
Abstract
Background:
Multiple studies have explored the prognostic role and clinical significance of the expression of the programmed cell death-1 (PD-1) gene in hepatocellular carcinoma (HCC). However, the results have been inconsistent. This study evaluated PD-1 expression and its clinical significance in patients with HCC, as well as the correlation between HCC pathological features and prognoses.
Methods:
All related research in PubMed, Embase, and Web of Science prior to October 31, 2019, was retrieved. The Newcastle-Ottawa Scale was used to evaluate the quality of the literature. Stata 14.0 statistical software was used to analyze the data, and the correlations between PD-1 expression and the clinicopathological characteristics of patients were analyzed using the odds ratio (OR) and its 95% confidence interval (CI). The hazard ratio (HR) and its 95% CI were used to analyze the correlation between PD-1 high expression and patient prognosis. Begg's test was used to evaluate publication bias.
Results:
A total of 581 patients were analyzed in the six studies included in the meta-analysis. Pooled analysis revealed that high levels of PD-1 expression did not correlate with overall survival (HR = 0.79; 95% CI: [0.41-1.54]; p = 0.493). PD-1 positivity was associated with better disease-free survival (HR = 0.52; 95% CI: [0.38-0.72]; p < 0.0001). Furthermore, elevated PD-1 expression corrected for age (OR = 0.62, 95% CI: [0.41-0.96]; p = 0.030) and alpha-fetoprotein levels (OR = 2.27, 95% CI: [1.46-3.55]; p < 0.0001), were not correlated with patient sex, tumor size, tumor multiplicity, hepatitis B virus history, tumor node metastasis stage or Barcelona Clinic Liver Cancer stage.
Conclusions:
This meta-analysis revealed that PD-1 expression may be a useful prognostic marker in HCC patients. Prospective clinical studies are needed to support these findings.
Background
Hepatocellular carcinoma (HCC) remains one of the most common cancers worldwide. It is the fifth most common cancer and the second leading cause of cancer-related deaths (Torre et al., 2015). Although medical treatment has made great progress in the past decade, considering that liver cancer surgical resection is only applicable to a small number of patients and that the tumor recurrence rate is high after surgery, the long-term survival rate of liver cancer is low. Limited treatment options and high recurrence rates pose an imminent need for the discovery of new therapeutic interventions (Knox et al., 2015). Recent breakthroughs in cancer immunotherapy have revolutionized the method of cancer treatment, including HCC, in the era of precision medicine (Chen et al., 2016; Liu et al., 2019a, 2019b; Macek Jilkova et al., 2019).
Immune escape is an important mechanism of tumorigenesis and development. Its mechanism can be divided into the escape mechanism derived from tumor cells themselves and the escape mechanism derived from immune cells in the tumor microenvironment. T cells play an important role in immune escape (Hamid and Carvajal, 2013; Jiang et al., 2019; Tian et al., 2019). Increasing numbers of scholars have used immune checkpoints to explain the immune escape of tumors. Programmed cell death-1 (PD-1) is a 288 amino acid-sized cell membrane surface molecule encoded by the human PDCD1 gene, and its role is to negatively regulate the immune response (Henick et al., 2014; Sunshine and Taube, 2015). PD-1 ligands include programmed death-ligand 1 (PD-L1) and programmed death-ligand 2 (PD-L2). PD-L1 is a 40 kDa transmembrane protein encoded by the human CD274 gene. Its function in tumor tissues, pregnancy, allogenic graft tissue, and autoimmune diseases is to suppress immune system function (Ohaegbulam et al., 2015; Kim and Chen, 2016). When stimulated by T cell receptor signals or cytokines, PD-1 expression can be detected on the surface of T cells during the development of the thymus or on the surface of some peripheral hematopoietic cells. PD-1 is expressed on CD4− CD8− cells and on the surface of thymus cells. Its expression can also be induced on the surface of peripheral CD4+ T cells and CD8+ T cells, B cells, monocytes, natural killer cells, and some dendritic cells (Seifert et al., 2017; Zhao et al., 2019).
