
Abstract
Aims:
To investigate the expression levels of serum interleukin-17 (IL-17) and interleukin-27 (IL-27) in children with bronchial asthma and to correlate these expression levels with lung function indicators.
Methods:
A total of 106 children with bronchial asthma (observation group: 76 in the acute attack phase, 30 in remission) and 60 healthy children (control group) aged 1-10 years were enrolled.
Results:
Levels of IL-17, IL-27, and fractional exhaled nitric oxide (FeNO) in the peripheral blood of children with bronchial asthma were higher compared to the control group. In addition, blood IL-17, IL-27, and FeNO levels in the children in the acute stage of bronchial asthma were higher compared with those in remission. The respiratory rate of children in the remission stage was lower compared with those in the acute stage, however, the other indicators were higher. IL-17, IL-27, and FeNO levels positively correlated with the respiratory rate and were negatively correlated with inspiratory time, expiratory time, peak time, and time to reach peak tidal expiratory flow/total expiratory time (TPTEF/TE; all p < 0.05).
Conclusion:
IL-17 and IL-27 levels are associated with the incidence and the development of bronchial asthma in children, and could be useful diagnostic markers. They may also effectively improve the specificity of FeNO for diagnosing the extent of lung injury in children.
Introduction
Bronchial asthma in children is mainly caused by chronic inflammation of the airway. Pathophysiological abnormalities related to bronchial asthma include airway hyperresponsiveness, inflammation, tissue reconstruction, and increased thickness of the reticular basement membrane. It also leads to an increase in the smooth muscle mass that is often accompanied by the variable limited expiratory flow. Around 70-80% of the bronchial asthma cases occur in children aged 4-5 years. Bronchial asthma is one of the most common causes of repeated cough in children (Mochizuki et al., 2017; Ostergaard et al., 2018). With changes in lifestyle and increases in environmental pollution, the incidence of bronchial asthma in children has been continuously rising. In addition to this, disease severity may further deteriorate in about 30-54% of the currently inflicted children. Such changes can lead to typical bronchial asthma that greatly affects children's learning and the overall development of their physical and mental healths (Yoshihara et al., 2015; Joschtel et al., 2018). Children suffering from bronchial asthma need active clinical intervention to prevent irreversible airway stenosis and airway remodeling. Early diagnosis is, hence, very important for the treatment and subsequent improvement in their lung function.
Currently, the gold standard for the diagnosis of airway inflammation in bronchial asthma is either endobronchial biopsy or bronchoscopic support tube lavage but they have certain limitations in clinical use. Complicated procedures, high trauma, and medical costs are its major disadvantages (Korevaar et al., 2015; Liu et al., 2015). Serological diagnosis has always been preferred by clinical researchers because it has the advantages of simplicity, noninvasiveness, and high specificity. Increase in the levels of fractional exhaled nitric oxide (FeNO) is a potential marker for the diagnosis and treatment of asthma in children (Chien et al., 2013; Lezmi et al., 2018). In a previous study, interleukin-17 (IL-17) was reported to be involved in the development of asthma. Compared to normal children, asthmatic children had significantly elevated levels of serum IL-17 that correlated with the severity of the disease. Xie et al. (2015) have found that the messenger RNA (mRNA) and protein expression levels of IL-17 in the alveolar lavage fluid of asthma patients were significantly increased and positively correlated with disease severity. Li et al. found that interleukin-27 (IL-27) was elevated in induced sputum in patients with steroid-refractory asthma. The underlying mechanism of this steroid resistance was identified as the activation of the MyD88-dependent pathway by IL-27 and IFN-γ in macrophages. The integrated signal from IL-27/IFN-γ inhibited the glucocorticoid-induced transport of the glucocorticoid receptor to the nucleus of the macrophage that induced airway hyperresponsiveness (Li et al., 2010). These studies have, therefore, reported the close relationship of IL-17 and IL-27 in asthma but its diagnostic value in asthma is still undefined.
We hypothesized that IL-17 and IL-27 were closely related to the incidence and development of bronchial asthma in children, and therefore, analyzed the relationship between IL-17 and pulmonary function indicators in asthmatic children to explore their diagnostic efficacy.
