
Abstract
Background:
The Wnt/β catenin pathway promotes bone mineralization stimulating proliferation, differentiation, and survival of osteoblasts; it also inhibits osteoclast differentiation and osteocyte activity. Sclerostin (SOST) and Dickkopf 1 (DKK1) are Wnt/β catenin pathway inhibitors. Genetic variability in the expression of SOST and DKK1 might be involved in the development of postmenopausal osteoporosis (OP).
Aim:
To determine whether the SOST rs851056 and DKK1 rs1569198 polymorphisms are associated with OP in Mexican-Mestizo postmenopausal women.
Materials and Methods:
Two hundred and eighty Mexican-Mestizo postmenopausal women were assessed for their bone mineral density by dual-energy X-ray absorptiometry (DXA). Patients were classified as OP or non-OP. Genomic DNA was extracted from peripheral blood leukocytes. Genetic polymorphisms were analyzed by quantitative polymerase chain reaction using TaqMan probes.
Results:
The frequency of OP was 40% among the study population. Osteoporotic patients were older (p < 0.001), had a higher frequency of smoking (p = 0.01), and lower body mass index (p < 0.001) compared with the non-osteoporotic patients. The genotypic frequencies of the rs851056 locus of the SOST gene were GG 19%, GC 45%, and CC 35%, whereas the genotypic frequencies of the rs1569198 locus of the DKK1 gene were GG 15%, GA 40%, and AA 44%. In relation to rs851056 locus of the SOST gene, no differences were observed between the OP and non-OP cohorts in the frequencies of the GC polymorphism (48.7% vs. 43.1%). Similarly, analyses of the DKK1 rs1569198 does not demonstrate differences in the GA genotypic frequencies between the OP and non-OP cohorts (42.5% vs. 38.9%).
Conclusion:
Polymorphisms SOST rs851056 and DKK1 rs1569198 polymorphisms are not associated with OP in Mexican-Mestizo postmenopausal women.
Introduction
Osteoporosis (OP) is characterized by loss of bone mineral mass, leading to a deterioration of the bone microarchitecture and an increased risk of bone fractures (Cosman et al., 2014). Decreases in bone mineral mass are associated with a loss of balance between the bone formation mediated by osteoblasts and resorption by osteoclasts. The Wnt/β-catenin pathway plays a prominent role in this balance by regulating bone mineralization (Johnson and Kamel, 2007; Delgado-Calle et al., 2017). The Wnt/β-catenin pathway promotes proliferation, differentiation, and survival of osteoblasts while inhibiting osteoclast differentiation (Delgado-Calle et al., 2017). Two of the major inhibitors of the Wnt/β-catenin pathway are sclerostin (SOST) and Dickkopf 1 (DKK1) (Glinka et al., 1998; Semënov et al., 2005). SOST is a bone morphogenetic protein antagonist, which leads to inadequate bone formation. SOST is produced primarily by mature osteocytes from the SOST gene (Winkler et al., 2003). SOST interferes with bone mineralization through its binding to the low-density lipoprotein receptor-related protein 5/6 (LRP5/6), which antagonizes downstream Wnt/β-catenin signaling by blocking the stimulus for bone mineralization (Winkler et al., 2003; Li et al., 2005). In addition, SOST interferes with bone mineralization through interaction with low-density lipoprotein receptor related protein 4 (LRP4), which acts as a chaperone molecule for the inhibitory action of SOST on Wnt/β-catenin pathway (Krause et al., 2010; Leupin et al., 2011; Sharifi et al., 2015).
DKK represents a four-member family of glycoproteins, including DKK1, DKK2, DKK3, and DKK4. Mature osteoblasts and osteocytes predominantly express DKK1 (Monaghan et al., 1999). DKK1 has a direct effect on osteoclastogenesis through inhibition of the differentiation and maturation of osteoblast cells and increases the expression of the receptor activator of nuclear factor kappa-B ligand (RANKL) and osteoprotegerin (OPG) (Fujita and Janz, 2007).
Thus, it has been hypothesized that variants of SOST and DKK1 genes might affect the production, expression, and function of these proteins, modifying the risk of OP. Indeed, some studies have shown an association between SOST polymorphisms and bone mineral density (BMD) in postmenopausal women (Sims et al., 2008; Valero et al., 2011). However, Ock et al. reported no significant association between the rs851056 polymorphism of SOST and BMD in Korean postmenopausal women (Lee et al., 2014).
