
Abstract
Aim:
Spinal muscular atrophy (SMA) is an inherited, autosomal recessive neuromuscular disease that causes high morbidity and mortality. The prevalence is 1-2/100,000, while the incidence is 1/6000-1/10,000 among live births. Due to the high carrier frequency (1/40-1/60) of SMA-associated alleles, screening can prevent new cases. The aim of the current study was to present the development of a new, quantitative, real-time, polymerase chain reaction (PCR)-based screening test that uses an intelligent ratio (IR) for analyses, as well as a comparison of the results with the gold standard.
Materials and Methods:
Included in the study were 100 patients with various risk genotypes for survivor motor neuron 1 (SMN1) and SMN2 genes whose genetics had been previously investigated using multiplex ligation probe amplification (MLPA). A combination of the 5′ nuclease assay and allele-specific PCR was used to quantify the SMN1 deletion mutation with real-time PCR using the FII gene as a reference. All of the optimized standards were adapted to software that provided automated analyses. The approval number of the institutional ethics committee for the study is 2012-KAEK-15/1497.
Results:
The results of the screening test were completely compatible with the MLPA results; it achieved 100% sensitivity and specificity compared with the gold standard. The use of the IR in the analyses provided a user-independent method that quickly and accurately provided results, regardless of the amount of DNA used of the extraction method.
Conclusion:
Carrier or newborn screening of SMA is essential in countries that have high rates of consanguineous marriages. The screening test presented in this study that uses FII as a reference gene proved to be low-cost, reliable, applicable, accurate, and amenable to use in an automated system for SMA screening.
Introduction
Spinal muscular atrophy (SMA), one of the most common causes of infant death, refers to a group of inherited autosomal recessive neuromuscular diseases characterized by muscle weakness and atrophy. The phenotype is caused by progressive degeneration and loss of anterior horn cells in the spinal cord and nuclei of the brainstem (Verhaart et al., 2017). According to the age of onset and clinical severity of symptoms, four clinical subtypes have been defined and classified. About 50% of SMA patients are diagnosed with type 1 (Werdnig-Hoffman disease), which is not only the worst prognostically but is also the most common type (Markowitz et al., 2004). Type 2, the infantile-onset chronic form of SMA, and type 3, the juvenile-onset form, are the intermediate forms of the disease, which differ from each other by the ability to walk in type 3. Type 4 is the milder form of the disease with adult onset (Prior et al., 2010). The recently defined form of SMA is type 0 that presents with intrauterine-onset hypotonia and birth asphyxia and progresses to fatal outcomes in the neonatal period (Al Dakhoul, 2017).
The carrier frequency of SMA ranges between 1/40 and 1/60. Although it varies according to the rates of marriages with consanguinity or the genetic background of the population, the incidence of SMA is estimated to be ∼1 in 10,000 live births. Furthermore, the prevalence has been reported as 1-2 in 100,000 due to early mortality in patients with the disease (Markowitz et al., 2004; Prior et al., 2010; Verhaart et al., 2017).
The cause of all five types of 5q13.2-associated SMAs is the homozygous or compound heterozygous mutations of the survivor motor neuron 1 (SMN1-MIM *600354) gene. The molecular mechanism of clinical differences between SMA subtypes has been thought to depend on the number of copies of the SMN2 gene, which is known as the modifier of the disease (Lunn and Wang, 2008).
SMN2, which is the centromeric homolog of SMN1, is identical to SMN1, except for five single nucleotide variations, four of which are noncoding variants, and the only coding variation is c.840C>T, which is a silent transition mutation in exon 7 of the SMN2 gene. SMN2 dysregulates the exonic splicing enhancer and causes a less functional transcript. Deletion of both copies of exon 7 in the SMN1 gene, or SMN1 conversion to the SMN2 gene, is the most causative mechanism (95%) of the disease (Ogino and Wilson, 2004). Deletion of SMN1 on one allele and a single nucleotide mutation of the other allele have been reported as minor causative reasons (4%) of the disease. Additionally, single nucleotide mutation of both alleles is the rarest reason (Prior et al., 2010).
