-well Thermal Cycler (Applied Biosystems, Waltham, MA). Genotyping was performed with NlaIII and BtsCI restriction enzymes (New England Biolabs, Ipswich, MA) to identify the −174G>C and −596G>A polymorphisms, respectively. To visualize the generated fragments, electrophoresis was performed in 6% of 29:1 polyacrylamide gel (IBI Scientific) and resolved at 200 V for 40 min.
Demographic data from BC patients were collected for correlation with disease stage. Plasma IL-6 concentrations were measured using a Human IL-6 ELISA kit (BioLegend, San Diego, CA).
Using the genotypic data, a Hardy-Weinberg equilibrium (HWE), association analysis of genotypes and alleles was performed using χ2 tests. Linkage disequilibrium was ignored due to the proximity of the variants (422 bp between them). The distribution curve of the IL-6 plasma concentration was assessed with Kolmogorov-Smirnov tests, and Kruskal-Wallis test was utilized to establish the association between genotype and IL-6 concentration or a Mann-Whitney U-test for the association with demographic data. Statistical analyses were performed in SPSS v22 software (IBM, Armonk, NY), applying an alpha of 0.05.
Results
The number of individuals who were genotyped differed in the two groups due to depletion of samples, resulting in data from 408 individuals analyzed for the −174G>C polymorphism (200 HCs and 208 BC), and data from 416 individuals for the −596G>A (200 HCs and 216 BC) polymorphism. The two IL6 gene polymorphisms studied (−174G>C p = 0.632; −596G>A: p = 0.872) were found to be in HWE for HCs. This means that the studied variants were not subject to genetic drift events in the HC population. The frequencies of the alleles and genotypes for both groups, as well as the results of the association test for the allelic and codominant inheritance model, are given in Table 1.
Allele and Genotype Frequencies, and the Results of the Association Test
Allelic model.
Codominant inheritance model.
BC, breast cancer; HC, healthy control; CI, confidence interval; OR, odds ratio; p, significance defined by the χ2 test.
Stratification of the BC population was carried out according to the prognostic markers of disease, and associations were established between the presence of polymorphisms and menopausal status, pathological stage, metastasis, and molecular phenotype. Statistical tests were applied to stratified groups to attribute associations between subgroups and the HCs. None of the prognostic markers were associated with any of the polymorphisms studied (see Table 2 for demographic data of patients and for results of association tests).
Demographic Data for Breast Cancer Patients and the Result of the Association Test
Significance as assessed with the χ2 test.
χ2 test versus the HCs group.
Significance assessed with the Mann-Whitney U-test.
NA, test not performed; TNBC, triple negative breast cancer.
Standard control measurements of plasma IL-6 had a correlation coefficient R2 = 0.9845. The concentrations measured did not follow a normal distribution according to the Kolmogorov-Smirnov test (p = 1.019 × 10-41) and the overall mean for this measurement was 7.654 pg/mL (see the box plot of plasma IL-6 concentrations for each genotype in Fig. 1). A Kruskal-Wallis test showed that distribution of IL-6 concentrations was not significantly associated with either genotype (−174G>C p = 0.839; −596G>A p = 0.848).