Materials and Methods
Recruitment of subjects
Children with bronchial asthma were enrolled in the observation group in addition to a control group consisting of healthy children. Inclusion criteria: children in the observation group were enrolled according to the diagnostic criteria of the 2017 Global Initiative for Asthma (Brusselle et al., 2017). Children suffering from the acute stage of bronchial asthma had a higher frequency of coughs; or had difficulty lying on their backs; or had an obvious nasal flaring; or could not quietly fall asleep at night; or had the presence of rales in the lungs, and others. Patients with atypical clinical symptoms had a positive bronchial provocation test or exercise test. There were no clinical symptoms in the children in remission. The enrolled children provided their complete medical history and had no history of allergic diseases, any recent glucocorticoid treatment, drug allergy, or respiratory diseases. Exclusion criteria: Children who had symptoms of wheezing, shortness of breath or cough caused due to other diseases; or children who were previously treated with anti-IgE antibodies and other antiasthmatic drugs or glucocorticoids; or children with abnormal bleeding/coagulopathy combined with cardiovascular and cerebrovascular diseases or in combination with liver and renal function diseases or combined with digestive tract diseases; or children who were transferred to the hospital midway during an attack; or children whose relatives did not cooperate with the treatment; or children who had mental disorders were excluded from the study. All healthy children enrolled in the control group had no specific diseases such as allergic rhinitis, bronchial asthma, acute respiratory infections, and had no family history of allergies during the week before the initiation of the study. The study was approved by the Ethics Committee of the Children's Hospital of Chongqing Medical University and the patient or their family member signed the informed consent form.
Detection method
Peripheral blood of the subjects on fasting conditions was collected by nurses and sent for analysis within 1 h of collection. IL-17 and IL-27 were measured in the blood using enzyme-linked immunosorbent assay according to the kit instructions (Shanghai Hengfei Biotechnology Co., Ltd.). FeNO was measured using the PGM-1860 type ToxiRAE Pro EC Nitric Oxide Detector (Beijing Oriental Haitai Technology Co., Ltd.) in accordance with the standards set by the European Respiratory Society/American Thoracic Society. Lung function test was performed using the MINATO lung function meter AS-507 (Shanghai Jumu Medical Devices Co., Ltd.) according to the instructions. All measurements in the study groups were recorded after the diagnosis of the disease and before initiating treatment.
Statistical analysis
SPSS 19.0 (Asia Analytics Formerly SPSS China) was used for all the statistical analyses. The enumeration data were expressed as n (%) and the ratios were compared using the χ2 test. The measurement data were expressed as mean ± standard deviation. Comparison between the two groups was performed by independent sample t-test whereas comparisons between multiple groups were analyzed by analysis of variance. The post hoc test was performed by least significant difference test. The ROC curve was used to analyze the diagnostic value of IL-17, IL-27, and FeNO in the acute asthmatic children. The diagnostic value of FeNO in combination with IgE in asthmatic children was analyzed by a logistic regression model. Pearson's correlation analysis was performed for investigating the association of IL-17 and IL-27 in combination with FeNO and lung function. The differences were considered statistically significant when p < 0.05.
Results
Characteristics of the study cohort
A total of 60 children were enrolled in the control group, including 31 boys (51.67%) and 29 girls (48.33%). Their age, body weights, and heights were 5.24 ± 1.33 years, 35.27 ± 12.68 kg, and 142.66 ± 17.63 cm, respectively. A total of 106 children were recruited in the observation group, in which there were 58 boys (54.72%) and 48 girls (45.28%). Their ages, body weights, and heights were 5.19 ± 1.58 years, 33.56 ± 10.59 kg, and 144.13 ± 17.82 cm, respectively. There were no significant differences in the age, height, and weight between the two groups (all p > 0.05). The average disease course and severity in the children of the observation group are shown in Table 1.
General Data
IL-17 and IL-27 plasma levels with asthma and disease status
The serum levels of IL-17 and IL-27 in the peripheral blood of children with bronchial asthma were significantly higher compared with those in the control group (both p < 0.05). The levels were also higher in the acute stage of disease compared with those in the remission stage (both p < 0.05) (Table 2).
Results of Interleukin-17 and Interleukin-27 Detection
Compared with the acute stage, ap < 0.05.
Compared with the ressimion stage, bp < 0.05.
IL-17, interleukin-17; IL-27, interleukin-27.
FeNO plasma levels with asthma and disease status
The levels of FeNO in the peripheral blood of children with bronchial asthma in both the acute or remission stages were higher compared to those in the control group (both p < 0.05). Also, the FeNO levels were higher in children with acute stage asthma compared with those in the remission stage (p < 0.05) (Fig. 1).
