
Abstract
Background:
Multiple lines of evidence have suggested that genetic factors may contribute to steroid-induced osteonecrosis of the femoral head (SONFH). Complement receptor 2 (CR2), constituting a family of regulators of complement activation, has been recently reported to be associated with osteonecrosis of the femoral head (ONFH) in Koreans. The aim of this study was to evaluate the relationships between polymorphisms of the CR2 gene and susceptibility to SONFH in the male Han Chinese population.
Materials and Methods:
A total of 468 SONFH patients and 1224 healthy controls were recruited for this study. Ten tag single nucleotide polymorphisms (SNPs) located within the CR2 gene were genotyped. Genetic association analyses, including SNP and haplotypic analyses, were performed for the 10 SNPs. Furthermore, bioinformatic analyses were conducted to examine the functional consequences of SNPs shown to be significantly associated with SONFH.
Results
: An intronic SNP, rs311306, was identified to be significantly associated with the risk of SONFH (p = 0.0008, odds ratio = 1.44). Allelic analyses showed that the C allele of this SNP significantly elevated the risk of SONFH, which was replicated in genotypic association analyses. Moreover, a 3-SNP haplotype was significantly associated with SONFH (rs311306-rs17044576-rs3767933, p = 7.49 × 10−8). Furthermore, bioinformatic analyses indicated limited functional consequences of SNP rs311306, but a complex interaction network was constructed for the protein encoded by the SLC44A2 gene and proteins encoded by the CD19, CD81, and C3 genes.
Conclusion:
Our findings shed new light on the link between the CR2 gene and SONFH in Han Chinese males, providing clues as to the nature of the mechanisms involved in the etiology of ONFH.
Introduction
Osteonecrosis of the femoral head (ONFH) is a kind of orthopedic refractory disease that occurs in middle-aged and young populations, resulting in substantial loss of function and disability. Its incidence rate rises every year, and 10,000-20,000 new cases are diagnosed in the United States each year (Mankin, 1992). ONFH is mainly divided into two categories: traumatic and nontraumatic. Because the onset of nontraumatic ONFH is insidious, the diagnosis of this disease is usually delayed, rendering treatment difficult (Ikeuchi et al., 2015). So far, long-term and large-scale use of glucocorticoids (GCs) has become the primary cause of nontraumatic ONFH (Varoga et al., 2009). However, only a portion of people who were exposed to the same dose of steroid will develop ONFH, suggesting that genetic factors may contribute to steroid-induced osteonecrosis of the femoral head (SONFH) (Wang et al., 2018).
Many case-control studies have also found a significant association between single nucleotide polymorphisms (SNPs) and SONFH in Caucasian and Chinese populations (Du et al., 2016; Wang et al., 2016). Hence, it is necessary to find the genes responsible for susceptibility to SONFH through candidate gene studies, which may lead to a better understanding of SONFH.
Complement receptor 2 (CR2), also known as CD21, belongs to the family of regulators of complement activation (Isnardi et al., 2010). Recently, in a Korean population, including 50 ONFH in systemic lupus erythematosus (SLE) patients (ONFH-SLE) and 150 SLE patient controls, SNPs, rs3813946, rs311306, and rs17615, were found to be significantly associated with an increased risk of ONFH-SLE under a recessive model (Kim et al., 2016). To date, this is the only study reporting the association between CR2 and SLE-induced ONFH. Considering that the current treatment for SLE could entail a large number of GCs, which is also an important risk factor for SONFH, CR2 may also be a susceptibility gene to SONFH.
Until now, the association of the CR2 gene with SONFH was only identified in samples from the Korean population and has never been validated in different populations. Given that different ethnic populations may exhibit genetic heterogeneity of SONFH, it is necessary to evaluate the association of the CR2 gene and SONFH in other ethnic populations to improve the current understanding of the role of the CR2 gene in SONFH risk. Considering that the role of the CR2 gene in ONFH susceptibility in the Han Chinese population has not been previously evaluated, we carried out a case-control study to systematically investigate the relationship between genetic polymorphisms of the CR2 gene and SONFH risk in Han Chinese individuals, with the aim of providing clues as to the nature of the mechanisms involved in the etiology of SONFH.