In many human cancers, PD-1 expression is linked to poor prognosis (Boger et al., 2016; Boussiotis, 2016; Reddy et al., 2017; Yang et al., 2017). PD-1 is also expressed in HCC. However, the impact of PD-1 expression on prognosis in HCC remains controversial due to limited data. Yang et al. (2019) reported that PD-1 expression was associated with poor overall survival (OS) in HCC. However, PD-1 expression was not correlated with OS according to Long et al. (2018).
To resolve the above inconsistency, based on the existing literature, we performed a meta-analysis to evaluate the relationship between PD-1 expression and the clinicopathological characteristics and prognosis of HCC.
Materials and Methods
This meta-analysis was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses declaration standards (Moher et al., 2009).
Search strategy
All related original research literature in PubMed, Embase, and Web of Science were retrieved with the search terms “programmed cell death protein 1”, “PD-1”, “Hepatocellular carcinoma”, and “HCC” up to October 31, 2019. In the search process, a combination of subject words and free words was used. In addition, the search was supplemented by manual search and other search methods, reference retrospection, and searches in Google Scholar.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) HCC was histopathologically diagnosed; (2) the expression of PD-1 was determined by immunohistochemistry or other methods; (3) cancer patients were divided into two groups based on the high and low expression levels of PD-1; (4) the relationship between PD-1 expression and prognosis or clinicopathological characteristics was described; and (5) hazard ratios (HRs) and 95% confidence intervals (CIs) were reported, or sufficient data were available for calculation. The exclusion criteria were as follows: (1) study type: review, conference summary, case report, etc.; (2) research object: animal experiment or cytology research; and (3) repeatedly published articles or repeated data applications.
Data extraction
Two authors (J.Y. and W.Z.) independently screened and extracted the literature according to the inclusion and exclusion criteria. Any cases of disagreement were discussed or judged by a third party (Y.Y.). For any studies lacking information, the original author was contacted. The extracted content included the following: title, author, year of publication, country, sample size, age, the detection method of PD-1, etc. In addition, clinicopathological parameters were also extracted from the eligible studies, including sex distribution, tumor size, tumor number, tumor node metastasis (TNM) staging, hepatitis B virus (HBV) history, and so on. If the HR was not directly provided in the text, it was calculated from the survival curve.
Quality evaluation
The Newcastle-Ottawa Scale (NOS) was used to evaluate the methodological quality of the included data for case-control studies. The NOS was mainly evaluated from three aspects: object selection, comparability between groups, and outcome measurement, with a maximum score of 9 points. Studies with a score >6 points were considered high-quality research.
Statistical analyses
Stata 14.0 software was applied to perform all statistical analyses. The 95% CI of the HR was used to evaluate the relationship between PD-1 expression and prognosis. If the HR was not provided in the article, then the method described by Parmar et al. (1998) was used. In the reported method, the HR is extracted from the Kaplan-Meier (KM) survival curve using Engauge Digitizer Version 4.1 software (http://digitizer.sourceforge.net/). For the evaluation of the relationship between PD-L1 expression and clinicopathological features, odds ratios (ORs) and 95% CIs were used. The method above was used for calculations. The heterogeneity test was performed by the χ2 test. p ≥ 0.1 and I2 ≤ 50% indicate that there is homogeneity between the results of the study, and a fixed effects model was used for meta-analysis; otherwise, a random effects model was used. The model was subjected to meta-analysis. Begg's test was used to estimate publication bias. Sensitivity analysis was used to assess the robustness of the combined results. p < 0.05 was considered statistically significant.
Results
Search results
A flow chart of the study selection criteria is shown in Figure 1. According to the above retrieval strategy, 286 articles related to PD-1 were retrieved from the major databases, and a total of 118 duplicate studies were removed by software. By reading the titles and abstracts, 152 articles that clearly did not meet the inclusion criteria were excluded. Then, according to the inclusion and exclusion criteria, a comprehensive and systematic evaluation was conducted on the remaining 12 articles with available full texts, and 6 articles were excluded. Six articles with 581 HCC patients were evaluated (Chang et al., 2017, 2018a, 2018b; Li et al., 2017; Long et al., 2018; Yang et al., 2019).