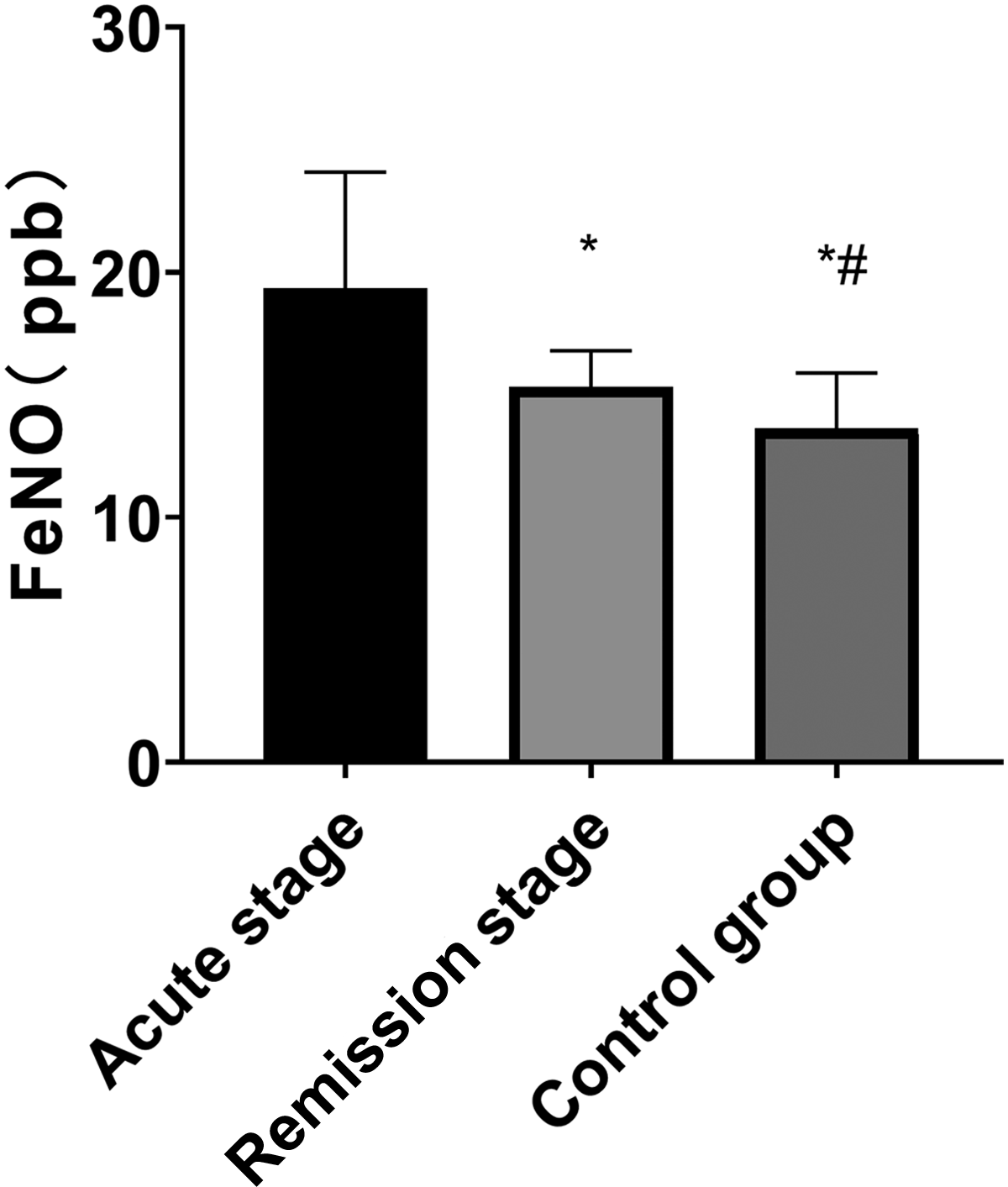
Results of FeNO detection. Compared with the acute stage, *p < 0.05; compared with the remission stage, #p < 0.05. FeNO, fractional exhaled nitric oxide.