Materials and Methods
Study subjects
In this study, we recruited 468 SONFH cases and 1,224 healthy controls consecutively from the Honghui Hospital of Xi'an Jiaotong University during the period 2013 to 2016. The diagnosis of ONFH was based on results of 3 examinations, including X-ray, bone scans, and magnetic resonance imaging. If the patient has used an average daily dose of ≥16.6 mg or a maximum daily dose of 80 mg prednisolone equivalent within 1 year before the onset of clinical symptoms or imaging diagnosis of ONFH (Koo et al., 2002), SONFH was diagnosed.
ONFH patients with a history of direct trauma or combined causes and other hip diseases, patients who consumed more than 400 mL of alcohol per week, and patients with a history of severe disease or severe chronic disease, such as diabetes, cardiovascular and cerebrovascular diseases, acute lymphoblastic leukemia, disseminated intravascular coagulation, hemoglobinopathies, hemophilia, diabetes, dysfunctional lipid metabolism, gout, coagulopathies, rheumatologic diseases and malignancies, sickle cell anemia, thalassemia, thrombophilias, HIV, pancreatitis, and osteomyelitis, were excluded from the study (Matos et al., 2012).
Healthy individuals who have never been exposed to high-dose steroids were enrolled as controls. They were recruited from individuals who participated in the routine physical examination and were matched by age and body-mass index (BMI) with the patients. All controls had no hip pain, no history of thromboembolic events, no symptoms of hip disease, and no chronic diseases or malignant diseases such as diabetes, cardiovascular and cerebrovascular diseases, and cancers. X-ray results in the anterior and posterior pelvis showed no lesions. All subjects were Han Chinese males living in Xi'an city and surrounding areas. Written informed consent was given by all subjects. The study protocol was approved by the Ethics Committee of the Honghui Hospital of Xi'an Jiaotong University.
SNP selection and genotyping
All SNPs in the CR2 gene with minor allele frequencies (MAFs) >0.05 based on the 1000 Genomes Project Han Chinese in Beijing (CHB) population were searched first. Then, MAFs >0.05 with pair-wise tagging and r2 ≥0.6 were defined as selection criteria to generate 10 tag SNPs for our study. Basic information on the 10 tag SNPs is presented in Supplementary Table S1.
Genomic DNA was extracted from peripheral blood using Tiangen DNA extraction kits (Tiangen Biotech Co., Ltd., Beijing, China) according to the manufacturer's protocol. The Sequenom MassARRAY platform with iPLEX GOLD chemistry (Sequenom, San Diego, CA, USA) was utilized for SNP genotyping through the manufacturer's protocols. Sequenom Typer 4.0 software was used for processing raw signals and generating genotype data (Guan et al., 2012). Laboratory personnel were blinded to the case-control status of the samples (Guan et al., 2014). Five percent of the samples were replicated in genotyping, and the results were 100% in concordance with the other results.
Statistical analysis
Differences in characteristic information between patients and controls were examined by the χ2 test and Student's t-test. Hardy-Weinberg equilibrium tests were performed for each genotyped SNP in the control group by Haploview. Single SNP-based association analyses were performed using PLINK (Chang et al., 2015). Odds ratios (ORs) and 95% confidence intervals (CI) were calculated as well. Linkage disequilibrium (LD) blocks were also constructed by Haploview, and haplotypic association analyses were performed for each LD block using PLINK. Bonferroni corrections were applied to avoid multiple comparisons, and the threshold of the p value used for single SNP association analyses was 0.05/10 = 0.005.
To further investigate functional consequences of the significant hit in the association analyses, we utilized RegulomeDB and extracted expression quantitative trait locus (eQTL) data from the GTEx database (Consortium, 2013) to examine the biological function of the associated SNP. CR2 expression data in multiple human tissues were extracted, and eQTL signals were analyzed. In addition, we investigated the gene-gene network of CR2 using the STRING database, which is a database of known and predicted protein-protein interactions.
Results
All participants were male, comprising 468 SONFH cases and 1224 healthy controls. As shown in Table 1, no significant differences were identified for age, BMI, smoking status, or drinking status between SONFH cases and controls (Table 1). All SNPs were in Hardy-Weinberg equilibrium in the control group (p > 0.05; Supplementary Table S1). As presented in Table 2, an intronic SNP, rs311306, was identified to be significantly associated with the risk of SONFH (χ2 = 11.18, p = 0.0008). The association signal was still significant after Bonferroni correction (pthreshold = 0.05/10).
Demographic and Characteristic Information of the Study Subjects
Results of Single-Marker-Based Association Analyses
Significant hit is highlighted in bold.