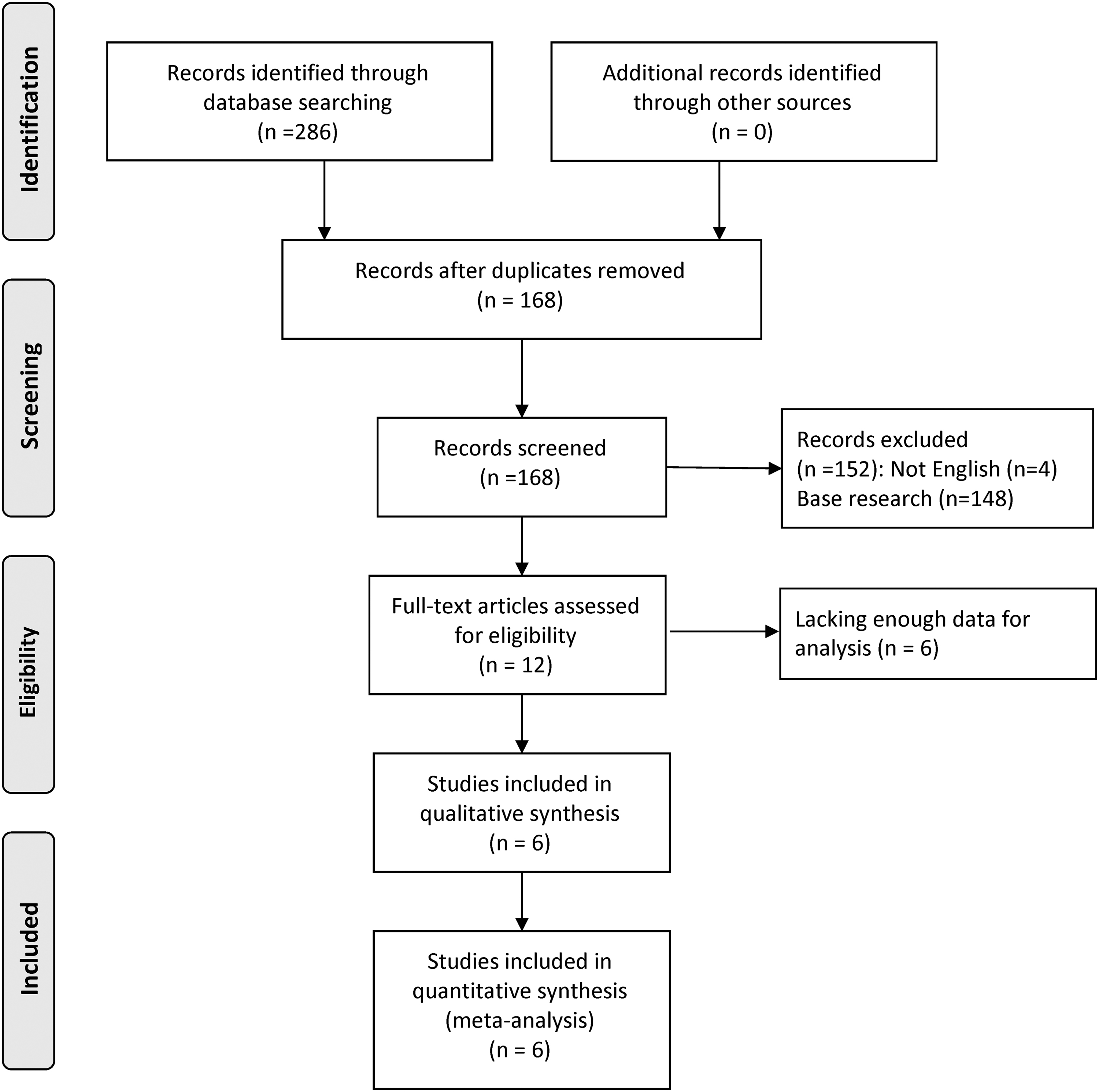
Flow chart of studies in the analysis.