Other studies have also evaluated a possible association between several single nucleotide polymorphisms (SNPs) of DKK1 and BMD in postmenopausal women (Koromila et al., 2013; Wang et al., 2016; Martínez-Gil et al., 2018). Martinez-Gil et al. showed an association between rs1569198 and femoral neck BMD (Martínez-Gil et al., 2018). However, two other studies reported no associations between rs1569198 and the risk for lower BMD in Greek and Chinese populations (Koromila et al., 2013). Besides, there are other studies that analyze other polymorphisms in SOST and DKK1 genes (Ciubean et al., 2019; Wang et al., 2019).
In the Mexican postmenopausal population, the prevalence of OP varies from 13% to 40% (Delezé et al., 2000; Rojano-Mejía et al., 2011). Although genetic factors can be implicated in the risk of OP. To date, there are no studies in the Mexican population assessing whether the SNPs rs851056 of SOST and rs1569198 of DKK1 gene can contribute to the decrease in BMD. Therefore, the objective of this study was to evaluate the association between rs851056 SOST and rs1569198 DKK1 polymorphisms with OP in postmenopausal Mexican women.
Materials and Methods
Subjects and clinical setting
A case-control study was performed. The study population comprised Mexican-Mestizo postmenopausal women. Mexican-Mestizo is defined according to the Mexican National Institute of Anthropology and History (INAH) as “individuals who were born in Mexico, of the 3rd generation including their own and who were descendants of the original autochthonous inhabitants of the region and individuals who were mainly Spaniards” (Sanchez-Serrano, 1996).
The study patients were recruited at an outpatient research clinic, at the Experimental Therapeutics Institute in the University of Guadalajara, Guadalajara, Mexico. We included unrelated postmenopausal women (defined as the absence of any episodes of menstruation for at least 1 year, caused by a decrease in female sex hormones secondary to natural causes, excluding diseases or surgical menopause). Included patients were ≥45 years of age. We excluded patients with type 2 diabetes mellitus, hypothyroidism, chronic kidney disease, cancer, antecedents in the last year of use of medication interfering with bone metabolism, such as corticosteroids, selective estrogen receptor modulators, bisphosphonates, denosumab, or parathormone. Patients with hormone replacement therapy were allowed to participate and the data were included in the antecedents.
Clinical assessments
Four investigators (N.A.R.-J., E.D.R.-A, A.H.N.-Z., B.C.-H., and N.S.F.-R.) recorded the demographic data and epidemiological characteristics of the participants, which included information regarding risk factors for OP: age, smoking status, and duration of menopause. Also, lifestyle was recorded with regard to activity, specifically as whether participants had a sedentary lifestyle, defined as not performing any regular exercise of at least 30 min/day by 4 days/week (Kanis, 1994).
Body mass index (BMI) was calculated with the following formula: weight (kg)/height2 (m2). BMI was used to identify patients who were low weight (<18.5 kg/m2), normal weight (18.5-24.9 kg/m2), overweight (25-29.9 kg/m2), and obese (≥30 kg/m2) (Nuttall, 2015).
Bone densitometry measurements
BMD (g/cm2) of the lumbar spine (L1-L4) and total femoral neck were determined using dual-energy X-ray absorptiometry (DXA) with a Lunar Prodigy Advance densitometer (GE Medical Systems Lunar ver. 16. software; GE Medical Systems, Madison, WI) (M.L.V.-V., J.C.V.-J., J.M.P.-G., E.N.S.-R., and L.G.-L.).
BMD of the lumbar spine and total hip were classified according to the guidelines of the International Society for Clinical Densitometry (ISCD) [The International Society for Clinical Densitometry (ISCD), 2013] (Schousboe et al., 2013). These guidelines recommend that postmenopausal women be classified as having OP using T-scores when the results of lumbar spine or total hip show a decrement of ≤−2.5 standard deviations (SDs) from the norm. For the purposes of this study, we consolidated all BMD results into two groups: (1) OP group (case: T score in BMD ≤−2.5 SD) and (2) non-OP group (control: included osteopenia and normal BMD. T score >−2.5 SD) (Kanis, 1994).