SMA causes high mortality and lifelong morbidity, so several methods have been developed for its prevention and/or treatment. Nusinersen is the first agent used in SMA treatment and is an antisense oligonucleotide that aims to increase the SMN protein expression. However, due to the requirement of early diagnosis, application difficulties, and high cost of treatment, it is not widely used. (Gidaro and Servais, 2019).
Thus far, various methods, such as multiplex ligation probe amplification (MLPA), restriction fragment length polymorphism (RFLP), real-time polymerase chain reaction (PCR), capillary electrophoresis, PCR-RFLP, and digital droplet PCR, have been used for the diagnosis and screening of SMA. Although MLPA has proven to be the gold standard method of diagnosis, it is not a relatively low-cost method and has user-dependent outcomes with a requirement of prolonged time for carrier screening (Prior et al., 2011).
In this study, it is aimed to develop an easily applicable, reliable, sensitive, user-friendly, cheap, and comprehensive screening test using the combination of amplification refractory mutation system analysis, 5′ nuclease assay, and allele-specific PCR technologies for quantification of deletion of the SMN1 mutation based on the single nucleotide variant in exon 7 with real-time PCR. This method will determine genotypes using a special ratio called the intelligent ratio (IR) through special software. To the best of our knowledge, this is the first screening test developed to quantitate SMN1 copies for screening SMA carriers with an automatized program that uses the IR and provides user-independent analyses.
Materials and Methods
Ethics approval
The study was performed after receiving approval from the local ethics committee (2012-KAEK-15/1497) in accordance with the ethical standards of the Institutional Research Committee and the 1964 Declaration of Helsinki and its later amendments. Informed consent was obtained from all of the patients and carrier parents who had been tested previously for SMN1 and SMN2 deletions with MLPA (MRC Holland SALSA MLPA P060).
Samples
Blood samples used in this study were selected from patients who applied to the Gazi University Faculty of Medicine, Department of Medical Genetics, Ankara Numune Training and Research Hospital, Department of Medical Genetics, and Dr. Sami Ulus Maternity and Children's Hospital Department of Medical Genetics between 2012 and 2017. Extra blood samples were not necessary for the study in accordance with the first consent given by the patients. Thus, extracted DNA or blood samples previously used for MLPA testing with SALSA MLPA probemix P021 SMA (MRC Holland, Amsterdam, The Netherlands) were also used for this study. Included in the study were 100 patients and of these, 30 were homozygous, 44 were carriers, and 26 were normal for SMN1 exon 7 deletion. The results obtained with MLPA were not shared with the technical team of the research wet laboratory.
DNA isolation
Genomic DNA was isolated from peripheral blood using the NucleoSpin blood DNA isolation kit (Macherey-Nagel, Duren, Germany). Next, the second and third genomic DNA extractions of the eight patients were performed using EZ1 Advanced XL (Qiagen, PL Venlo, The Netherlands) and Exgene Blood SV (GeneAll, Seoul, Korea). By using different isolation kits, it was aimed to optimize the test with different DNA extraction systems. DNA purity and concentrations, which were measured with a NanoDrop 2000 spectrophotometer (Thermo Fisher, Waltham, MA, USA), are presented in Table 1.
Purity and Concentrations of DNA Obtained Using Different Isolation Systems
A, absorbance.
Different concentrations of DNA were used to determine the minimum amount of DNA that the test system was sensitive to. For the same eight patients, the stock DNA that was isolated using the NucleoSpin kit was diluted four times at a one-third ratio (1/3, 1/9, 1/27, and 1/81, respectively).
