
Abstract
Objective:
The long-chain noncoding RNA (lncRNA) TINCR has been associated with the development and progression of bladder cancer. In this study, we analyzed the correlation between lncRNA TINCR single-nucleotide polymorphisms (SNPs) and bladder cancer susceptibility risk.
Methods:
The genotypes of the lncRNA TINCR rs2288947 and rs8113645 loci in 125 surgically treated bladder cancer patients and 125 controls were analyzed by Sanger sequencing. A dual-luciferase reporter gene assay was used to detect the binding of the microRNAs miR-1247-3p and miR-30c-2-3p with the lncRNA TINCR. The receiver operating characteristic curve was used to analyze the value of expression levels of the lncRNA TINCR and the microRNAs miR-1247-3p and miR-30c-2-3p in the diagnosis of bladder cancer.
Results:
The bladder cancer susceptibility risk of the rs2288947 G allele carriers was 2.32 times higher compared with the A allele carriers (95% confidence interval [CI]: 1.58-3.42, p < 0.01); The bladder cancer susceptibility risk of the rs8113645 T allele carriers was 0.33 times compared with the C allele carriers (95% CI: 0.19-0.55, p < 0.01). lncRNA TINCR was more highly expressed in bladder cancer tissues than controls (p < 0.01). The lncRNA TINCR rs2288947 A>G variation was associated with increased expression of lncRNA TINCR in bladder cancer tissues, and the rs8113645 C > T was associated with decreased expression. The expression levels of the lncRNA TINCR in cancer and paracancerous tissues showed a significant negative correlation with that of miR-1247-3p and miR-30c-2-3p (r = −0.89, −0.78, −0.81, and −0.66, all p < 0.01). The dual-luciferase reporter gene assay results indicate that the lncRNA TINCR rs2288947 G allele is the target of miR-1247-3p, and the rs8113645 C allele is the target of miR-30c-2-3p.
Conclusion:
The lncRNA TINCR rs2288947 A>G is associated with increased bladder cancer risk and rs8113645 C > T is associated with decreased susceptibility. These two SNP loci are associated with lncRNA TINCR expression levels; however, further studies are needed for validation.
Introduction
Bladder cancer is a common malignant tumor of the urinary system and one of the most frequent malignant tumors in the world. The 5-year survival rate of patients with aggressive bladder cancer is less than 60% (Dancik and Theodorescu, 2014). Although environmental factors such as smoking and occupational exposure are the major risk factors of bladder cancer (Koutros et al., 2016; Cumberbatch et al., 2018; Colin et al., 2018; Hadkhale et al., 2019), it is proved that genetic factors also play a role in the development of bladder cancer (Zhang and Zhang, 2015; Chiang et al., 2018; Song et al., 2019).
Long-chain noncoding RNA (lncRNA) is the regulatory RNA molecule of endogenous noncoding RNA, which has a regulatory function in different biological processes, such as chromosome inactivation and genomic imprinting and development (Autuoro et al., 2014). Recent studies showed that lncRNAs are abnormally expressed in a variety of malignant tumors, including bladder cancer (Yin et al., 2015; Chen et al., 2016; He et al., 2018).
Terminal differentiation-induced ncRNA (TINCR), located on 19p13.3, is a 3.7-kilobase transcript, which controls the differentiation of human epithelial tissues. Some studies indicate that TINCR is downregulated in human squamous cell carcinoma (Kretz et al., 2013; Sun et al., 2015; Lopez-Pajares et al., 2015). In addition, some researchers have found that TINCR expression is upregulated in bladder cancer tissues, which is associated with the development and progression of bladder cancer (Chen et al., 2016). Silencing TINCR can inhibit cell proliferation and activate apoptosis in vitro, suggesting that TINCR is the potential therapeutic target for treating bladder cancer.
With the advancement of sequencing technology, the gene polymorphism of lncRNA has been more and more elucidated, and used for the risk prediction of tumor development and progression (Zheng et al., 2017; Huang et al., 2019). In this study, we found two single-nucleotide polymorphism (SNP) loci, rs2288947 and rs8113645, respectively, at the binding sites of lncRNA TINCR with microRNAs by bioinformatics technology. rs2288947 is located at the binding site of the lncRNA TINCR with miR-1247-3p and rs8113645 is located at the binding site of the lncRNA TINCR with miR-30c-2-3p. According to dbDEMC 2.0 database, the expression of miR-1247-3p and miR-30c-2-3p is downregulated in bladder cancer. In this study, we analyzed the association of lncRNA TINCR SNPs rs2288947 and rs8113645 with its expression levels with bladder cancer susceptibility.