A1, tested allele (minor allele); BP, base pair on the chromosome; CHR, chromosome; CI, confidence interval; F_A, minor allele frequency in cases; F_U, minor allele frequency in controls; OR, odds ratio.
The MAF of the C allele of this SNP was significantly higher in SONFH cases compared with controls, and further analyses also indicated that the C allele of rs311306 has a positive correlation with the risk of SONFH (OR = 1.44, 95% CI = 1.16-1.79; Table 2). Further genotypic analyses identified the dose-dependent pattern. Compared with the GG and GC genotypes, the distribution of CC genotype was almost threefold higher in the patients (OR = 1.32, 95% CI = 1.03-1.70; Table 3). Similar results were obtained in both allelic and genotypic analyses.
Genotypic Association Results of rs311306
Significant p value is in bold italics.
OR and 95% CI were calculated in the additive model.
The LD structure of 10 SNPs is constructed in Figure 1. As presented in Figure 1, three LD blocks were identified, and the associated SNP rs311306 was located in block 1. Haplotypic association analyses were conducted in all LD blocks, and the results are summarized in Table 4. A 3-SNP haplotype was identified to be significantly associated with SONFH (rs311306-rs17044576-rs3767933, χ2 = 36.00, p = 7.49 × 10−8). The significant hit of single SNP-based association analysis was also included in this haplotype, which provided supportive evidence of the significant association of rs311306 with the risk of SONFH (Table 4). Furthermore, two common haplotypes in block 1 had solid associations with the risk of SONFH. For example, the frequency of haplotype CTC in the patients (p = 2.02 × 10−8; Table 4) increased threefold compared with controls, and the haplotype GTC had a higher frequency in the controls (p = 0.0081; Table 4).