Reference gene
In real-time PCR quantitation studies, a housekeeping gene should be used as a reference to normalize the results and compare them with each other. Thus far, many housekeeping genes have been used as references (Baris et al., 2010). In this study, although some of the recommended reference genes such as GAPDH and CFTR have been used, it was decided to use the prothrombin gene (FII; MIM* 176930) as it was the most appropriate reference in the analysis. To the best of our knowledge, the prothrombin gene has not been employed before as a reference or housekeeping gene.
Primer-probe design
Primers (P1 and P2) and a probe of the SMN1 gene were slightly modified at the C/T transition region at the position of 840 in exon 7 of the gene according to the method described previously by Maranda et al. (2012). Sequences of the primers and probe are listed for the reference gene, prothrombin, in Table 2.
Sequences of Primers and Probes of the Reference Gene FII
The probe used for SMN1 was labeled with the carboxyfluorescein dye stain, while the probe for the reference gene was marked with the Texas red dye stain.
Principle of the test system
The test principle was based on the 5′-3′ exonuclease activity of the Taq DNA polymerase. The probe has a reporter dye at the 5′ end and a quencher dye at the 3′ end. The quencher dye suppresses reporter dye irradiation and simultaneously prevents the probe from acting as a primer. In the course of PCR, the probe between the reporter and the quencher is broken apart by enzyme activity, and radiation is produced when suppression is eliminated. This process only takes place on probes hybridized over the target region. As the amount of amplification increases, luminescence increases linearly with the release of the reporter dye, and the increase is detected simultaneously.
Real-time PCR
In the study, all of the primers and probes were optimized to operate as multiplexes in a single tube. The PCR master mix included 1 × SNP PCR buffer (SNP Biotechnology, Ankara, Turkey), 3 mM of MgCl2, 0.2 mM of each dNTP, 0.8 pmol of SMN1 P1 and P2, 0.5 pmol of SMN1 probe, 0.7 pmol of prothrombin P1 and P2, 0.4 pmol prothrombin probe, 1 U of Hot Start Taq DNA polymerase, and PCR-grade water that was added to complete a total volume of 20 μL. Five microliters of DNA is added to each tube.