Genotyping SOST and DKK-1 gene polymorphisms
Peripheral whole blood samples harvested in Vacutainer tubes containing ethylenediaminetetraacetic acid as an anticoagulant were collected from each patient. Genomic DNA was obtained from these blood samples using the modified Miller technique (Miller et al., 1988). Genomic DNA was quantified using a Nanodrop Genomic, DNAs were diluted in Tris-EDTA buffer to 20 ng/μL and placed in 200 μL propylene cryotubes (Eppendorf™). Genotyping SOST rs851056 and DKK1 rs1569198 polymorphisms was performed by quantitative polymerase chain reaction (qPCR) using TaqMan probes (Livak and Kenneth, 1999). Protocols for the Taqman ID were followed according to the manufacturer's instruction: C_11711720C_30 and C_11711720D_40 (Applied Biosystems); the StepOne™ Real-Time PCR system was employed for this purpose (Applied Biosystems) (I.N.B.-A., C.A.N.-V., A.V.-V., and M.-C.M.M.) (All results were independently scored by two blinded investigators (A.M.S.-C. and I.N.-A.). In the case of ambiguous results, the sample was analyzed a second time.
Determination of serum levels
Serum levels of SOST and Dickkopf were quantified by enzyme-linked immunosorbent assay (ELISA) using commercial kits: SOST (R&D Systems, Inc., 157 Minneapolis, MN. Sensitivity 0.37 pg/mL) and DKK-1 (R&D 156 Systems, Inc., Minneapolis, MN. Sensitivity 0.94 pg/mL), All procedures were performed according to the manufacturer's recommendations. All measurements were performed by the same researchers, who were blind to the clinical characteristics of the patients to avoid measurement biases.
Institutional review board
This study was approved by the ethics committee of the Hospital Civil “Dr Juan I. Menchaca,” Universidad de Guadalajara, Jalisco, Mexico, with registration number: HCG/CUCI/CI-0194/007/12. This study was conducted according to the principles expressed in the Helsinki Declaration (last revision Fortaleza, Brazil 2013). All study participants voluntarily provided written informed consent.
Statistical analyses
Qualitative variables are expressed as frequencies (%), whereas quantitative variables are indicated as the mean ± SD. We identified genotypic frequencies by direct counting. Allelic frequencies were determined by direct counting of the observed genotypic frequencies. Comparisons of means between the two groups was computed using the independent sample Student's t-test.
Comparisons between proportions were carried out using the chi-squared test (or the Fisher's exact test if required). Odds ratios (ORs) and their 95% confidence intervals (95% CIs) were calculated. A logistic regression analysis was performed to identify the variables associated with OP. We included, as covariates variables such as age, current tobacco consumption, menopause, BMI, and genotypes. The covariates included in the final model had p < 0.20 on univariate comparison or variables with biological plausibility to identify associated variables, excluding potential confounders. Kruskal-Wallis was performed to compare serum SOST and DKK1 levels between genotypes (E.E.P.-G. and L.G.-L.).
The Hardy-Weinberg equilibrium (HWE) for SOST rs851056 and DKK1 rs1569198 polymorphisms were evaluated in the groups and were determined by comparing the observed and expected data using the chi-squared test (A.M.S.-C. and I.N.-A.).
A p-value was considered significant at the p ≤ 0.05 level. Data were analyzed with SPSS version 23.0 Statistical software program (SPSS, Inc., NY), and OR and their 95% CI were obtained utilizing EPI INFO version 7.2 software (Epi Info™; Atlanta, GA).
Results
We evaluated 280 postmenopausal women. OP was observed in 113 (40%) of the postmenopausal women.
Table 1 presents the epidemiological characteristics of the postmenopausal women included. These patients had a mean age of 61 ± 8 years, and a mean duration of years since the onset menopause of 16 ± 9 years, 58% of patients had a sedentary lifestyle. Smoking was reported in 17% of subjects; current alcohol consumption was reported in 16% of subjects and 34% had normal or low weight, whereas the remaining 66% were overweight or obese.
Epidemiological Characteristics of Postmenopausal Patients
Qualitative variables were expressed in frequencies (%); quantitative variables were expressed as the means ± SDs; sedentary lifestyle was defined as not exercising for at least 30 min/day at least 4 days a week; non-OP was defined as normal BMD and osteopenia (T score ≥−2.5 SD).; OP (T score in BMD ≤−2.5 SD).