Materials and Methods
Subjects
In this study, we focused on 125 patients with bladder cancer, who underwent surgical treatment in our hospital from October 2017 to October 2019, including 105 male patients and 20 female patients, 45-79 years of age, with an average age of 63.10 ± 10.95 years. All patients were postoperatively diagnosed with bladder cancer by two pathologists based on a pathologic diagnosis. We collected tumor tissue samples during bladder cancer surgery, and the paracancer tissue was collected at least 5 cm away from the cancer tissue. Inclusion criteria: (1) patients with the lesion diagnosed as bladder urothelial carcinoma; (2) patients who took the transurethral resection of bladder tumor in our hospital; (3) patients who received no radiotherapy or chemotherapy; and (4) patients who signed informed consent. Exclusion criteria: (1) patients with other types of bladder cancer; (2) patients with other malignant tumors; (3) pregnant or lactating women; and (4) patients with incomplete clinical data. One hundred twenty-five subjects with healthy physical examinations for non-bladder cancer were selected as a control group based on the age and sex of bladder cancer patients, including 103 men and 22 women, 33-88 years of age, with a mean age of 63.10 ± 10.95 years. Exposure to hazardous materials (aromatic amines, polycyclic aromatic hydrocarbons, diesel, etc.) at work is considered a high risk. Our research protocol was approved by the Medical Ethics Committee of Zibo Central Hospital, and informed consent was obtained from all subjects.
Detection of gene polymorphisms
The whole blood genomic DNA of subjects was extracted by the TIANamp Blood DNA kit (Tiangen Biotech, Beijing, China). The genotypes of subjects were analyzed by Sanger sequencing. The primer sequence for amplifying rs2288947 is 5′-ACC TGG AGT GAG ATC TAG GCT-3′ (forward primer) and 5′-AAT AGG CTG GGG TAG AGG GC-3′ (reverse primer). The primer sequence for amplifying rs8113645 is 5′-CTG CAA TCC CAG GTG TAT TGG-3′ (forward primer) and 5′-GCT CTT GCC CAG GAC ATT TT-3′ (reverse primer). The polymerase chain reaction (PCR) system contains 5 μL 10 × Taq buffer, 3 μL MgCl2 (25 mM), 2 μL forward primer (10 μM), 2 μL reverse primer (10 μM), 1 μL dNTP Mix (10 mM), 4 μL template DNA (25 ng/μL), and 32.5 μL ddH2O. Reaction conditions: 90°C predenaturation for 5 min; 94°C denaturation for 30 s; 56°C annealing for 30 s; and 72°C extension for 60 s; 35 cycles in total; and at last 72°C extension for 7 min. The PCR products were analyzed by Sanger sequencing, and the results were compared with the data of the dbSNP database to confirm the genotypes.
Real-time quantitative PCR analysis
Total RNA was extracted from bladder cancer tissues using Trizol LS reagent (Invitrogen, Inc., Carlsbad, CA) according to the manufacturer's instructions and cDNA was synthesized using M-MLV reverse transcriptase (Clontech, Palo Alto, CA). Real-time quantitative PCR (qRT-PCR) was conducted on the ABI 7500 thermal cycler (Applied Biosystems) using SYBRGreen MasterMix (Bio-Rad, Hercules, CA) according to the manufacturer's instructions to detect the relative expression level of lncRNA TINCR using GAPDH as the reference gene, and the relative expression levels of miR-1247-3p and miR-30c-2-3p, using β-actin as the reference gene. The primer sequence of U6 is 5′-GAT TAG AAC CGT CGG TAA CGG AA-3′ (forward primer) and 5′-AGC GAT CTC GTT GGC CTT TCT ACC-3′ (reverse primer). The primer sequence of GAPDH is 5′-TGA AGG TCG GAG TCA ACG G-3′ (forward primer) and 5′-CCT GGA AGA TGG TGA TGC G-3′ (reverse primer). The primer sequence of lncRNA TINCR is 5′-TGT GGC CCA AAC TCA GGG ATA CAT-3′ (forward primer) and 5′-AGA TGA CAG TGG CTG GAG TTG TCA-3′ (reverse primer). The primer sequence of miR-1247-3p is 5′-CAC CCG TCC CGT TCG TC-3′ (forward primer) and 5′-GAA GGT GGC TCA GTT CGG G-3′ (reverse primer). The primer sequence of miR-30c-2-3p is 5′-ATA CTG TAA ACA TCC TAC ACT CTC A-3′ (forward primer) and 5′-AGA AAG AGT AAA CAG CCT TCT CC-3′ (reverse primer). The relative expression levels of lncRNA TINCR, miR-1247-3p, and miR-30c-2-3p were analyzed using the 2−▵▵CT method.
The Luciferase reporter gene assay
T24 cells were seeded in 24-well plates (1 × 105/well) and cultured for 24 h. Then pGL3-rs2288947 G allele promoter vectors, pGL3-rs2288947 A allele promoter vectors, 50nM miR-1247-3p mimic, and template-free control (NC) were co-transfected in T24 cells using Lipofectamine 2000 (Invitrogen, Inc.). Likewise, pGL3-rs8113645 T allele promoter vectors, pGL3-rs8113645 C allele promoter vectors, 50 nM miR-30c-2-3p, and template-free control (NC) were co-transfected in T24 cells. Forty-eight hours after transfection, luciferase activity was measured using the dual-luciferase reporter assay system (Promega, Madison, WI).