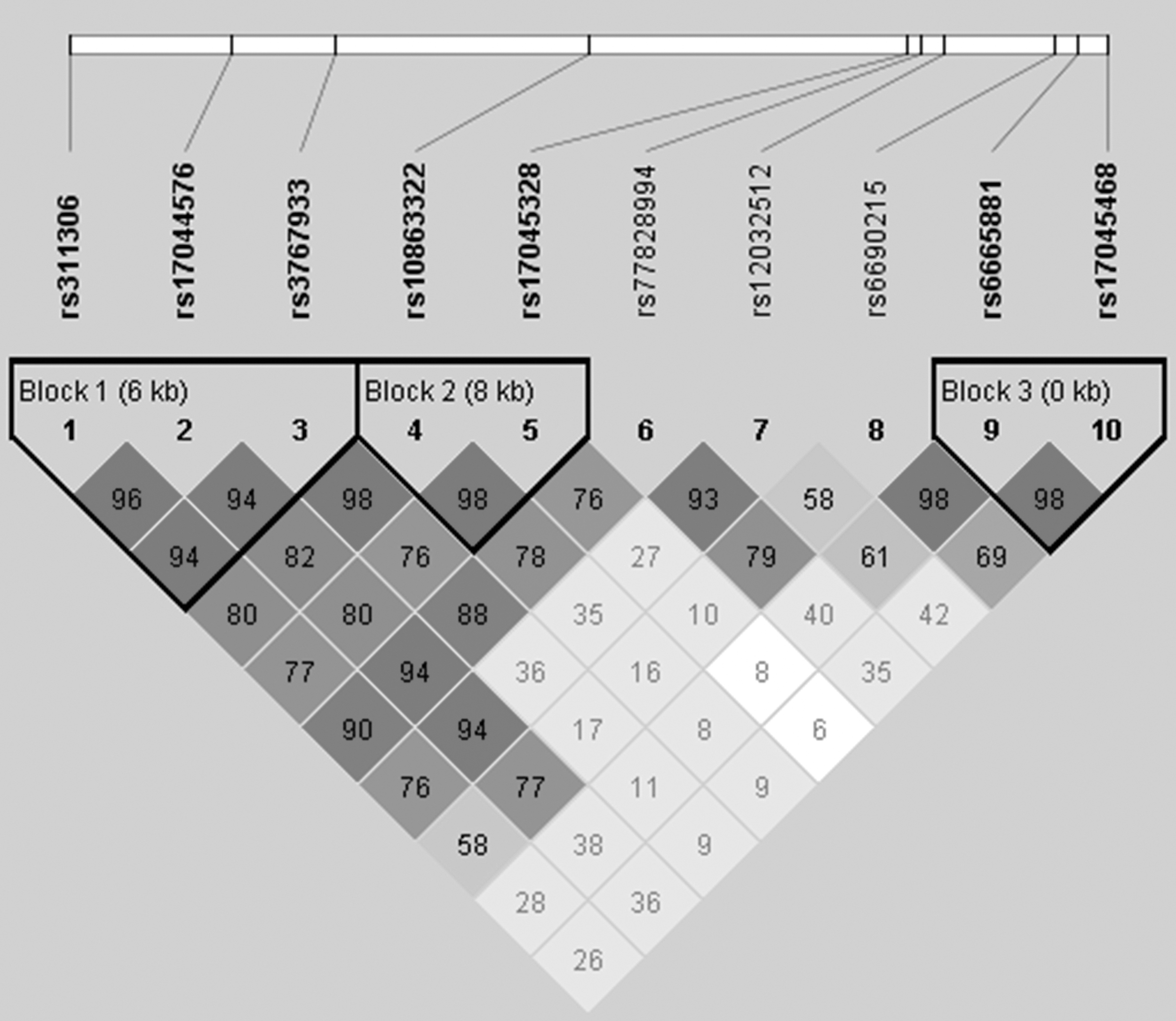
Linkage disequilibrium structure of the 10 tag SNPs. Values of D′ are indicated in each cell. The darker the gray color, the greater the value. Bold SNPs indicate that they are in the linkage disequilibrium blocks. SNP, single nucleotide polymorphism.
Results of Haplotype-Based Association Analyses
Significant hits are highlighted in bold.
DF, degree of freedom; F_A, haplotype frequency in cases; F_U, haplotype frequency in controls.
The potential biological function of SNP rs311306 was examined in the RegulomeDB database, and the RegulomeDB score was 5. The database has a self-developed score system ranging from 1 to 7; the lower the score, the more the functional significance. Thus, the function of the associated SNP is unknown. Furthermore, the eQTL data of SNP rs311306 on CR2 in 25 human tissues were extracted and analyzed (Fig. 2 and Supplementary Table S2).
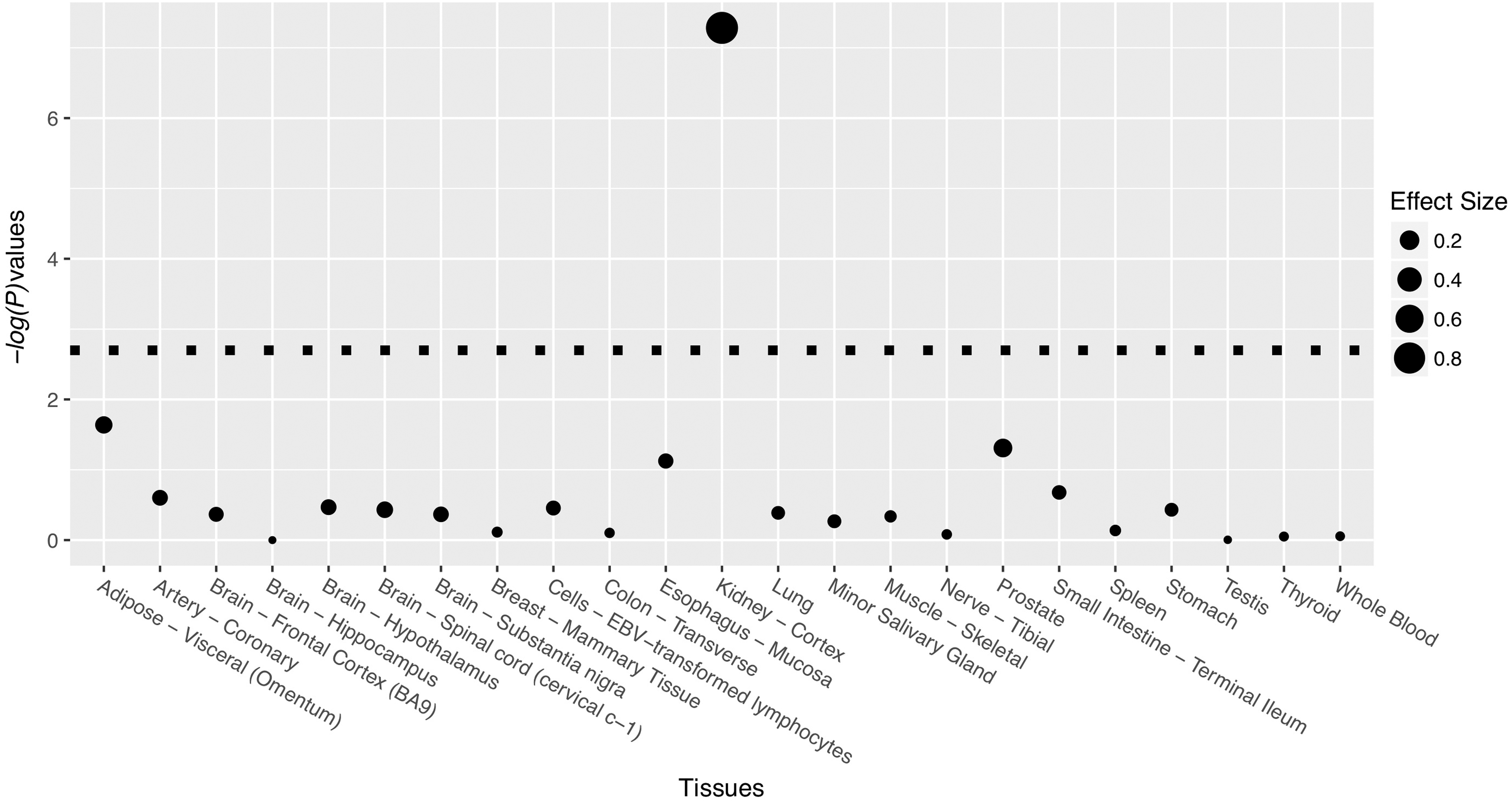
The eQTL signal of SNP rs311306 in multiple human tissues. The threshold of p values after Bonferroni correction is indicated by the dotted line. eQTL, expression quantitative trait locus.
After Bonferroni corrections, a significant eQTL hit was identified in the kidney cortex. The C allele of SNP rs311306 was significantly associated with a higher expression level of CR2 in the kidney cortex (Supplementary Fig. S1). These results indicated that the functional consequences of SNP rs311306 were very limited. The gene-gene network of CR2 is shown in Figure 3. According to the STRING database, the protein product of CR2 interacts experimentally with several proteins encoded by genes CD19, CD81, and C3. In addition, CR2 was also predicted to be connected with other proteins encoded by genes, including CD27, TNFSF13B, CD5, SPN, IFNA21, IFNA17, and IFNA2.