BMD, bone mineral density; BMI, body mass index; DKK1, Dickkopf 1; OP, osteoporosis; DXA, dual-energy X-ray absorptiometry; SD, standard deviation; SOST, sclerostin.
Genotypic distributions of SOST and DKK1 SNPs were in HWE (data not shown).
Table 2 shows the comparison of epidemiological and BMD characteristics between postmenopausal women with OP versus those without OP. Women with OP were older than non-OP (63 ± 8 vs. 59 ± 8, p < 0.001). Similarly, the group of women with OP had a higher duration of menopause (16 ± 10 years vs. 12 ± 8 years, p < 0.001), higher frequency of smoking (24% vs. 13%, p = 0.01), a lower BMI (25.5 ± 4 kg/m2 vs. 28.9 ± 5 kg/m2, p < 0.001), and a lower frequency of overweight and obesity (54% vs. 74%, p = 0.001) compared with the non-OP group. Interestingly, a lower proportion of sedentary lifestyle was observed in the OP group compared with the non-OP group (50% vs. 63%, p = 0.04). No other variables had significant differences.
Comparison of Epidemiological and Bone Mineral Densitometry Characteristics of Postmenopausal Women With Osteoporosis Versus Without Osteoporosis
Qualitative variables were expressed as frequencies (%); quantitative variables were expressed as means ± SDs. Comparisons between differences in proportions were performed with the chi-squared test (or Fisher's exact test if applicable). Comparisons between differences in means were performed with independent samples Student's t-tests; sedentary lifestyle was defined as not exercising for at least 30 min/day at least 4 days a week; non-OP was defined as normal BMD and osteopenia (T score ≥−2.5 SD); OP (T score in BMD ≤−2.5 SD).
Table 3 compares the genotypic and allelic frequencies of SOST rs851056 and DKK1 rs1569198 between the OP and non-OP groups. We observed a trend associating the absence of OP with the GG genotype at the rs851056 locus of the SOST gene; however, this trend did not achieve statistical significance (13.3% vs. 23.4%, p = 0.11). Similarly, there was a trend for the C allele compared with the G allele to be associated with OP (OR = 1.35, 95% CI: 0.96-1.91, p = 0.08). There were no significant differences between the frequencies of the GA genotype at the rs1569198 in the OP group compared with the non-OP group (42.5% vs. 38.9%, p = 0.69). An allele was observed at a similar frequency between the OP group and the non-OP group (65.5% vs. 63.7%, respectively, OR = 1.08, 95% CI: 0.76-1.53, p = 0.68).
Evaluation of rs851056 Polymorphism of SOST Gene and rs1569198 Polymorphism of DKK1 Gene and as Predictor of Osteoporosis Versus Nonosteoporosis in Postmenopausal Women
GG, wild homozygote; GC, heterozygote; CC, mutated homozygous for rs851056; GG, wild homozygote; GA, heterozygote; AA, mutated homozygous for rs1569198; qualitative variables were expressed in frequency (%).*p Values were obtained comparing OP versus non-OP.
95% CI: 95% confidence interval; OR, odds ratio.
Table 4 shows the risk factors associated with OP. In the final models, it is noted that age (OR = 1.06; 95% CI: 1.03-1.09, p < 0.001) and tobacco consumption (OR = 2.43; 95% CI: 1.25-4.74, p = 0.009) were considered a risk factor for OP in SOST. Also, age (OR = 1.08; 95% CI: 1.04-1.12, p < 0.001) and current tobacco consumption (OR = 2.24; 95% CI: 1.09-4.56, p = 0.02) were associated with a decrease in BMD for DKK1. We do not observe an association for risk of OP with the presence of any genotype of the SOST gene rs851056 polymorphism and DKK1 gene rs1569198 polymorphism.
Associated Factors with Osteoporosis
Multivariate analysis: logistic regression analysis; dependent variable: OP. Stepwise method *G/G; genotype used as referent for rs851056 SOST and *G/G genotype used as referent for rs1569198 DKK1.