Statistical analysis
Statistical analysis was carried out using the χ2 test for the categorical variables and using the t-test and one-way analysis of variance for the continuous variables with a normal distribution. Whether the genotypes of the control group conformed to the Hardy-Weinberg equilibrium was analyzed by χ2 test. The association of the genotypes and allele frequencies and dominant model and recessive model of the lncRNA TINCR rs2288947 and rs8113645 with bladder cancer susceptibility was analyzed by logistic regression, and the odds ratio (OR) and 95% confidence interval (CI) were calculated, with adjustment for age, sex, smoking condition, alcohol consumption, occupational exposure, and chronic bladder inflammation. The receiver operating characteristic (ROC) curve was used to evaluate the diagnostic values of lncRNA TINCR, miR-1247-3p, and miR-30c-2-3p. Statistical analysis was performed using GraphPad Prism 8 (GraphPad Software, Inc., San Diego, CA) and SPSS 22.0 (SPSS, Chicago, IL). All statistical tests were two sided and p < 0.05 was considered significantly significant.
Results
Clinical characteristics
The clinical characteristics of 125 patients with bladder cancer and 125 controls recruited in this study are shown in Table 1. Among 125 bladder cancer patients, there were 77 patients with non-muscle invasive bladder cancer and 28 with invasive bladder cancer. There were 22 TNM I patients, 31 TNM II patients, 35 TNM III patients, and 37 TNM IV patients. The pathological grading was in accordance with WHO standards. There were 25 cases of G1 grade, 56 cases of G2 grade, and 44 cases of G3 grade. Among them, there were 16 patients with chronic bladder inflammation, accounting for 12.80%. The analysis results suggested that there were no significant differences between bladder cancer patients and the controls in clinical characteristics, including age, sex, smoking condition, and drinking condition. The proportion of bladder cancer patients with occupational exposure and chronic bladder inflammation was significantly higher than that in the control group (p < 0.05).
Comparison of Clinical Characteristics Between Bladder Cancer Patients and the Controls
Case, bladder cancer.
SD, standard deviation; TNM, tumor-node-metastasis.
Association between lncRNA TINCR polymorphisms and bladder cancer susceptibility
In this study, the genotype frequencies of lncRNA TINCR rs2288947 and rs8113645 in the control group conformed to the Hardy-Weinberg equilibrium (p = 0.10, 0.20) (Table 2). Taking the AA allele of rs2288947 as the reference gene, we found that there was no correlation between AG genotype and bladder cancer susceptibility, the bladder cancer susceptibility risk of GG genotype carriers was 4.56 times higher (95% CI: 2.07-10.06, p < 0.01) and that of the dominant model (AG+GG vs. AA) and recessive model (GG vs. AA+AG) carriers was 2.11 times and 3.96 times higher (95% CI: 1.85-8.47, p < 0.01). The bladder cancer susceptibility risk of G allele carriers is 2.32 times higher compared with A allele carriers.
Association Between Genotypes and Allele Frequencies of lncRNA TINCR rs2288947 and rs8113645 and Bladder Cancer Susceptibility Risk
CI, confidence interval; HWE, Hardy Weinberg equilibrium; lncRNA, long-chain noncoding RNA; OR, odds ratio.
Taking the CC genotype of rs8113645 as the reference gene, we found that the CT genotype was significantly associated with decreased bladder cancer risk (OR = 0.26, 95% CI: 0.13-0.51, p < 0.01). There was no significant correlation between the TT genotype and bladder cancer susceptibility risk. The dominant model was significantly associated with decreased bladder cancer susceptibility risk, while the recessive model found no association. The bladder cancer susceptibility risk of T allele carriers is 0.33 times that of C allele carriers.
Stratified analysis
We stratified the subjects by age, gender, smoking condition, drinking condition, occupational exposure, and chronic bladder inflammation and the analysis results revealed that the bladder cancer susceptibility risk of rs2288947 dominant model carriers only rose among patients who were <60 years old (adjusted OR = 2.76, 95% CI: 1.20-6.35, p = 0.027) and are male (adjusted OR = 2.29, 95% CI: 1.31-4.00, p = 0.005), smokers (adjusted OR = 1.85, 95% CI: 1.17-2.92, p = 0.006), drinkers (adjusted OR = 2.43, 95% CI: 1.18-5.02, p = 0.025), having high-risk occupations (adjusted OR = 1.61, 95% CI: 1.09-2.24, p = 0.013), and with chronic bladder inflammation (adjusted OR = 2.17, 95% CI: 1.01-3.40, p = 0.046), and those without chronic bladder inflammation (adjusted OR = 1.34, 95% CI: 1.01-1.79, p = 0.046) (Table 3).
The Stratified Analysis of lncRNA TINCR rs2288947 SNPs and Bladder Cancer Susceptibility Risk
SNP, single-nucleotide polymorphism.
Only among patients who were female (Adjusted OR = 0.54, 95% CI: 0.13-2.21, p = 0.604), nondrinkers (Adjusted OR = 0.58, 95% CI: 0.25-1.33, p = 0.2774), and with chronic bladder inflammation (Adjusted OR = 0.61, 95% CI: 0.12-1.24, p = 0.475), the bladder cancer susceptibility risk of the lncRNA TINCR rs8113645 dominant model carriers had no significant change, but significantly changed in other stratification (Table 4).