Gene-gene interaction network constructed based on protein-protein interaction (PPI) data. Lines mean experimentally determined interactions and predicted interactions.
Discussion
Previous studies have suggested that some variants may be involved in development of ONFH, but the genetic association between these variants and susceptibility to SONFH remains unknown. Recently, Kim et al. reported that three SNPs (rs3813946, rs311306, and rs17615 in the CR2 gene) were associated with an increased risk of ONFH (Kim et al., 2016), but the association between genetic variants in the CR2 gene and SONFH has not been examined. In this study, an intronic SNP rs311306 in the CR2 gene was identified to be significantly associated with the risk of SONFH both at allelic and genotypic levels in Han Chinese individuals. Notably, in Kim's study, only the association signal of SNP rs311306 was still significant after Bonferroni correction.
Moreover, based on the 1000-genome CHB data, we found that there was a strong LD between rs3813946 and rs311306 (r2 = 0.95) or between rs17615 and rs311306 (r2 = 1). Still, both studies also indicated a slight difference in MAF at rs311306 between the Han Chinese population and Koreans, suggesting that the SNP may have a certain degree of population heterogeneity. Furthermore, haplotype analyses were conducted in our study and also presented a significant association signal between rs311306 and the risk of SONFH, providing further evidence for our results. Although our study has different patterns from those reported by Kim et al., both studies established the link between the CR2 gene and ONFH. To the best of our knowledge, our study was the first to report the association between the CR2 gene and SONFH in the Han Chinese population. Further studies are still needed to validate the current findings in other different populations.