The PCR program, which consisted of 32 cycles, included an initial denaturation for 3 min at 95°C, denaturation for 15 s at 95°C, and annealing and extension for 1 min at 60°C and was used for amplification of the SMN1 and reference gene regions. PCR was performed using the Bio-Rad CFX 96 detection system (Hercules, CA, USA).
Standards
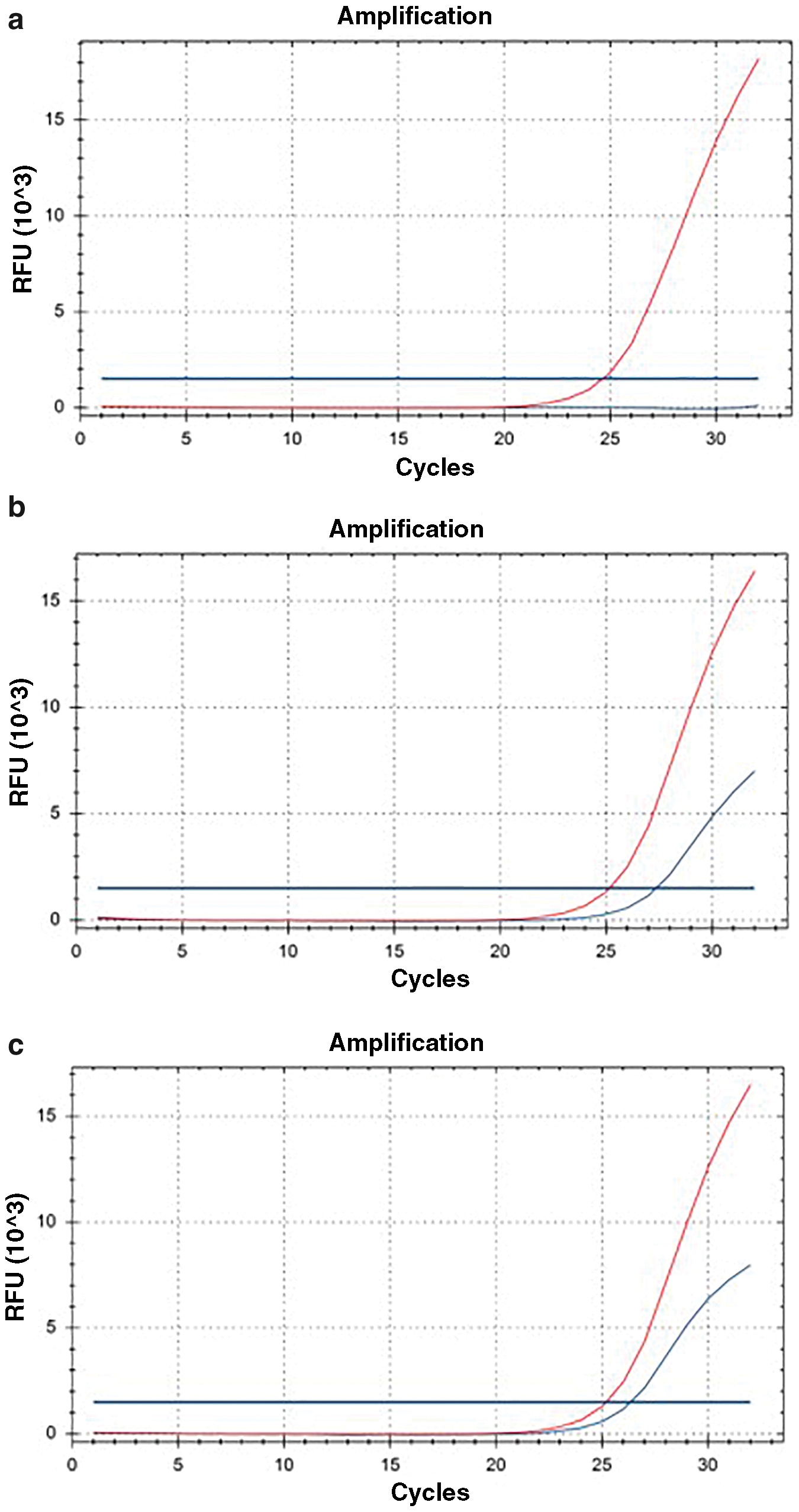
In this study, different dilution series of the synthetic plasmid of the reference gene were tested to determine the optimum slope value, which is necessary so as to reduce the invalid result range and improve the efficiency of the test system. A high level of efficiency is a requirement to obtain accurate and reproducible results. The optimum 4 dilution series were selected according to the stated criteria above, and the starting point of the amplification cycle and curves of the standards that proved the optimization are shown in Figure 1. Next, the optimized standards and slope values were transferred and integrated into special software to quantify the target and reference gene. Thus, the system did not require the usage of any tubes of standards at any point due to the integrated standards of the software.

Optimization of the standard concentrations to obtain an ideal slope value. Color images are available online.
IR method
The aim of this method was detecting 0, 1, and 2 copies of SMN1 exon 7 alleles. The IR method is based on the ratio of the reference gene to the SMN1 gene exon 7 quantification. Both quantifications of the reference gene and the SMN1 gene were detected by means of the embedded slope value in the software, and the ratio of these quantification values determined the IR value. The software gives the results automatically based on the values. Moreover, interpretation of results based on the IR can be analyzed manually (Table 3). IRs of SMA genotypes were determined using several isolation systems and different concentrations of DNA.
Interpretation of Results with the Intelligent Ratio
FAM, carboxyfluorescein; IR, intelligent ratio; SQ, starting quantity.
Results
Data were analyzed using the standard plot analyses of the real-time PCR study as well as with automated software developed on the basis of the IR method, which calculates the ratios of the target and reference genes without any standards.