Stratified Analysis of lncRNA TINCR rs8113645 SNPs and Bladder Cancer Susceptibility Risk
In this case, the association between the SNP of rs2288947 in the lncRNA TINCR and bladder cancer susceptibility risk was affected by the factors of age, gender, smoking, drinking condition, and occupational exposure, whereas the association between the SNP of rs8113645 in lncRNA TINCR and bladder cancer susceptibility risk was only related to the factors of gender, drinking condition, and chronic bladder inflammation.
Association between lncRNA TINCR polymorphisms and tumor invasion, tumor stage, and tumor grades of bladder cancer patients
Association between different genotypes of rs2288947 and rs8113645 in the lncRNA TINCR and tumor invasion is illustrated in Table 5. The analysis results showed that there was no significant association between rs2288947 SNP and tumor invasion (p > 0.05) and the frequency of rs8113645 T allele was higher among non-muscle invasive bladder cancer patients.
Association Between lncRNA TINCR rs2288947 and rs8113645 Polymorphisms and Tumor Invasion
Correlation between different genotypes of rs2288947 and rs8113645 in the lncRNA TINCR and tumor stage is illustrated in Table 6. No significant correlation was found between SNPs rs2288947 and rs8113645 and tumor stage (p > 0.05).
Association Between lncRNA TINCR rs2288947 and rs8113645 Polymorphisms and TNM Stage
Correlation between different genotypes of rs2288947 and rs8113645 in the lncRNA TINCR and tumor grades is illustrated in Table 7. The results showed that carriers of rs2288947 G allele had a higher tumor grade (p < 0.01), but there was no correlation between SNP rs8113645 and tumor grade.
Correlation Between lncRNA TINCR rs2288947 and rs8113645 Polymorphisms and Tumor Grades
Upregulated expression of lncRNA TINCR in bladder cancer tissues, the potential diagnostic marker for bladder cancer
We extracted total RNA from the tumor tissues and adjacent normal tissues (5cm away from the tumor tissue) resected in 125 bladder cancer surgeries and analyzed the relative expression levels of lncRNA TINCR, the result of which indicated that lncRNA TINCR was highly expressed in bladder cancer tissues (p < 0.01, Fig. 1A). The results of the ROC curve analysis showed that the area under the curve (AUC) of lncRNA TINCR expression level in the diagnosis of bladder cancer was 0.68 (95% CI: 0.54-0.84, p < 0.01, Fig. 1B). We found no significant difference in lncRNA TINCR expression levels between non-muscle invasive tumor tissues and invasive tumor tissues, while the expression levels in TNM III/IV tumor tissues were higher than those in TNM I/II tumor tissues (p = 0.047, Fig. 1D). The expression levels of lncRNA TINCR were higher in high-grade tumor tissues (p < 0.01, Fig. 1E).

lncRNA TINCR abnormally highly expressed in the bladder cancer tissues.
Association between lncRNA TINCR polymorphisms and lncRNA TINCR expression levels in cancer tissues
We analyzed lncRNA TINCR expression levels in bladder cancer tissues of patients with different genotypes of rs2288947 and rs8113645 in the lncRNA TINCR and found that lncRNA TINCR expression levels were highest in bladder cancer tissues of patients with rs2288947 GG genotype, followed by AG genotype and AA genotype. The difference between these three genotypes is statistically significant (p < 0.001, Fig. 2A). lncRNA TINCR expression levels in bladder cancer tissues of patients with rs8113645 CC genotype were highest, followed by CT genotype and TT genotype, and the difference between three genotypes was statistically significant (p = 0.021, Fig. 2B).