Characteristics of the eligible studies
One study (Chang et al., 2018b) provided the HR and 95% CI for the reported OS and disease-free survival (DFS) directly; Kaplan-Meier curves were used to estimate the HRs and 95% CIs for the remaining studies (Chang et al., 2017, 2018a; Li et al., 2017; Long et al., 2018; Yang et al., 2019). The detection method used was an enzyme-linked immunosorbent assay in one study (Li et al., 2017), quantificational real-time polymerase chain reaction in one study (Yang et al., 2019), and the antibody array assay in one study (Chang et al., 2018a); the remaining studies used immunohistochemistry (Chang et al., 2017, 2018a, 2018b; Long et al., 2018; Yang et al., 2019). The number of cases included in the study ranged from 42 to 145. Five studies reported OS (Li et al., 2017; Chang et al., 2018a, 2018b; Long et al., 2018; Yang et al., 2019). Three studies reported DFS (Chang et al., 2017, 2018a, 2018b). The quality of the literature included in this study was high. The patient characteristics and study quality scores are listed in Tables 1 and 2.
The Characteristics of Studies Included in the Meta-Analysis
qRT-PCR, quantificational real-time polymerase chain reaction; ELISA, enzyme-linked immunosorbent assay; OS, overall survival; DFS, disease-free survival.
Quality Assessment Based on the Newcastle-Ottawa Scale
Survival analysis
Based on the six articles with OS/DFS data, we evaluated the correlation between PD-1 expression and prognosis among the 581 patients. The meta-analysis of five studies revealed no significant correlation between high/low expression of PD-1 and OS (HR = 0.79; 95% CI: [0.41-1.54]; p = 0.493). A high rate of heterogeneity was detected (I2 = 80.7%), and for this reason, a random effects model was used. For DFS, the results obtained from the analysis of three studies showed a low rate of heterogeneity (I2 = 48.2%), and a fixed effects model was used. HCC patients with high PD-1 expression levels had significantly better DFS than those with low PD-1 expression levels (HR = 0.52; 95% CI: [0.38-0.72]; p < 0.0001). The meta-analysis of PD-1 expression levels and prognosis of HCC patients are shown in Figures 2 and 3.