Figure 1 shows the comparison of serum SOST and DKK1 levels between genotypes. In the comparison of rs851056 of SOST gene, the genotypes groups GG (n = 15), GC (n = 40) and CC (n = 15), nonsignificant differences in serum SOST levels were observed (p = 0.3). Whereas in the comparison of genotypes groups GG (n = 12), GA (n = 26) and AA (n = 32), of rs1569198 of DKK1 gene, no differences were observed in serum DKK1 levels (p = 0.4).
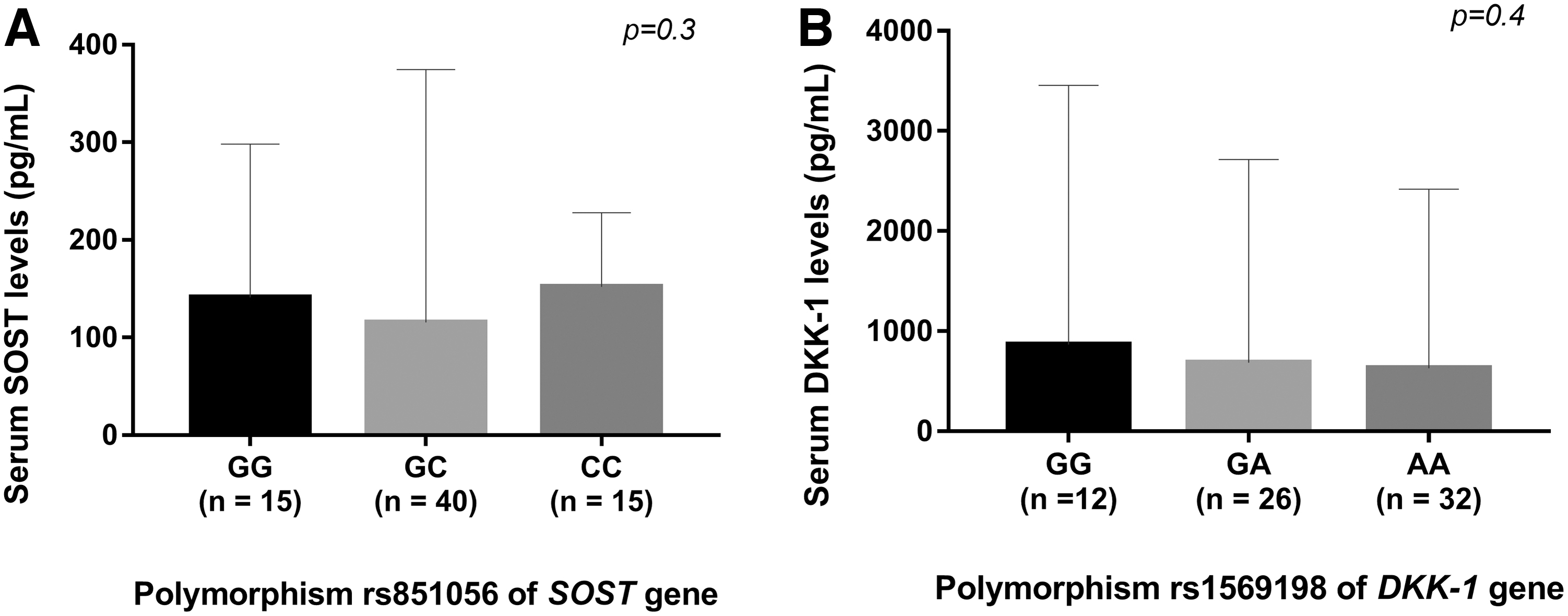
Comparison of serum SOST levels between genotypes of SNPs rs851056 of SOST gene and serum DKK1 levels between genotypes of rs1569198 of DKK1 gene.
Discussion
In this study of Mexican-Mestizo postmenopausal women, we identified a prevalence of the polymorphism GC of SOST gene of 45% and 40% of the GA polymorphism of DKK1 gene. For both genes, the heterozygous genotype was the most frequently observed in the Mexican-Mestizo population. We report the first allelic and genotypic frequencies in a Latin American country for the rs851056 polymorphism of the SOST gene nor rs1569198 of the DKK1 gene, neither of which was confirmed to confer a risk of OP in this population.