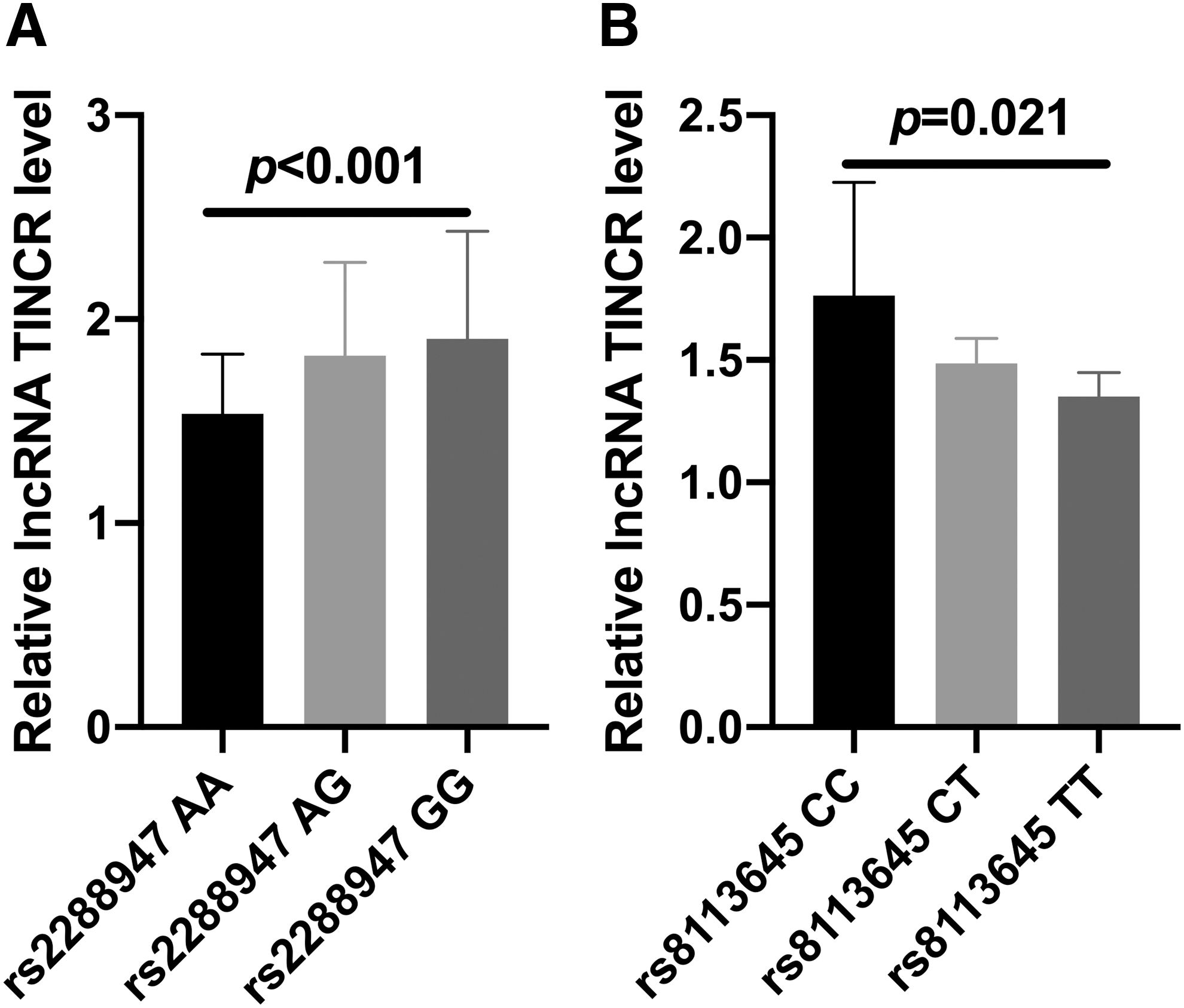
The association between lncRNA TINCR polymorphisms and lncRNA TINCR expression levels in cancer tissues.
Thus, lncRNA TINCR rs2288947 A>G variation was associated with increased lncRNA TINCR expression levels in bladder cancer tissues, while lncRNA TINCR rs8113645 C > T variation was correlated with decreased lncRNA TINCR expression levels.
The downregulated expression of miR-1247-3p and miR-30c-2-3p in bladder cancer tissues, a potential marker of bladder cancer
The expression levels of miR-1247-3p and miR-30c-2-3p in bladder cancer tissues were analyzed using qRT-PCR and the results indicated that the expression levels of miR-1247-3p and miR-30c-2-3p are significantly lower than those in paracancer tissues, and the differences were statistically significant (p < 0.001, Fig. 3A, C). The AUC of the ROC curve of miR-1247-3p and miR-30c-2-3p expression levels in the diagnosis of bladder cancer was up to 0.89 (95% CI: 0.86-0.93, p < 0.01, Fig. 3B) and 0.87 (95% CI: 0.83-0.92, p < 0.01, Fig. 3D), respectively.