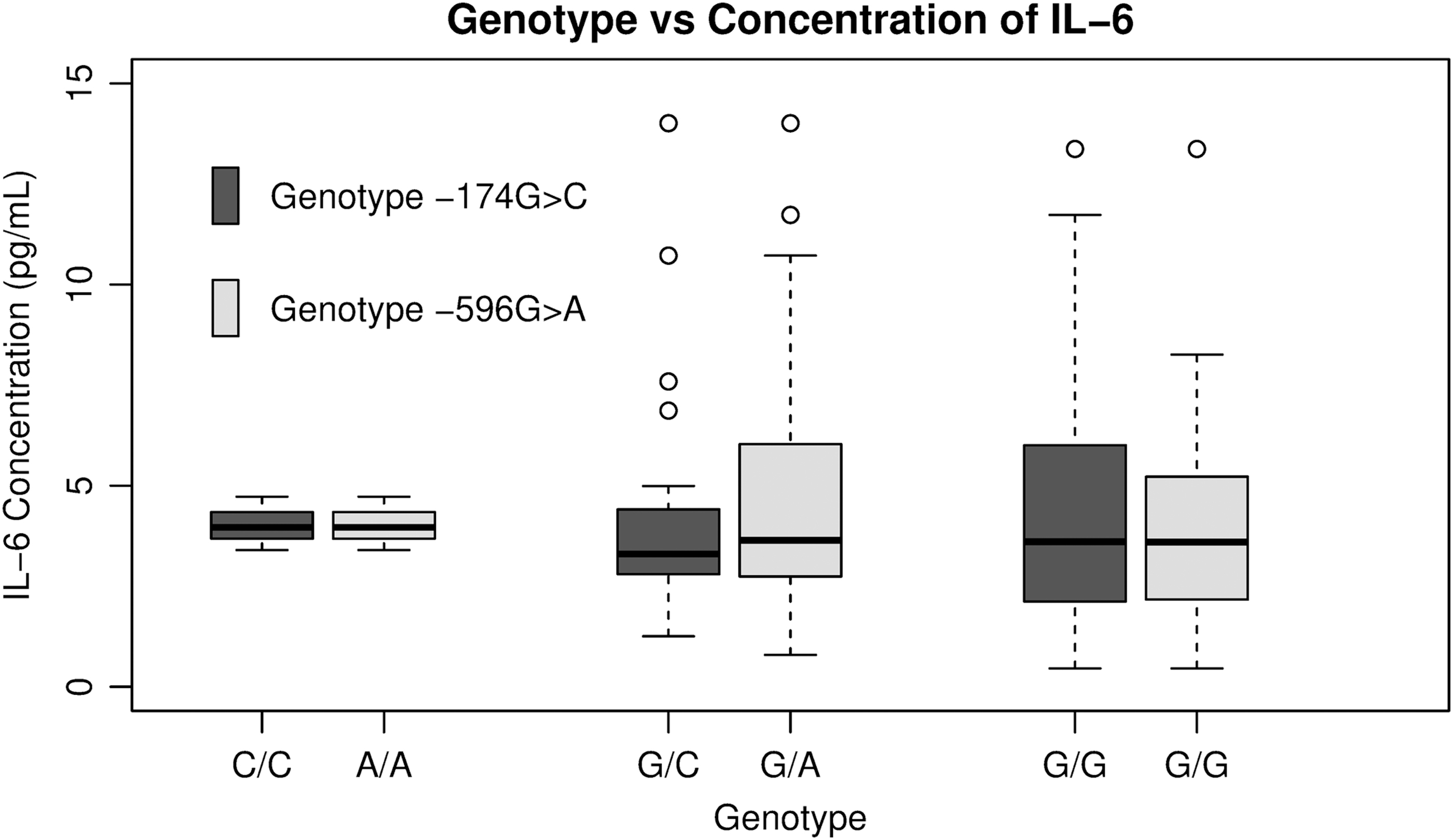
Plasmatic concentration of IL-6 by genotype. Average concentration for each genotype with 95% confidence interval. IL-6, interleukin-6.
Discussion
The majority of mammary tumors stimulate their growth in an estrogen-dependent manner, and it is thought that IL-6 favors tumor progression by enhancing aromatase, estrone sulfatase, and estradiol-17β-hydroxysteroid dehydrogenase type 1 activity, all enzymes involved in synthesis of estradiol (Purohit et al., 2002). The C and A alleles of the −174G>C and −596G>A IL6 polymorphisms are believed to alter transcription factor binding motifs in the IL6 gene, modifying IL6 expression and thereby altering estrogen synthesis (Terry et al., 2000; Gyamfi et al., 2018). This model, however, does not appear to be linear, nor can it be extrapolated to all populations, as shown in an earlier meta-analysis wherein ethnic origin was seen to influence the association between the −174G>C polymorphism, the risk of cancer, and the IL-6 concentration (Liu et al., 2012; Tian et al., 2015). Our current results are consistent with the concept of cancer as a complex multifactorial disease that involves genetic, environmental, and lifestyle factors. According to a binational American Mexican study, the IL-6 gene polymorphisms were associated with BC only among women with minimal Native American ancestry (Slattery et al., 2014). Our results are consistent with this study, due to the reported Amerindian ancestry of the population of Jalisco (range 31.5-46.7%) (Salazar-Flores et al., 2015; Mendoza-Carrera et al., 2017). In addition, there were no differences in plasma IL-6 concentrations associated with the studied polymorphisms, although there was a slight trend toward lower concentrations in patients carrying the −174C and −596A polymorphisms of the IL6 gene.