The product of CR2 functions as a receptor for C3d/iC3b, which plays an important role in innate immunity and induction of inflammatory signaling pathways (Sarrias et al., 2001). Several studies have indicated that inflammation plays an important role during development of SONFH (Jin et al., 2019). Excess steroids can suppress complement activation and immune complex formation and ultimately lead to immune system malfunctions and SONFH (Luukkainen et al., 1992). Previous studies have shown that SONFH patients have a significantly lower level of complement factor C3 (C3) in serum (Chen et al., 2015). C3 has already been demonstrated to be closely related to arthritis (Monach et al., 2007). Knocking out C3 expression was able to reduce the severity of arthritis in mice (Hietala et al., 2004).
In addition, C3 may control the clearance of necrotic or apoptotic cells in tissue remodeling (Elward et al., 2005). It has been demonstrated that the increased apoptosis level in osteoblasts and osteocytes escalates the severity of ONFH in both mice and humans receiving GCs (Weinstein et al., 2000). These results suggest that the CR2 gene may be involved in the pathogenesis of SONFH by regulating the complement system, especially C3, which can regulate inflammation and apoptosis in SONFH. An increased risk of ONFH can also be influenced by some autoimmune disorders, including SLE and rheumatoid arthritis (Leventhal and Dorfman, 1974).
The significant hit, SNP rs311306, was an intronic SNP and therefore it cannot have any functional consequences of altering the protein encoded by CR2. In the recent years, a large number of risk variants of complex diseases have been identified, such as schizophrenia (Zhang et al., 2018; Han et al., 2019; Guan et al., 2020a). Given that it is difficult to obtain reliable results only from SNP-based analyses (Zhu et al., 2016; Sun et al., 2017; Zhang et al., 2017; Li et al., 2018; Guan et al., 2020b), related gene expression analyses would be necessary. Thus, further analysis based on data extracted from the GTEx database indicated that this SNP was a significant eQTL for CR2 in a specific type of human tissue.
However, we need to be careful in interpreting such results obtained from publicly available databases. First, the kidney cortex does not seem to be related to SONFH; therefore, this result could serve as indirect evidence of the functional consequences of SNP rs311306 in the risk of SONFH. Second, eQTL data in the GTEx database were obtained from individuals with various conditions and might not be a proper reference for SONFH. In addition, even if we can show that the SNP rs311306 has an eQTL effect on CR2 in certain tissues in ONFH, it is still difficult to establish the functional link between this SNP and ONFH because we have not thoroughly examined the genetic architecture of CR2.
The SNP rs311306 might only serve as a surrogate of some underlying ungenotyped DNA variants with true effects on the risk of SONFH. In future studies, functional analysis is still needed to fully investigate the functional consequences of SNP rs311306 on CR2 in targeted tissues of SONFH. In the present study, we only examined common variants. However, several recent studies have indicated that rare and low-frequency variants might contribute significantly to the risk of complex human disorders (Sule et al., 2013; Umair et al., 2017; Di Resta et al., 2018). Thus, target sequencing-based population studies might be informative in exploring the genetic architecture of CR2 in its association with SONFH.
The present study suffered from several limitations. First, we only recruited male subjects. This strategy accelerated the recruitment process at the cost of generalizing the study results. Another limitation is that we did not perform any statistical procedure to control population stratification, which might cause spurious association signals. As a candidate, gene-based association study, we simply do not have enough SNP data to perform statistical procedures commonly used in genome-wide association studies. Nevertheless, we restricted our study subjects to the Han Chinese population, who lived in Xi'an city and surrounding areas. This strategy was used to reduce the genetic heterogeneity of our study subjects and at least partly control the potential confounding effects.
Another potential concern is that all patients with ONFH had some underlying diseases, including rapidly progressive glomerulonephritis, primary nephrotic syndrome, pemphigus, and impetigo. Although no evidence has shown that these diseases are related to ONFH, it is still possible that ONFH was not caused by steroid therapy, but by these underlying diseases. In the present study, we have recruited individuals who have never been exposed to high-dose steroids as controls. This strategy might undermine the ability of the case-control study design to detect potential effective SNPs. A potential improvement is to enroll those individuals who have been exposed to high-dose steroids, but not developed ONFH. In addition, our study sample is a consecutive sample, but not a random sample of patients. Therefore, our results should be considered preliminary and need to be confirmed in the future research.
In summary, in this study, we identified an SNP within the CR2 gene that was significantly associated with the risk of SONFH. Our findings establish a link between the CR2 gene and SONFH in Han Chinese males, providing clues as to the nature of the mechanisms involved in the etiology of ONFH. Further exploration of the underlying biological mechanisms behind the significant signals identified in this study is a direction of interest for future research.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.