Of the 100 previously studied patients, 30 had homozygous deletions of SMN1 exon 7, while 44 were detected as carriers, and 26 were normal. The results were all consistent with the previous MLPA outcomes in all of the patients studied with the screening kit. All of the samples were loaded onto a single plate to see the results in a total view (Fig. 2). Of the carriers, four could not be shown in Figure 2 due to the 96-well capacity. The evaluation of results with real-time PCR plots for heterozygous, homozygous, and normal individuals is presented in Figure 3.
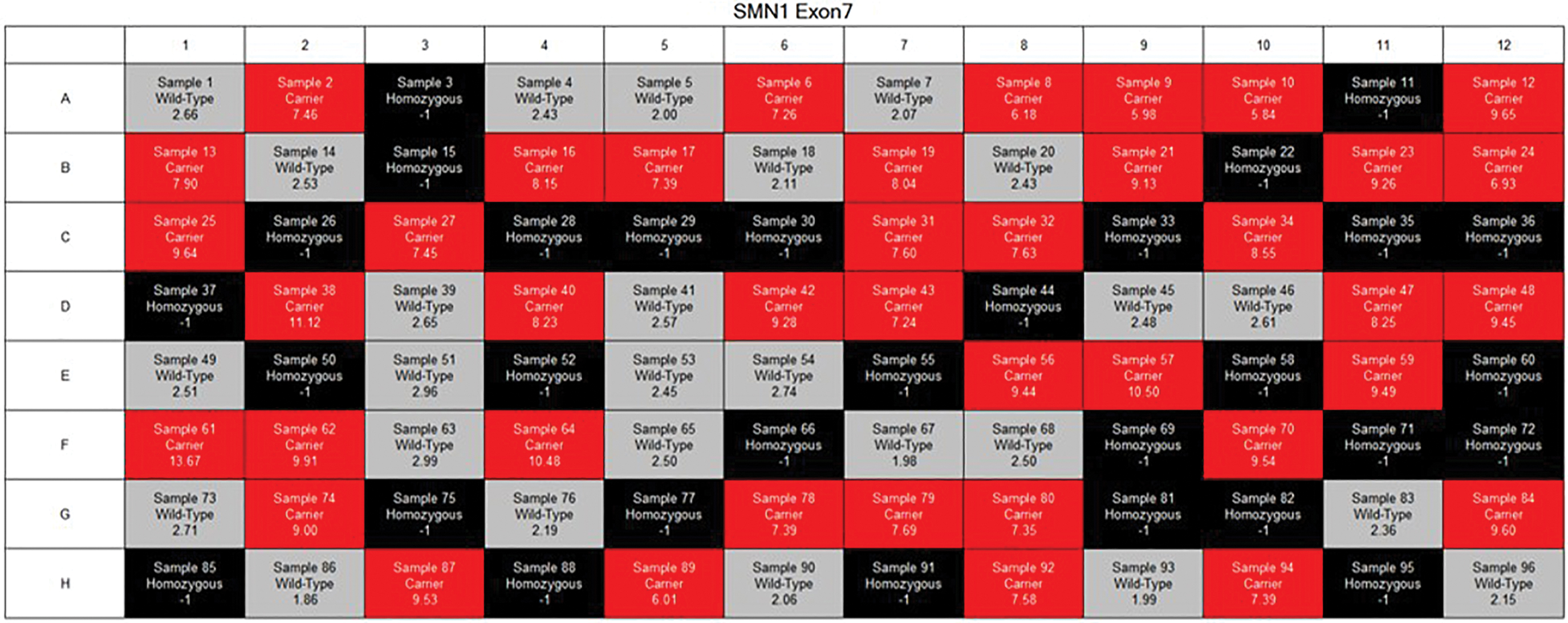
Results of the patients on the automatized software. Light gray indicates wild type (IR ≤5.50), red indicates carriers (IR ≥ 6.00), and black indicates the homozygous mutation of SMN1 (Texas red/ [N/A]: −1). IR, intelligent ratio; SMN1, survivor motor neuron 1. Color images are available online.