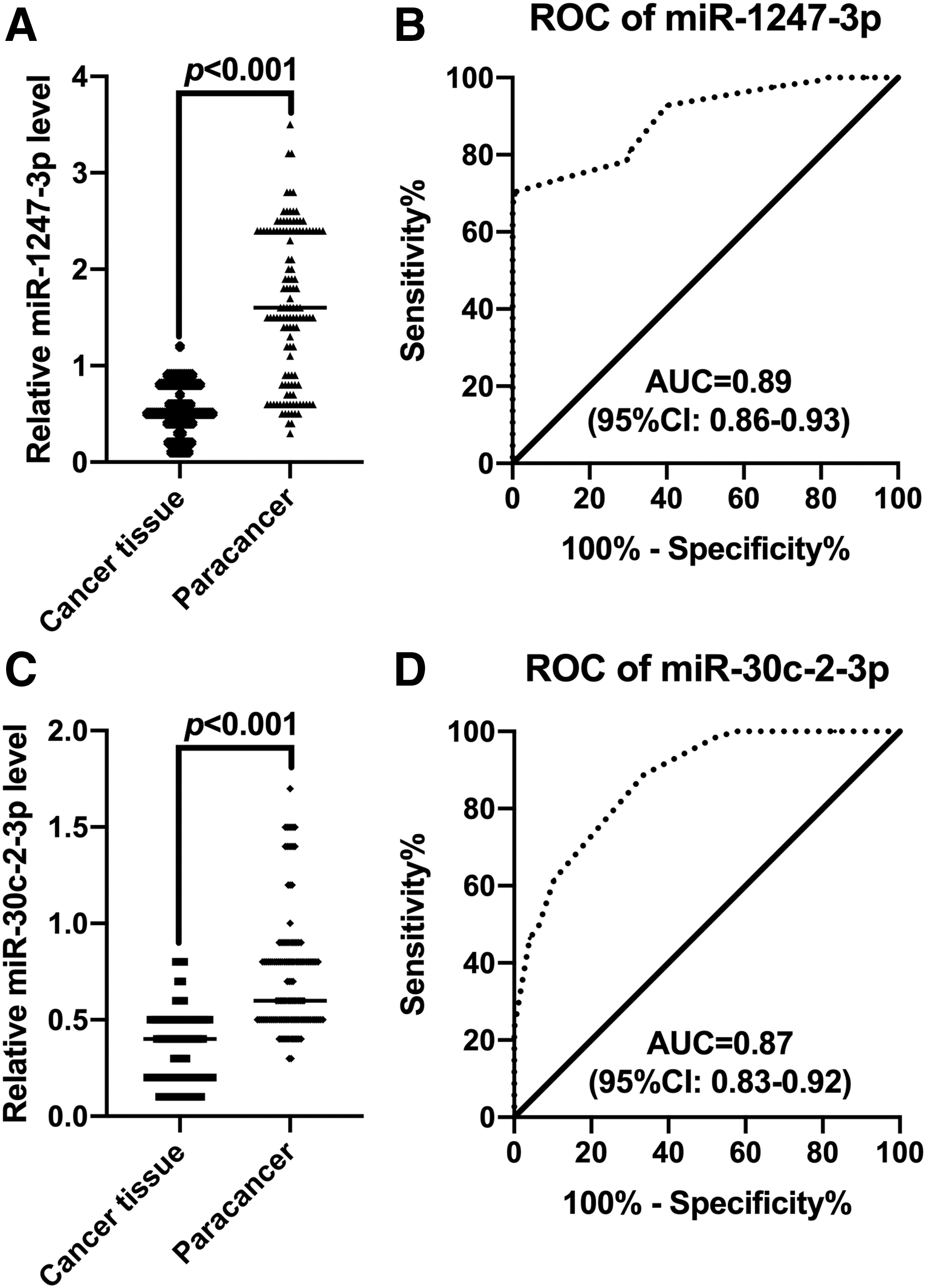
The expression levels of miR-1247-3p and miR-30c-2-3p in bladder cancer tissues.
Pearson correlation was performed to analyze the correlation between the expression levels of lncRNA TINCR and those of miR-1247-3p and miR-30c-2-3p in cancer tissues and normal paracancerous tissues of bladder cancer patients, and results revealed that lncRNA TINCR expression levels were significantly negatively correlated with both miR-1247-3p and miR-30c-2-3p levels in cancer tissues and paracancer tissues (r = −0.89, −0.78, −0.81, −0.66, all p < 0.01, Fig. 4A-D).

Correlation between the expression levels of lncRNA TINCR and those of miR-1247-3p and miR-30c-2-3p in bladder cancer tissues.
Correlation between lncRNA TINCR polymorphisms and the expression of miR-1247-3p and miR-30c-2-3p
We attempted to further analyze the expression levels of miR-1247-3p and miR-30c-2-3p in the different genotypes of lncRNA TINCR rs2288947 and rs8113645. The results showed that rs2288947 SNP was significantly associated with the expression levels of miR-1247-3p no matter in the cancer tissues or paracancer tissues (p = 0.03, p < 0.01, Fig. 5A, B), while rs8113645 SNP was significantly associated with the expression levels of miR-30c-2-3p (p < 0.01, p < 0.01, Fig. 5C, D).
