
Abstract
Aim:
Circulating microRNA-21 (miR-21) has been utilized as a diagnostic tool in the assessment of heart failure (HF). Blood constitution may be altered when HF occurs and miR-21 may affect hematopoiesis. Sample hemolysis may influence the determination of circulating miRNAs, challenging the diagnostic use of miRNAs.
Methods:
We examined the relationship between blood measurements and miR-21 levels in ambulant chronic HF patients with reduced ejection fraction (HFrEF; n = 19). Healthy volunteers (n = 11) served as controls. Serum miR-21 levels were measured through quantitative reverse transcription polymerase chain reaction (RT-qPCR) and we calculated the hemolysis score (H-score). The study was approved by our Institutional Review Board (EK FaF UK 02/2018).
Results:
MiR-21 serum levels were reduced in HFrEF patients compared with the controls (p < 0.05), without relationship to New York Heart Association class, left ventricular ejection fraction, or N-terminal prohormone of brain natriuretic peptide levels. MiR-21 levels decreased markedly in anemic patients, compared with those with normal hematocrits (p < 0.05). We found a significant relationship between miR-21 to hematocrit (p < 0.05) and hemoglobin concentration (p < 0.05). Importantly, we found a correlation between hematocrit and sample H-score (p < 0.05) in the cohort of HFrEF patients; however, there was no correlation between hemolysis and miR-21.
Conclusion:
Circulating miR-21 levels were decreased in HFrEF patients and hematocrit was identified as a factor associated with this abnormality. This suggests that miR-21 mirrors other characteristics of HFrEF patients rather than the standard identifiers of HF severity and progression.
Introduction
MicroRNAs, small noncoding RNA molecules regulating gene expression at the post-transcriptional level, are potent modulators of cardiac remodeling in heart failure (HF) (Thum et al., 2008; Doka et al., 2017; Napoli et al., 2020; Kura et al., 2020). Multiple circulating miRNAs have been described as candidates for diagnostic biomarkers (Huang et al., 2019); among them, miR-21 has been suggested as a top candidate when studying HF (Thum et al., 2008).
Anemia, a condition contributing to advanced HF, is viewed as a risk marker for identifying individuals who are more likely to experience a progressive degradation of their overall health status (Savarese et al., 2020). The reason why this occurs is largely unknown; however, miRNA-21 may be involved, as it affects hematopoiesis (Bhagat et al., 2013) perhaps serving as a mechanistic link between anemia and HF. The aim of this study was to study the relationship between serum miR-21 concentrations and anemia in patients suffering from HF with reduced ejection fraction (HFrEF).
Methods
Study participants
Ambulatory patients diagnosed with chronic HF (ICD-10 code I50) were examined at the outpatient clinic of St. Michael's Hospital in Bratislava, Slovak Republic. Inclusion criteria at the time of initial assessment were (1) present symptoms and signs of HF, (2) left ventricular ejection fraction (LVEF) <35%, and (3) serum N-terminal prohormone of brain natriuretic peptide (NT-proBNP) >125 pg/mL. After the initial assessment, patients were comprehensively treated for HF and routinely examined at the clinic for at least 3-year follow-up period until year 2017. After observation period, patients underwent endpoint examination, which consisted of echocardiography, blood sampling for blood count, and biochemistry including NT-proBNP and miR-21 analysis. Control group consisted of apparently healthy volunteers (hereinafter controls) with the following exclusion criteria: (1) diagnosis of any cardiovascular or other chronic disease and (2) current pharmacological treatment. Controls were not eligible for unnecessary HF examination. At the end of study (year 2017), each volunteer provided blood sample for miR-21 analysis. The study was approved by Ethics Committee of the Faculty of Pharmacy, Comenius University in Bratislava (EK FaF UK 02/2018). Each participant provided written informed consent.
Blood samples
Blood samples were taken between 7:00 and 8:00 a.m. after overnight fasting. Standard laboratory examinations, including analyses of NT-proBNP levels and blood count were performed. We defined hematocrits of <38% in females and <41% in males as mild-moderate anemia (Androne et al., 2003).