The effectiveness of IL-17, IL-27, and FeNO in the diagnosis of bronchial asthma in children
ROC curve analysis showed that the area under the curve for diagnosis of bronchial asthma in children using IL-17 was 0.772 (95% confidence interval [CI], 0.693-0.850). When the IL-17 level was 77.43 pg/L, the sensitivity was found to be 50.73% while the specificity was found to be 80.56%. The area under the curve for diagnosis of bronchial asthma in children using IL-27 was 0.702 (95% CI, 0.615-0.790). When the IL-27 level was 18.55 ng/L, the sensitivity and specificity were found to be 75.00% and 65.79%, respectively. The area under the curve for diagnosis of bronchial asthma using FeNO in children was 0.838 (95% CI, 0.769-0.907). When the FeNO level was 17.23 ppb, the sensitivity was found to be 98.45% and the specificity was found to be 64.47%. The area under the curve for the diagnosis of bronchial asthma in children using all the markers was 0.917 (95% CI, 0.873-0.961), and the sensitivity and specificity were found to be 96.67% and 83.68%, respectively (Table 3 and Fig. 2).
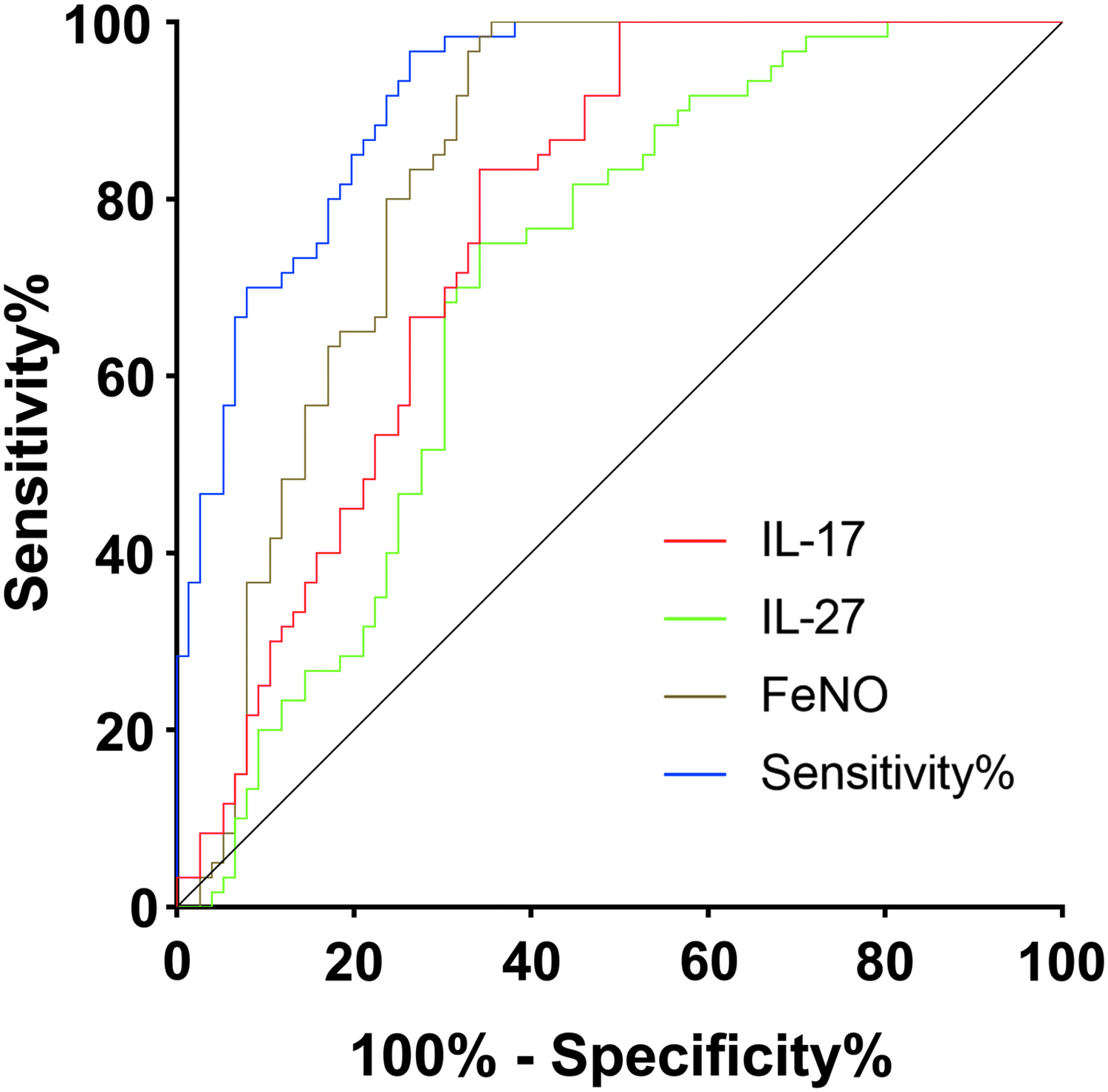
The effectiveness of IL-17, IL-27, and FeNO in the diagnosis of bronchial asthma in children. AUC(IL-17) = 0.772, AUC(IL-27) = 0.702, AUC(FeNO) = 0.838, AUC(Combination) = 0.917. AUC, area under the curve; IL-17, interleukin-17; IL-27, interleukin-27.