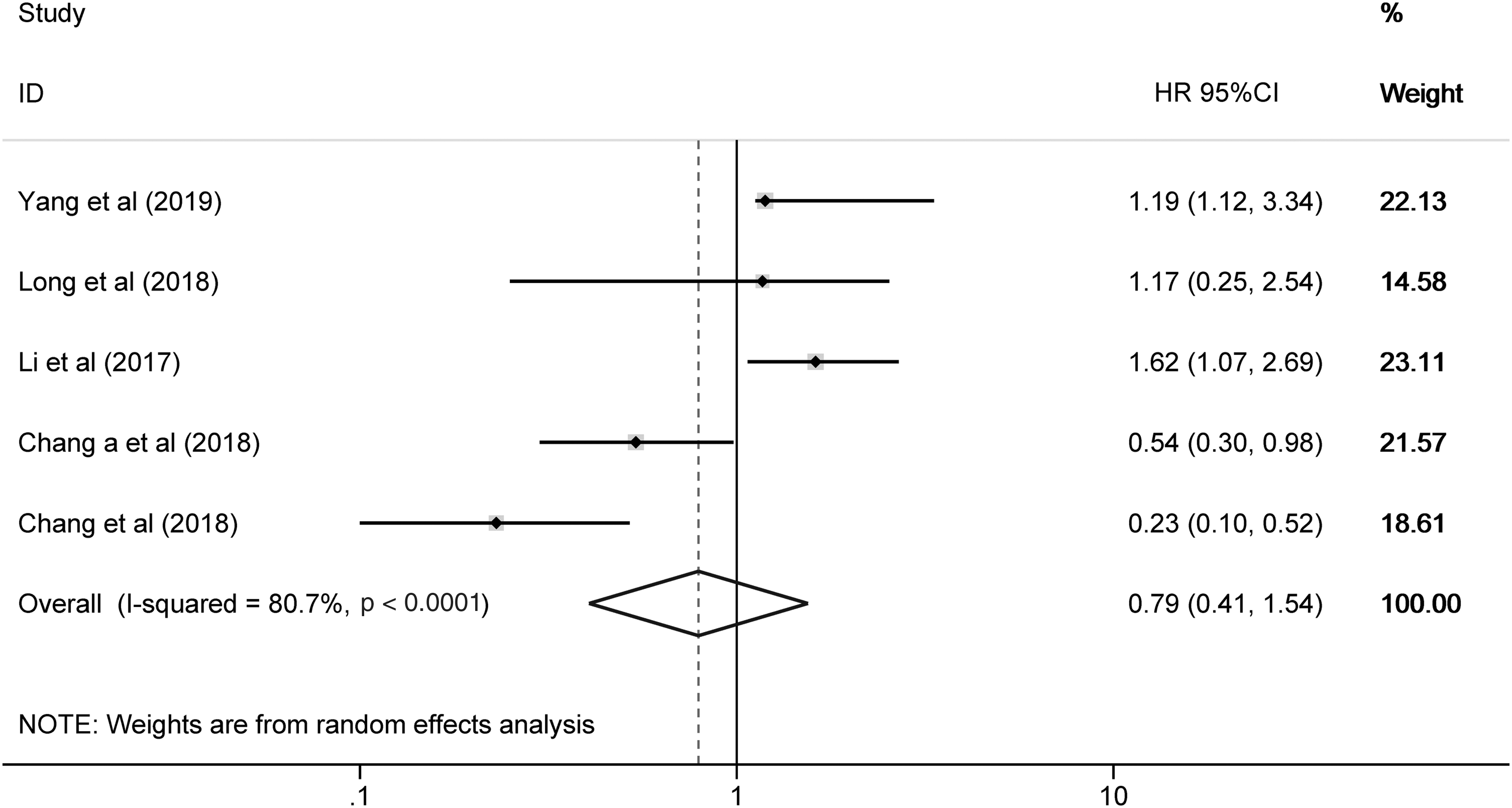
Forest plot of studies evaluating the association between PD-1 expression and OS in patients with HCC. HCC, hepatocellular carcinoma; PD-1, programmed cell death-1; OS, overall survival.

Forest plot of studies evaluating the association between PD-1 expression and disease-free survival in patients with HCC.
Correlation of PD-1 expression with clinical features
The correlations between PD-1 expression and age, sex, tumor size, alpha-fetoprotein (AFP), tumor multiplicity, HBV history, TNM stage, and Barcelona Clinic Liver Cancer (BCLC) stage showed less heterogeneity among the literature (I2 < 50%). The meta-analysis results showed that the correlations between PD-1 expression and sex, tumor size, tumor multiplicity, HBV history, TNM stage and BCLC stage (p > 0.05), age (OR = 0.62, 95% CI: [0.41-0.96]; p = 0.030), or AFP (OR = 2.27, 95% CI: [1.46-3.55]; p < 0.0001) were not statistically significant. The relationships between high PD-1 and the clinicopathological features are shown in Table 3.
The Relationship Between High Programmed Cell Death-1 and the Clinicopathological Features
HBV, hepatitis B virus; AFP, alpha-fetoprotein; BCLC, Barcelona Clinic Liver Cancer; TNM, tumor node metastasis; OR, odds ratio; CI, confidence interval.
Sensitivity analysis and publication bias
The sensitivity analysis is shown in Figure 4. After excluding Li et al. (2017), the meta-analysis results showed that the expression of PD-1 was still not significantly correlated with OS (HR = 0.64; 95% CI: [0.31-1.33]; p = 0.232). This suggested that the results of the study were unstable. In addition, the difference was not statistically significant. Therefore, whether the expression of PD-1 is related to OS needs to be further verified. In this meta-analysis, according to Begg's test (p = 0.142), there was no publication bias in the included literature involving PD-1 and OS (Fig. 5).