A study of regulatory variants as potential prognostic biomarkers demonstrated an extensive variability between Egyptian (AlSuhaibani et al., 2016) and Thai (Sa-Nguanraksa et al., 2016) ethnic groups. There was an association between the −174G>C polymorphism (C allele) with BC and a greater involvement of lymph nodes in carriers of the CC genotype. Furthermore, lower disease-free survival was observed for carriers of the AA genotype with the −596G>A polymorphism in the Thai population. To establish a prognostic association with the polymorphisms examined in this study, we included data from the BC group regarding menopausal status, pathological stage, metastasis, and molecular phenotype. There was, however, no significant relationship between the polymorphisms and any of the prognostic variables, indicating that a relationship between the variants and these potential prognostic markers could not be established for the studied population.
Plasma IL-6 concentrations may differ in distinct clinical stages of BC, and may be dependent on individual characteristics such as menopausal status and metastasis. In a Chinese population (Ma et al., 2017), plasma IL-6 levels were correlated with ductal carcinoma clinical stages II and III, patients with lymph node metastasis, and estrogen receptor expression in tumors and HER2+ ductal carcinomas. In an Indian population, IL- 6 was observed to be overexpressed in BC, stratifying the diseased population and displaying significant differences when analyzing the groups according to their clinical stage (Raghunathachar Sahana et al., 2017). Association between high levels of IL-6 and an improved clinical prognosis was observed in patients of Serbian origin (Milovanovic et al., 2018), suggesting sensitivity to endocrine therapy. In our study, IL-6 levels were not associated with menopausal status, pathological stage, metastasis, or the patient molecular phenotype, implying that there is no relationship between plasma IL-6 concentrations and these markers in the Mexican population. It is important to highlight that the genotypic frequencies are similar to those previously reported in the Mendoza-Carrera study (Mendoza-Carrera et al., 2017). In addition, the comparison of genotypic frequencies of HCs does not differ from those reported in 1000 genomes project (−174G>C: p = 0.1985; −596G>A: p = 0.2435) (Clarke et al., 2017).
To translate these research findings to clinical oncology, it is important to take into account not only the genetic factors but also the epigenetics and the environment. It has been reported that obesity is associated with increased levels of IL-6 (Ouchi et al., 2011). Our group demonstrated an association between obesity and parity as risk factors for BC in Mexican women from the ELLA Binational Breast Cancer Study (Martínez et al., 2012).
This study is not without its limitations as there was a lack of a control group for IL-6 circulating levels and the number of samples analyzed was not large. The strength of the study relies on the systematic epidemiological, clinicopathological, and molecular information of the ELLA Binational Breast Cancer Study and the analysis according to menopausal status, clinical stage, and molecular phenotype.
Conclusions
In the population studied, there was no significant evidence associating the −174G>C and −596G>A polymorphisms of the IL6 gene with BC or its prognostic markers. Also, there was no influence of these polymorphisms on the plasma concentration of IL-6 in these patients.
Ethical Approval
This study was conducted conforming to the declaration of Helsinki and the research was approved by the ethical investigation committee from each hospital and Universidad de Guadalajara (CI-9708).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors express their gratitude to Ella Binational Breast Cancer Study, Avon Mexico: Promesa Cáncer 2019, the PROMEP-SEP Program, and the Postgraduate Doctorate Program in Human Genetic, Centro Universitario de Ciencias de la Salud, Universidad de Guadalajara for funding.