The Effectiveness of Interleukin-17, Interleukin-27, and Fractional Exhaled Nitric Oxide in the Diagnosis of Bronchial Asthma in Children
AUC, area under the curve; CI, confidence interval; FeNO, fractional exhaled nitric oxide.
Lung function indicators
The lung function indicators of tidal volume, inspiratory time, expiratory time, respiratory ratio, peak time, time to reach peak tidal expiratory flow/total expiratory time (TPTEF/TE), and volume to peak tidal expiratory flow/total expiratory volume (VPTEF/VE) of the children in the remission stage and control group were significantly higher compared to the acute stage, while the respiratory rate was significantly lower in the remission and control group compared to those in the acute stage (all p < 0.05). There was no significant difference in the lung function indicators of tidal volume, respiratory ratio, inspiratory time, expiratory time, and respiratory rate between the children in the remission stage and the control group (all p > 0.05), however, the peak time, TPTEF/TE, and VPTEF/VE were significantly lower in the remission stage compared with those in the control group (all p < 0.05) (Table 4).
Lung Function Indicators
Compared with the acute stage, ap < 0.05.
Compared with the ressimion stage, bp < 0.05.
TPTEF/TE, time to reach peak tidal expiratory flow/total expiratory time; VPTEF/VE, volume to peak tidal expiratory flow/total expiratory volume.
Correlation of IL-17, IL-27, and FeNO with lung function
Pearson's correlation analysis showed that IL-17 positively correlated with the respiratory rate (p < 0.05) and negatively correlated with inspiratory time, expiratory time, respiratory ratio, peak time, TPTEF/TE, and VPTEF/VE (all p < 0.05). There was no correlation of IL-17 with tidal volume (p > 0.05). IL-27 positively correlated with the respiratory rate (p < 0.05) and negatively correlated with inspiratory time, expiratory time, peak time, and TPTEF/TE (all p < 0.05) while there was no correlation of IL-27 with tidal volume, respiratory rate, and VPTEF/VE (all p > 0.05). FeNO was also found to be positively correlated with the respiratory rate (p < 0.05) and negatively correlated with tidal volume, inspiratory time, expiratory time, respiratory ratio, peak time, TPTEF/TE, and VPTEF/VE (all p < 0.05) (Fig. 3).
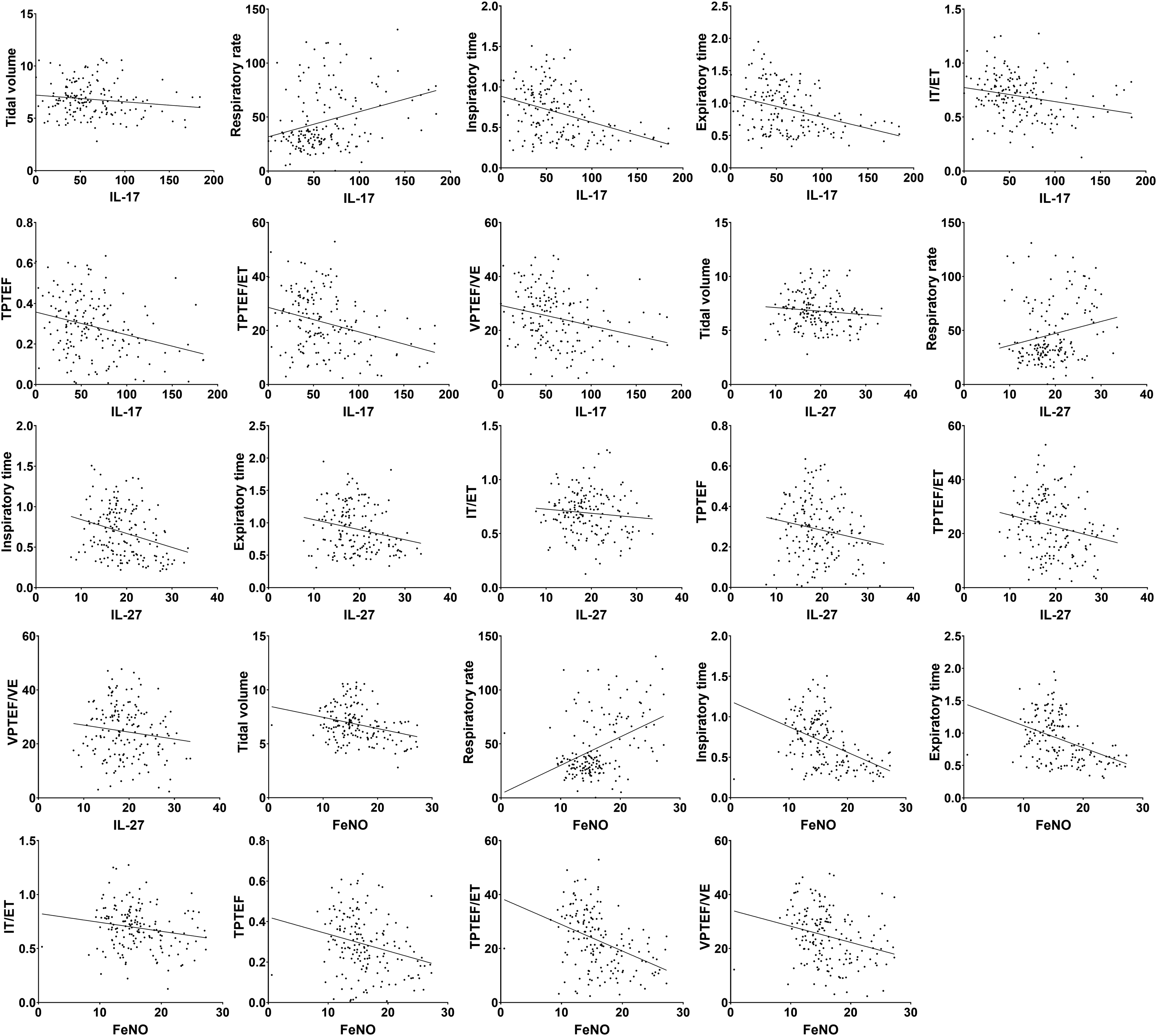
Correlation of IL-17, IL-27, and FeNO with lung function.
Discussion