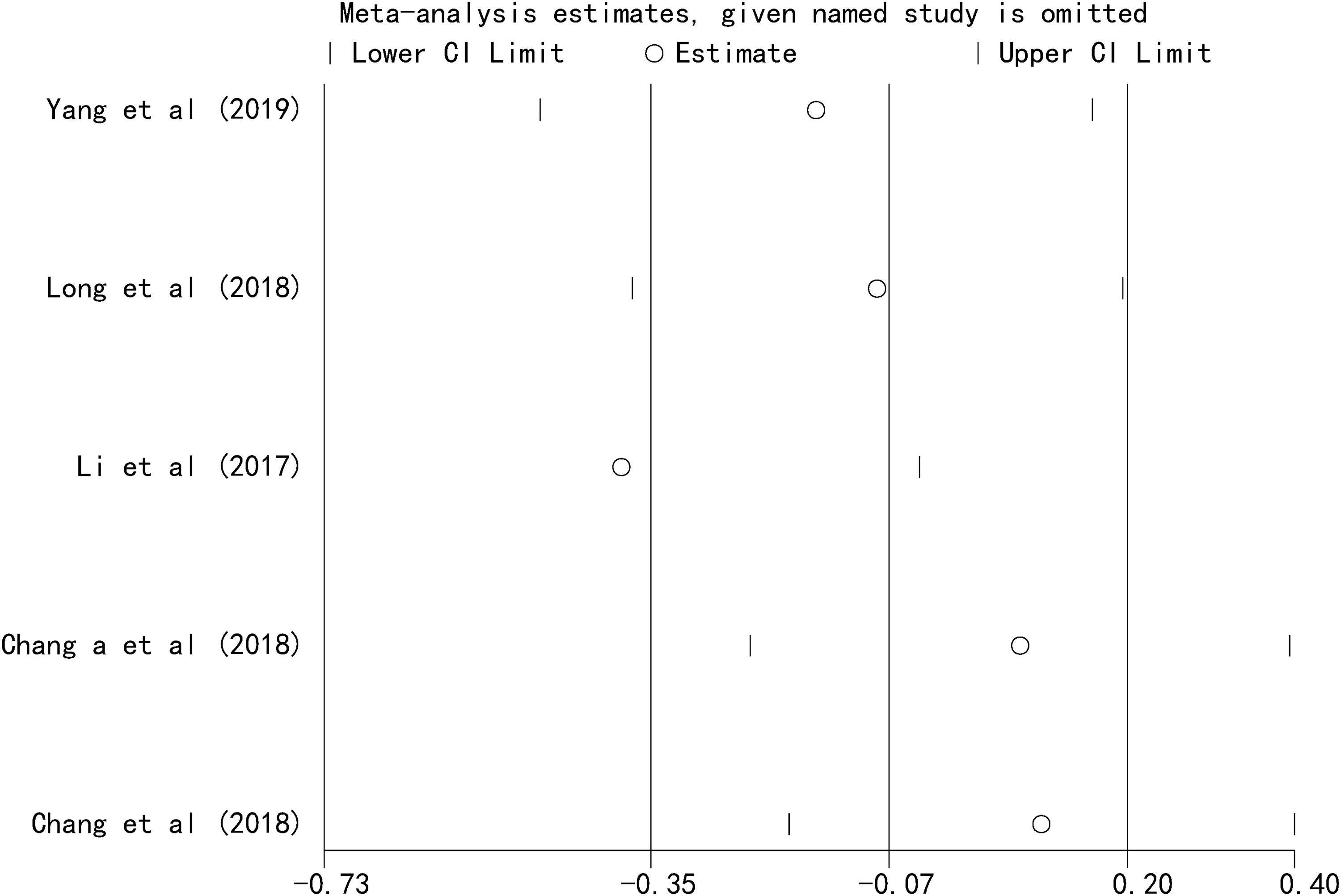
Sensitivity analysis for all eligible studies investigating the association between PD-1 expression and OS in patients with HCC.