Analyzing the plots of the reference and target gene quantifications on real-time PCR for homozygous
Tests using different concentrations of DNA in each tube and using DNA obtained with different isolation kits are presented in Figure 4. IR values were determined within the same range, giving the same result as the test used for DNA for all of the concentrations. The results were also the same for the test performed using DNA obtained through the three extraction systems.
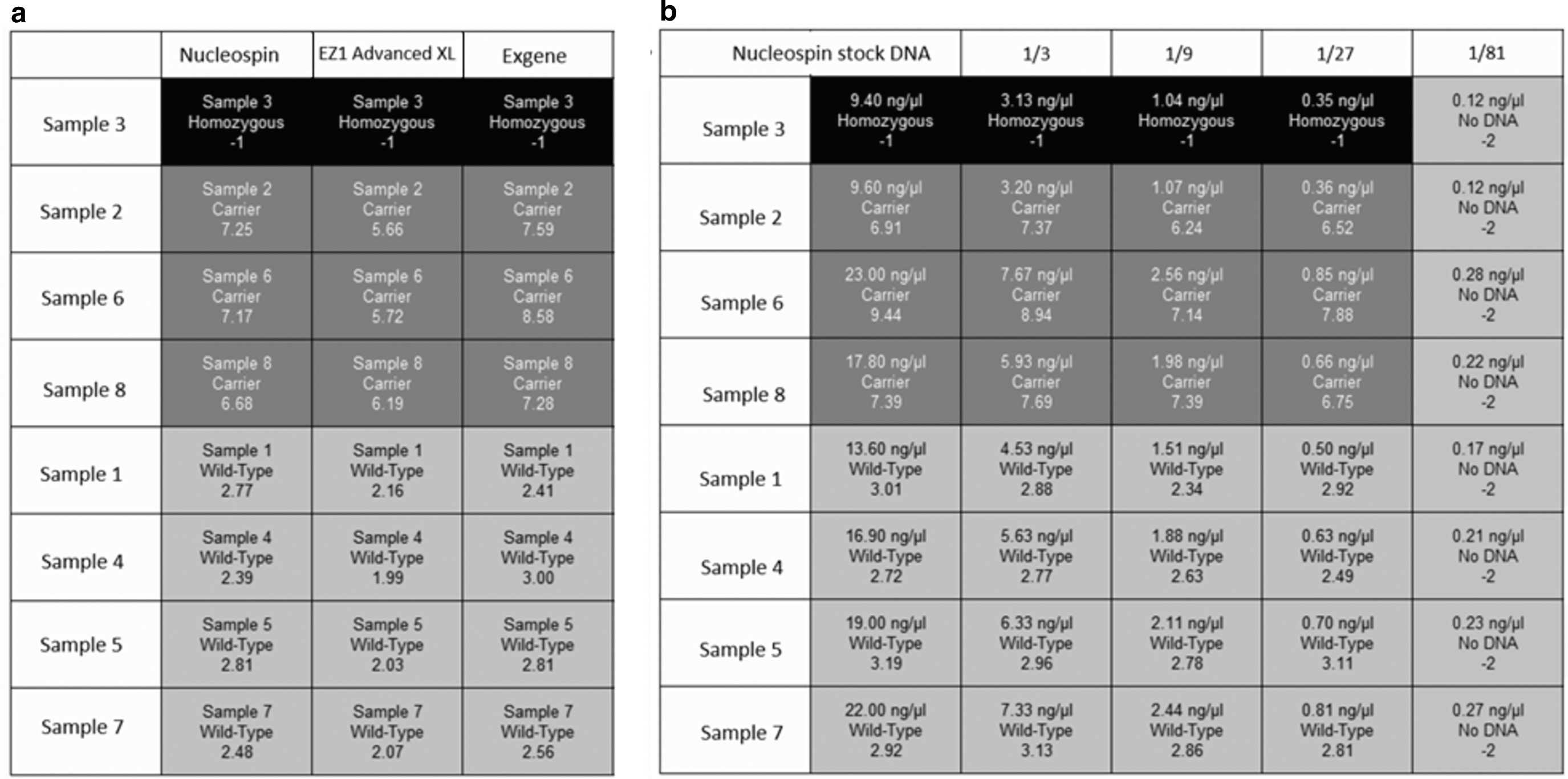
Evaluation of results obtained by different isolation kits
The true positive rate, that is, sensitivity and specificity of the test, was calculated as 1 because there were no false negative (FN) or false positive (FP) results, respectively (Table 4).