Bronchial asthma is one of the most common respiratory diseases in pediatrics. Its main clinical characteristics include airway inflammation, reversible airway obstruction, airway hyperresponsiveness, and airway remodeling. In most countries, the prevalence of asthma is continuously increasing leading to an enormous social impact and increased cost to the public health care system (Braman, 2006; Liu et al., 2012). The current methods used to diagnose bronchial asthma in children are eosinophil count, lung function test, airway reversibility test, airway hyperresponsiveness test, and measurement of FeNO levels (Inoue et al., 2016; Lemière et al., 2018). However, these methods have some limitations such as complicated protocols and low specificity. Therefore, a simple, reliable, and minimally invasive biomarker is needed.
IL-17 is mainly secreted by CD4+ T helper cells and acts on Th17 cells. Many studies have reported that IL-17 is associated with asthma severity and airway remodeling (Nanzer et al., 2013). There is a link between the activation of the complement pathway and the IL-23-Th17 axis in severe asthma. Complement factor C5a inhibits IL-17-producing Th17 cells and affects the frequency of airway hyperresponsiveness, while complement factor C3a plays a stimulating role. The disruption of this equilibrium is conducive to the C3a pathway, thereby increasing the response of Th17 cells and airway hyperresponsiveness, which subsequently promotes IL-17 production (Chesne et al., 2014). IL-17 also promotes airway fibrosis by increasing the production of pro-fibrotic cytokines, pro-angiogenic factors, and collagen while it also promotes airway remodeling in synergism with Th17 cells in a CD40 signal-dependent manner (Molet et al., 2001; Hayashi et al., 2013). IL-27 is mainly produced by activated dendritic cells and lung macrophages and acts on helper T cells, regulating their differentiation and growth (Owaki et al., 2005). The exact mechanism of IL-27 in bronchial asthma is unclear. Allergen stimulation leads to an inflammatory reaction in the body that subsequently leads to an increase in the expression of IL-27, thereby inducing the expression of CXCL9 and CXCL10 and thereby, aggravating the inflammation of the airway. This may be one of the mechanisms through which IL-27 is involved in bronchial asthma (Nieminen et al., 2010; Dong et al., 2013). FeNO is a good indicator for evaluating allergic rhinitis and bronchial asthma, and it can effectively assess airway inflammation in patients (Giudice et al., 2016). The results in the present study show that the expression levels of IL-17 and IL-27 in the peripheral blood of children with acute bronchial asthma are significantly elevated, while the expression levels of IL-17 and IL-27 are decreased in children in remission. FeNO also showed the same trend, suggesting that IL-17 and IL-27 are closely related to the incidence and development of bronchial asthma in children.