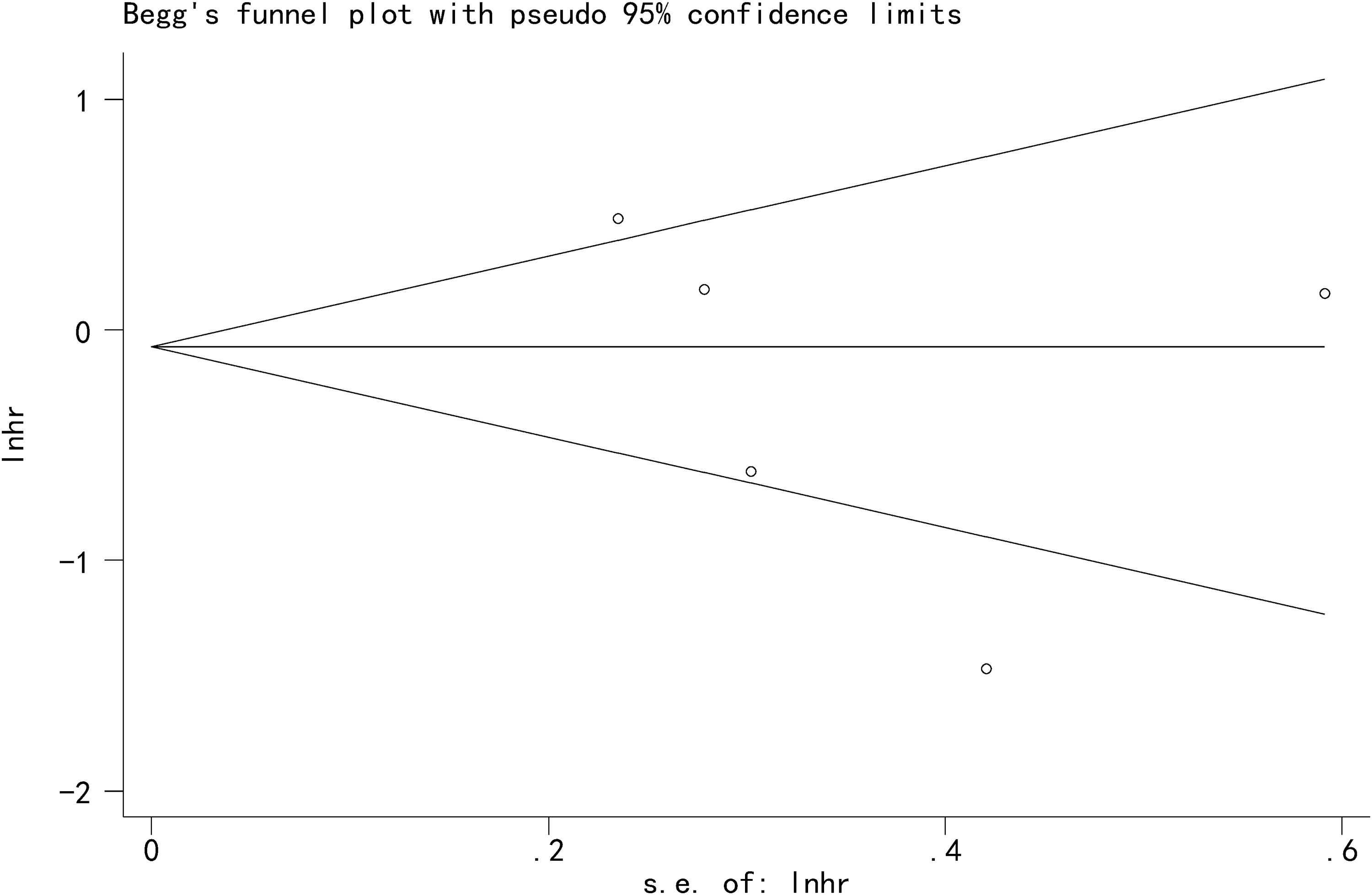
Begg's funnel plot for publication bias test, including PD-1 expression and prognosis in HCC.