Evaluation of the Standard Values for a Method According to the Results
FN, false negative; FP, false positive; TN, true negative; TP, true positive.
Discussion
SMA is one of the most prevalent neuromuscular diseases with autosomal recessive inheritance. The majority of this group of diseases is caused by the homozygous deletion of exon 7 of the SMN1 gene (Markowitz et al., 2004; Prior et al., 2010; Verhaart et al., 2017).
Premarital or newborn screening for SMA has been a current issue due to its high prevalence and carrier frequency. Because of high morbidity and mortality and treatment costs of the disease, screening has become a public health problem. Although major advances have been observed in the treatment of SMA recently, it is not possible to treat the disease completely. Thus, treatment effectiveness in patients with delayed diagnosis remains undefined. Therefore, high costs and difficulties in the availability of treatment medication have motivated researchers to search for alternative ways to prevent the disease.
One of the main aims of SMA screening of newborns is to provide early diagnosis and begin treatment without the neural loss seen within the first 6 months in infants. Therefore, when an infant carrier of SMA is detected through neonatal screening, the parents could be screened before subsequent pregnancies. It should be recommended that all identified parents should attend genetic counseling, and prenatal or preimplantation diagnosis for their future pregnancies should be offered.
Thus far, various screening tests have been developed based on a wide range of methods. Some disadvantages have been experienced, such as difficulties in the application process, high prices, technician-based faults, and nonautomated and subjective analyses (Prior et al., 2011; Vidal-Folch et al., 2018; Cao et al., 2019; Xia et al., 2019). However, these highly sensitive and specific methods have many advantages on quantification and diagnosis (Table 5). In a screening kit, accuracy, reliability, and easy applicability are essential parameters, and it is very important to have quick and standardized results. The IR was developed for analyzing results and it was integrated into the software to eliminate errors based on subjective analyses. Thus, the IR provided quick, automated, and user-independent accurate results that could be determined within the software. Due to the software having integrated standards, subsequent studies do not require the usage of standards repetitively.
Summary of the Basic Advantages and Disadvantages of the Methods Used for Spinal Muscular Atrophy Diagnosis and/or Carrier Screening
PCR, polymerase chain reaction; RFLP, restriction fragment length polymorphism; SMN1, survivor motor neuron 1.
This SMA screening method was based on the c.840C>T variant in exon 7 in the SMN1 gene. Therefore, the method could not detect other rare mutations (2-4%) that caused SMA, although it was possible to detect the compound heterozygous mutations for SMN1. If an infant was detected as a carrier with one deleted SMN1 allele, the SMN1 gene would be sequenced to define whether the other allele had any intragenic mutations. Likewise, in premarital screening, sequencing for intragenic mutations could be performed for one of the parents if the other has been detected as a carrier for SMN1 deletion (Srivastava and Srivastava, 2019). The presented kit can direct patients with heterozygous deletions or the partners of carriers to be screened for any possible point mutations. As a result, it is useful for carrier and newborn screening as well as in early diagnosis and prevention of the disease.