The sensitivity and specificity of FeNO to diagnose bronchial asthma in children were found to be 98.45% and 64.47%, respectively. FeNO in combination with IL-17 and IL-27, the diagnostic specificity for bronchial asthma in children increased to 83.68%, which increased the diagnostic efficacy of FeNO. It may provide a reference for clinical screening of bronchial asthma in children. Mansour et al. reported that the cutoff of IL-17 for the diagnosis of pediatric asthma was 13.1 pg/mL while its sensitivity and specificity was 83.3% and 70%, respectively. The sensitivity can be increased to 95% when combined with IL-35 for diagnosis (Mansour et al., 2017). The possible reason for this could be the differences in recruited subjects. All subjects in the study of Mansour et al. were children with bronchial asthma while we have analyzed children with acute bronchial asthma. Du et al. (2016) reported that IL-17 rs763780, rs2275913, and rs8193036 single nucleotide polymorphisms may be associated with asthma susceptibility in Asian populations, while GA genotype in rs2275913 and TT genotype in rs8193036 of IL-17 may lead to an increased risk of asthma in Asians. Few diagnostic studies have been reported on IL-27 levels and asthma. In a study by Jacobs et al. (2018), IL-27 was identified as a potential biomarker for bacterial infection in immunocompromised pediatric patients. Abo-ElMagd et al. (2018) reported that the sensitivity of IL-27 for diagnosis of neonatal bacterial sepsis was 95.56%, specificity was 100%, and cutoff value was 485.56. Zhang et al. (2018) reported the importance of the diagnostic value of IL-27 in tuberculous pleural effusion. These studies suggest an important role of IL-27 in neonatal lung disease. Therefore, IL-17 and IL-27 may be important biomarkers in the diagnosis of bronchial asthma in children. However, considering the complexity, bronchial asthma can be divided into T2 type high asthma and T2 type low asthma. The main difference between the two is that T2 type low asthma has corticosteroid resistance, which is rare. The treatment and diagnostic criteria for asthma are not fully applicable to T2 low asthma (Amelia et al., 2018). Therefore, the clinical significance of IL-17 and IL-27 expression in the two subtypes of bronchial asthma needs further analysis.
Lung function is an important indicator of airway function (Ierodiakonou et al., 2016). In the present study, we have analyzed the correlation between IL-17, IL-27 levels, and lung function indicators in children with bronchial asthma. The study showed that IL-17 and IL-27 levels correlated with the extent of lung function damage. FeNO levels also correlated with lung function damage in children. The relationship between FeNO and lung function had been previously verified in many studies (Arakawa et al., 2016; Mansur et al., 2018). In addition to FeNO, we have also shown that IL-17 and IL-27 could be useful in the assessment of lung function.
However, the present study has some shortcomings. In this prospective study, there may have been some bias in the process of subject recruitment while there could also have been an inevitable Hawthorne effect, that is, when people realize that they are being investigated or observed, they deliberately change some behaviors or verbal expressions. The results and conclusions in this study still need to be further verified. In addition, we have analyzed the differences in IL-17 and IL-27 levels between two groups of children in the acute stage and in the remission stage but did not study the changes in IL-17 and IL-27 levels in children that improved from the acute stage to remission. This aspect could be explored in future studies. In addition, whether IL-17 and IL-27 can be used as potential indicators for the treatment of bronchial asthma remains to be further studied.
In conclusion, IL-17 and IL-27 are closely related to the occurrence and development of bronchial asthma in children and may have a good diagnostic value for bronchial asthma in children. It can effectively improve the specificity of FeNO in diagnosis and can reflect, to a certain extent, the extent of lung function damage.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.