Discussion
There is emerging evidence that immune escape and cancer immunoresistance play essential roles in tumor recurrence (Prieto et al., 2015). The most important antitumor immune response is mediated by T lymphocytes. T lymphocyte activation requires the stimulatory and inhibitory signals provided by the receptors and ligands of the CD28-B7 family (Chen, 2004; Inman et al., 2007; Tang et al., 2015). PD-1, a member of the CD28-B7 superfamily of costimulatory molecules, has been well characterized as a negative regulator of T cells by delivering inhibitory signals. It is expressed on activated CD4+ and CD8+ T cells and natural killer T cells (Keir et al., 2008). To date, two ligands have been identified for PD-1, namely, PD-L1 and PD-L2. PD-1/PD-L1 engagement blocks T cell receptor signaling, inhibits T cell proliferation, and contributes to T cell exhaustion, which is a crucial mechanism of immune evasion by tumors (Pardoll, 2012; Ceeraz et al., 2013; Zou et al., 2016). In many human cancers, PD-1 expression is associated with poor prognosis (Boger et al., 2016; Reddy et al., 2017; Yang et al., 2017). PD-1 is also expressed in HCC. However, many studies have found that it is not related to the prognosis of liver cancer patients (Chang et al., 2017; Li et al., 2017; Long et al., 2018). Moreover, whether PD-1 can be used as a molecular marker for the prognosis of liver cancer patients and whether its expression is closely related to the pathological characteristics of liver cancer are unknown.
This study conducted a meta-analysis on the above issues and found that high PD-1 expression was significantly associated with better DFS but was not related to OS in HCC. In the analysis of PD-1 and OS, the heterogeneity of the literature was found to be high. The reason for the possible heterogeneity is not clear; it may be due to inappropriate immunohistochemistry (IHC) staining conditions or because different groups use different treatment methods, and the threshold may lead to the bias observed in this meta-analysis. PD-1 as a prognostic factor for liver cancer also requires more high-quality prospective studies with uniform standards to provide more reliable evidence.
This study also assessed the relationship between PD-1 expression and the clinicopathological characteristics of HCC. All eligible studies showed that PD-1 expression is not related to sex, tumor size, tumor multiplicity, HBV history, TNM stage, or BCLC stage. The reasons for this finding may be related to the sample. The lack of quantity is also a related factor, and the significance of some indicators is not shown. However, the expression of PD-1 was significantly correlated with age and AFP. Due to the small number of studies included in this study, a large number of subsequent studies are needed to verify this hypothesis.
Our study has several limitations. First, the search strategy was used to obtain qualified English literature, and research reports published in other languages were not included. This may lead to potential bias and heterogeneity. Second, the cases included in this article were all case-control studies or cohort studies, so care should be taken in interpreting the combined results. Third, due to the different reagents used by each research group, the protein expression determination criteria differed, which unavoidably had a certain impact on the analysis results. Fourth, because many original documents only provided survival curves, the data extracted through indirect methods may have some impact on the final results. Fifth, all patients included were treated with surgery, but the treatment methods used before and after surgery were unclear, and the PD-1 expression site was also different, which had a certain impact on this meta-analysis. Thus, more prospective clinical studies are needed to further evaluate PD-1 expression in HCC, especially regarding OS, to explore its impact on prognosis.
Conclusions
The results indicated that PD-1 expression may be a useful prognostic marker in HCC patients. Due to the small number of studies included in this study, there are some limitations. To obtain more reliable conclusions, more forward-looking studies are needed in the future.
Footnotes
Ethical
Aggregate data were extracted from published studies; no patients were involved in the conduct of this study; thus, ethical approval and informed consent were not required.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.