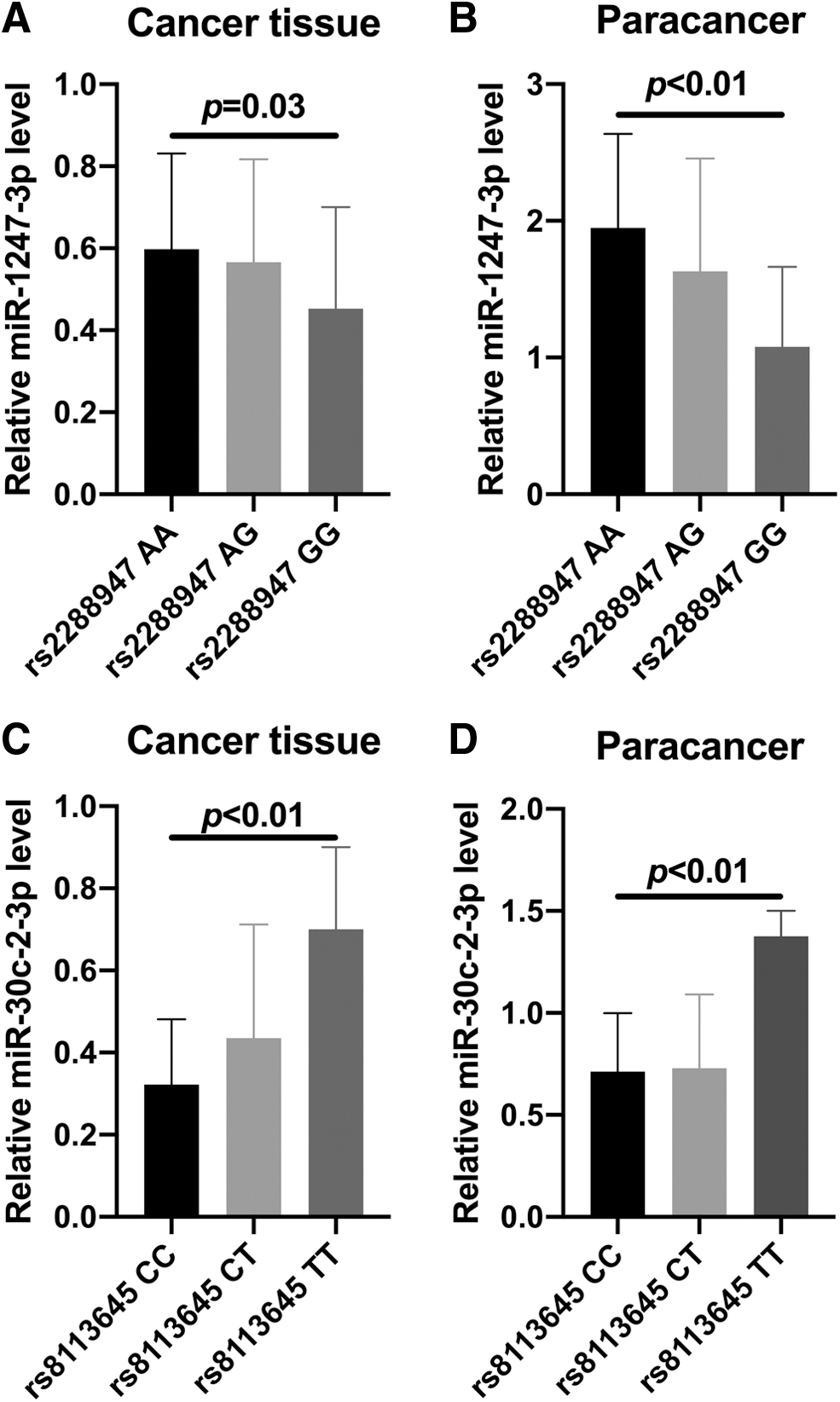
Association between lncRNA TINCR rs2288947 and rs2288947 SNPs in cancer and paracancer tissues and the expression levels of miR-1247-3 and miR-30c-2-3p.
lncRNA TINCR rs2288947 G allele, not A allele, is the target gene of miR-1247-3p; rs8113645 C allele, not T allele, is the target gene of miR-30c-2-3p
We predicted by bioinformatics analysis that there was a binding site for miR-1247-3p on the G allele of rs2288947 and a binding site for miR-30c-2-3 on the C allele of rs8113645 (Fig. 6A). The results of dual-luciferase reporter assay showed that the rs2288947 G allele was the target gene of miR-1247-3p, rather than A allele (Fig. 6B), and the rs8113645 C allele was the target gene of miR-30c-2-3p, rather than T allele (Fig. 6C).

The dual-luciferase reporter assay.
Discussion
Bladder cancer is one of the most common urinary malignancies and its morbidity and mortality are fairly high. Tumor recurrence and metastasis is the main cause of death in patients with bladder cancer (Martinez Rodriguez et al., 2017; Grayson, 2017; Farling, 2017). At present, the treatment for it is mainly based on surgery, but due to the multicentric origin of bladder cancer, which causes it to be easy to possess the characteristics of drug resistance, invasiveness, and recurrence, the current studies on bladder cancer mainly focus on finding effective targets to regulate the biological characteristics of bladder cancer at the source (Pham and Ballas, 2019). The development and procession of bladder cancer are affected by many factors such as DNA mutation, protein abnormality, and RNA abnormality.
lncRNAs are a class of noncoding RNAs, widely existing in cells. In-depth research on tumor pathogenesis makes scholars, both domestic and overseas, realize that lncRNAs can play a crucial regulatory role in various tumors. The regulatory function of lncRNAs on tumors is mainly by affecting cell surface modification, signaling pathway, and RNA editing (Zheng et al., 2016; Wang et al., 2018; Huang 2018). An increasing number of reports indicated that the dysregulated expression of lncRNAs is closely correlated with the pathological mechanisms of a variety of cancers, including bladder cancer; hence, lncRNAs are expected to become molecular targets for clinical diagnosis and treatment of tumors in the future.