SOST is a protein secreted by osteocytes that acts as an antagonist to the Wnt/β-catenin pathway. SOST can bind to the Wnt/β-catenin co-receptors LRP5/6, causing downstream regulation. In addition, SOST can interact with LRP4 as a molecule chaperone for the inhibition of Wnt/β-catenin signaling (Li et al., 2005; Leupin et al., 2011).
Moreover, it has been reported in animal models that overexpression of SOST increases RANKL expression in bone (Tu et al., 2012). Several genetic variants of the SOST gene have been reported. One of them, the rs851056 G > C polymorphism of SOST, has been associated with low SOST levels, favoring bone resorption in some populations. This SNP of the SOST gene is located at the −1073 locus of the promoter close to the transcriptional factor motifs starting site, which causes an increase in gene expression related to delaying bone remodeling. This change has been hypothesized to alter the expression and serum levels of SOST, influencing bone remodeling (Pérez-Campo et al., 2017). In this study, we did not identify an association between SOST rs851056 polymorphism and OP in the Mexican population.
Our results differ from the observations of other populations. Sims et al. (2008), in Australian postmenopausal women, reported an association between SOST rs851056 and an increase in the risk of low BMD (Sims et al., 2008). Yerges, in a Caucasian population of the United States found that a polymorphism of SOST is related to decreased mineral density in the femoral neck and lumbar spine in older men (Yerges et al., 2009). Contrarious to these two authors, Valero et al. (2011) in two cohorts of Spanish women from the provinces of Cantabria and Valencia found that the wild-type genotype GG had significantly lower BMD compared with the other genotypes, including the heterozygote.
These inconsistent results could be derived from differences in population selection, ethnicity, and other factors related to OP, such as age.
DKK1 is a protein that has a direct effect on osteoclastogenesis by either decreasing the expression of RANKL or increasing the expression of OPG (Glass et al., 2005; Spencer et al., 2006). Inhibiting DKK1 could promote osteoblast differentiation and bone formation, protecting against systemic bone loss (Yaccoby et al., 2007). In one study, a deletion of a DKK1 allele was associated with increased bone mineral and bone mass (Morvan et al., 2006).
The DKK1 rs1569198 G > A polymorphism is located in intron 3 in proximity to exon 4. Exon 4 encodes the C-terminal cysteine-rich domain of DKK1, which is reported to have the highest binding affinity to the relevant domain of LRP5 (Chen et al., 2008; Beauregard et al., 2013).
We did not identify an association between OP and any of the alleles or genotypes of the DKK1 rs1569198. Our findings are supported by two previous studies; Koromila et al. and Wang et al. did not observe any association between BMD and the DKK1 rs1569198 polymorphism in postmenopausal women in two independent studies (Koromila et al., 2013; Wang et al., 2016).
This exploratory study had several limitations that must be taken into account. This study might reflect only the genetic characteristics of patients with OP from the Western population of Mexico. Also, we only analyzed one polymorphic site for each gene. Other polymorphic sites could be implicated in the development of OP. Further studies should include genetic expressions associated with these genotypes as well as the influence from other factors, such as interactions between diverse genetic variations. Linkage disequilibrium (LD) within other SNPs should be analyzed.
Conclusion
To the best of our knowledge, this is the first study performed in Mexican-Mestizo postmenopausal women suffering from OP that evaluates the association between SOST rs851056 and DKK1 rs1569198 polymorphisms. As OP is a complex disease influenced by multiple factors, the influences of DKK1 and SOST polymorphisms on BMD need to be confirmed in prospective cohort studies with larger sample sizes.
Footnotes
Author's Contributions
M.L.V.-V., N.A.R.-J., B.C.-H., E.D.R.-A., C.A.N.-V., J.M.P.-G., N.S.F.-R., and A.H.N.-Z. were in charge of investigation, conceptualization, original draft, review, and editing. Conceptualization, investigation, resources, review and editing, and supervision by J.C.V.-J. Validation, resources, review and editing, and supervision by M.C.M.-M. and I.N.-A. Investigation and data curation by E.N.S.-R., A.V.-V., and I.N.B.-A. Formal analysis, data curation, original draft, review and editing, visualization, and supervision by E.E.P.-G. Investigation, original draft, review, and editing by L.G.-L. Conceptualization, methodology, investigation, resources, original draft, review and editing, supervision, and project administration by A.M.S.-C.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.