According to the comparison of results with those of the MLPA, the sensitivity, specificity, efficiency, and accuracy of the kit were all detected as 100% (Table 3). In this study, software was automatized for interpretation of results without any calculations. It was useful for obtaining user-independent results. Although the program is currently adapted for Bio-Rad CFX 96, it is aimed to adapt the automated program for other standard systems.
We used three, different, commercial DNA extraction kits for the first eight patients of the study group. Purity and concentration of DNA were measured (Table 1) and three independent tests were performed. All of the other factors of the study were implemented under standard conditions. All three tests obtained similar IR values, which were determined as the same results (Fig. 4a), although the purity of some DNA samples was not within the expected range since the study was not performed with fresh blood samples. The test was compatible with most of the other DNA extraction systems and did not require fresh blood samples and it was also superior to other screening kits on the market.
To determine the minimum sensitivity of the assay for the amount of DNA, the DNA, which was extracted using a NucleoSpin kit, was diluted in four consecutive series. It was determined that the required amount of DNA should be at least 0.01 ng, which is less than the amount of DNA that can be detected by all of the other isolation kits/systems on the market (Fig. 4b). Consequently, the amount of DNA did not affect the results. The test was easily applicable since it did not require DNA measurements after isolation.
The advantages and disadvantages of some methods are summarized, according to the technical guideline developed by Prior et al. (2011), in Table 5. Methods such as MLPA, quantitative PCR, and digital droplet PCR can detect the number of SMN2 copies (Table 5). Since screening tests should be applied to a large proportion of the population (premarital or newborns), it should be fast, reliable, and cost-effective. Although the current method cannot quantitate the number of SMN2 copies, SMA can be subclassified by diagnostic methods in case of suspicion of SMA in a patient. The method is cost-effective for SMA screening as it costs lower compared with counterparts and also 96 samples can be run simultaneously without the need of additional standard tubes.
This screening method quantitates the copies of the SMN1 gene. In normal individuals, two copies of the SMN1 gene are found in separate alleles (1 + 1). However, in rare cases (1-4%), there is no SMN1 gene in one of the alleles, while two SMN1 genes may be present in the other (0 + 2). In this case, the test results are normal (FN) due to detection of two copies of SMN1. However, the subject is a carrier for SMA. Consequently, it is not possible to determine whether two of the copies of SMN1 are in the same allele (cis) in any method used in SMA diagnosis or carrier screening (Table 5).
SMA is the result of a common single deletion event in 95% of cases, thus the methods developed to identify copy number variations are very sensitive. The new suggested technique cannot detect point mutations, which is a common disadvantage for all types of kits used for SMA screening (Kraszewski et al., 2018) (Table 5). In addition, all the primer and/or probe-based methods (MLPA, PCR-RFLP, and quantitative PCR) have the risk of FP results because of a possible sequence variant in the binding site. Direct DNA sequencing is used to detect intragenic point mutations. However, due to the high homology of SMN1 and SMN2, it is necessary to perform allele-specific sequencing for all identified variants (Prior et al., 2011).
Methods such as MLPA, PCR-RFLP, and digital PCR are multistep tests, so they are prone to technical errors. However, in the current test, unmeasured DNA is added to the ready PCR master mix and then loaded into the device in a single step. Therefore, it is easy to apply and technician-based errors are also minimal. PCR-RFLP and quantitative PCR are relatively low-cost methods such as the presented method. While carriers cannot be detected in PCR-RFLP, quantitative PCR has disadvantages such as misinterpretation of the melting and quantitation curves during analyses. In this method, carriers can be detected and a user-independent analysis is provided (Table 5).
In conclusion, a new, quantitative SMA screening kit using the IR, and in which FII is used as a reference gene for the first time, was developed to obtain accurate, reliable, efficient, highly sensitive, and specific results. In addition, the kit did not require standards and sample DNA measurements. The new automated and user-independent test provides the opportunity for early and sensitive detection of carriers or homozygous patients with SMN1 deletion, within 70 min from their blood.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study has been supported by SNP Biotechnology Ltd.