TINCR is an lncRNA required to induce key differentiation genes in epidermal tissues and is also a mutated gene in human dermatoses characterized by disruption of the epidermal barrier (Kretz, 2013). TINCR can abnormally express in a variety of malignant tumors and function as a molecular marker for early diagnosis of tumors and one of the prognostic predictors (Chen et al., 2016; Dong et al., 2019; Zhang et al., 2019; Hu et al., 2020; Xu et al., 2020). For example, TINCR specifically binds with epithelial cell adhesion molecule (EpCAM), and downregulation of TINCR promotes the hydrolysis of EpCAM, which then releases the intracellular domain and subsequently activates the Wnt/beta-catenin pathway (Zhang et al., 2016). Further studies found that the c-myc gene can inhibit TINCR expression by inhibiting the transcriptional activity of sp1, suggesting that downregulation of TINCR expression level facilitates the proliferation and metastasis of CRC cells, so TINCR can be considered a potential cancer suppressor gene.
The study results showed that the expression of lncRNA TINCR is upregulated in bladder cancer tissues. Although no difference of lncRNA TINCR expression levels was found between invasive and non-muscle invasive bladder cancer tissues, we found that lncRNA TINCR expression levels in TNM III/IV bladder cancer patients were higher than that in TNM I/II patients, and the expression levels of lncRNA TINCR were higher in high-grade tumor tissues; thus, we speculated that lncRNA TINCR was associated with the occurrence and development of bladder cancer. Chen et al. (2016) found that the expression of lncRNA TINCR was upregulated in bladder cancer tissues and cells, contributing to the occurrence and development of the tumor, consistent with the results of our study.
In this study, both SNP loci we selected are associated with bladder cancer risk. The bladder cancer susceptibility risk of the carriers with rs2288947 G allele was 2.32 times that of carriers with A allele, and the bladder cancer susceptibility risk of carriers with rs2288947 T allele was 0.33 times that of carriers with C allele. The minimum sample size of bladder cancer patients and the control group was 102 cases/102 cases and 103 cases/103 cases, respectively. One hundred twenty-five bladder cancer patients and 125 controls were involved in this study, indicating that the results of the study are objective and credible.
In addition, the stratified analysis of subjects' general clinical data indicated that only among patients who were <60 years old and were male, smokers, drinkers, having high-risk occupations, and with or without chronic bladder inflammation, the bladder cancer susceptibility risk of lncRNA TINCR rs2288947 dominant model carriers significantly rose, while only among those who were female, nondrinkers, and with chronic bladder inflammation, the bladder cancer susceptibility risk of lncRNA TINCR rs8113645 dominant model carriers had no significant change, which significantly changed in other stratification. The findings demonstrated that the association between SNPs of lncRNA TINCR rs2288947 and the bladder cancer susceptibility risk was related to factors of age, sex, smoking condition, drinking condition, and occupational exposures. The correlation between the SNPs of lncRNA TINCR gene rs8113645 and the susceptibility to bladder cancer was related to gender, drinking, and chronic bladder inflammation. In addition, the results of this study showed that rs2288947 G allele carriers had higher tumor grade. This also suggests that the combined effect of genetic factors and environmental factors determines the occurrence and development of bladder cancer.
We found that rs2288947 was located at the binding site of lncRNA TINCR and miR-1247-3p, and rs8113645 was located at the binding site of lncRNA TINCR and miR-30c-2-3p by means of bioinformatics. Considering the inconsistent binding efficiency of different alleles, it may occur that the lncRNA TINCR rs2288947 G allele is the target gene of miR-1247-3p, not the A allele, and the rs8113645 C allele is the target gene of miR-30c-2-3p, not the T allele. This speculation was also confirmed by dual-luciferase reporter assay.
We also found that the expression level of lncRNA TINCR was negatively correlated with that of miR-1247-3p and miR-30c-2-3p in bladder cancer tissues. Combined with the fact that the expression levels of miR-1247-3p and miR-30c-2-3p in cancer tissues were significantly lower than those in paracancer tissues, we proposed the hypothesis that the SNPs of rs2288947 and rs8113645 will affect the expression of lncRNA TINCR and further affect the lncRNA TINCR's function on the expression levels of its target microRNA molecules, namely miR-1247-3p and miR-30c-2-3p. However, how the changes in expression levels of lncRNA TINCR, miR-1247-3p, and miR-30c-2-3p lead to the occurrence and progression of bladder cancer remains undetermined and needs further study.
This study still has the following shortcomings, which require further research. First, considering the time limitation, we did not study the effects of these two SNP loci on the prognosis of bladder cancer patients. Second, we need to further study the changes in the expression levels of lncRNA TINCR, miR-1247-3p, and miR-30c-2-3p, and the molecular mechanisms underlying the occurrence and development of bladder cancer.
In conclusion, lncRNA TINCR SNPs rs2288947 and rs8113645 are associated with bladder cancer susceptibility. The expression levels of lncRNA TINCR with different alleles at SNP loci are significantly different, and further evidence of in vitro research is required to support its specific mechanism in the occurrence and development of bladder cancer.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from Zhejiang Provincial Medicine Health Science and Technology Program (2014ZQ015).