Determination of miRNA-21levels
For the analyses of miR-21 levels, additional venous blood samples were collected. For details of collection and storage, see Supplementary Appendix SA1. The relative abundance of miRNA-21 in blood serum was determined through quantitative reverse transcription polymerase chain reaction (RT-qPCR). The detailed procedure is described in Supplementary Appendix SA1. RNA was extracted from 50 μL of serum and used for a multiplex reverse transcription protocol with the TaqMan MicroRNA Reverse Transcription Kit and a primer pool of TaqMan MicroRNA assays for hsa-miR-21 and cel-miR-39. Finally, TaqMan™ Universal Master Mix II, with uracil-N-glycosylase (Applied Biosystems) was used for the qPCR. Mean PCR efficiency estimates per amplicon and quantification cycle (Cq) for each sample were determined from the raw data using LinRegPCR software (version 2018.0; Ruijter et al., 2009). The synthetic cel-miR-39 was added as an external miRNA to verify the interindividual variability among samples and to normalize the results of miRNA-21 levels in the final calculation using Pfaffl-like efficiency corrected relative abundance (Pfaffl, 2001). Addition of this external synthetic spike-in miRNA to the serum samples allowed us to evaluate the interindividual variability of the entire process and thus normalize possible variances arising from minor procedural differences between samples (Mitchell et al., 2008).
H-score calculation
Hematocrit levels may influence the extent of hemolysis and consequently may have an impact on microRNA concentrations (Kirschner et al., 2013; Mayr et al., 2017). For this purpose, we measured the absorbance values of serum samples at λ = 414 nm (oxyhemoglobin absorbance peak) and λ = 385 nm (“background” absorbance) using a NanoDrop® ND-1000 (Thermo Fisher Scientific). These values were used to calculate the lipemia-independent hemolysis score (H-score) according to (Appierto et al., 2014).
Statistical analyses
A Shapiro-Wilk test was used as a normality test. For normally distributed data, we performed a Student's t-test. For the non-normally distributed data, we performed a Mann-Whitney U test. Categorical data were tested using “N-1” chi-squared test. Statistical correlations between the two subject groups were determined by Pearson's (for bivariate normal distributed data) or Spearman's (for non-normally distributed data) correlation coefficients. All data were handled by GraphPad Prism (version 6; GraphPad Software, Inc., San Diego, CA). An adjusted (by Benjamini-Hochberg procedure for multiple comparisons) p-value <0.05 was considered statistically significant.
A receiver operating characteristic (ROC) curve was used to illustrate the diagnostic ability of miR-21 in serum to discriminate healthy volunteers and HF patients (for details see Supplementary Appendix SA1 and Supplementary Fig. S4).
Results
Basic clinical features of study participants are presented in Table 1 (additional information are in Supplementary Fig. S1 and Supplementary Table S1). Patients with HFrEF were divided in two subgroups—normal and mild-to-moderate anemia defined by hematocrit cutoff values <38% for women and <41% for men. Significant differences were observed only in anemia-related parameters—hematocrit, red blood cell count, and hemoglobin.
Characteristics of Patients at Endpoint Examination
Results are expressed as arithmetic mean.
Indicates statistical difference between anemic and nonanemic subjects (adj. p < 0.05).
Adj. p-value, adjusted for multiple comparison by Benjamini-Hochberg procedure; BP, blood pressure; HF, heart failure; IQR, interquartile range (25th-75th percentile); LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; N, number of subjects; NT-proBNP, N-terminal prohormone of brain natriuretic peptide; RVEDD, right ventricular end-diastolic diameter; ±SD, sample standard deviation.
We observed significantly reduced relative levels of circulating miR-21 when compared with healthy volunteers (p < 0.05; Fig. 1A), with a lack of significant relationship to relevant diagnostic features of HFrEF—LVEF and NT-proBNP (for details see Supplementary Fig. S2). However, HFrEF patients exhibited a significant correlation of their circulating miR-21 levels with their hematocrits (Pearson r = 0.5539; p < 0.05) as well as with their hemoglobin levels (Pearson r = 0.5202; p < 0.05) yet not with other blood count parameters (for details see Supplementary Fig. S3).
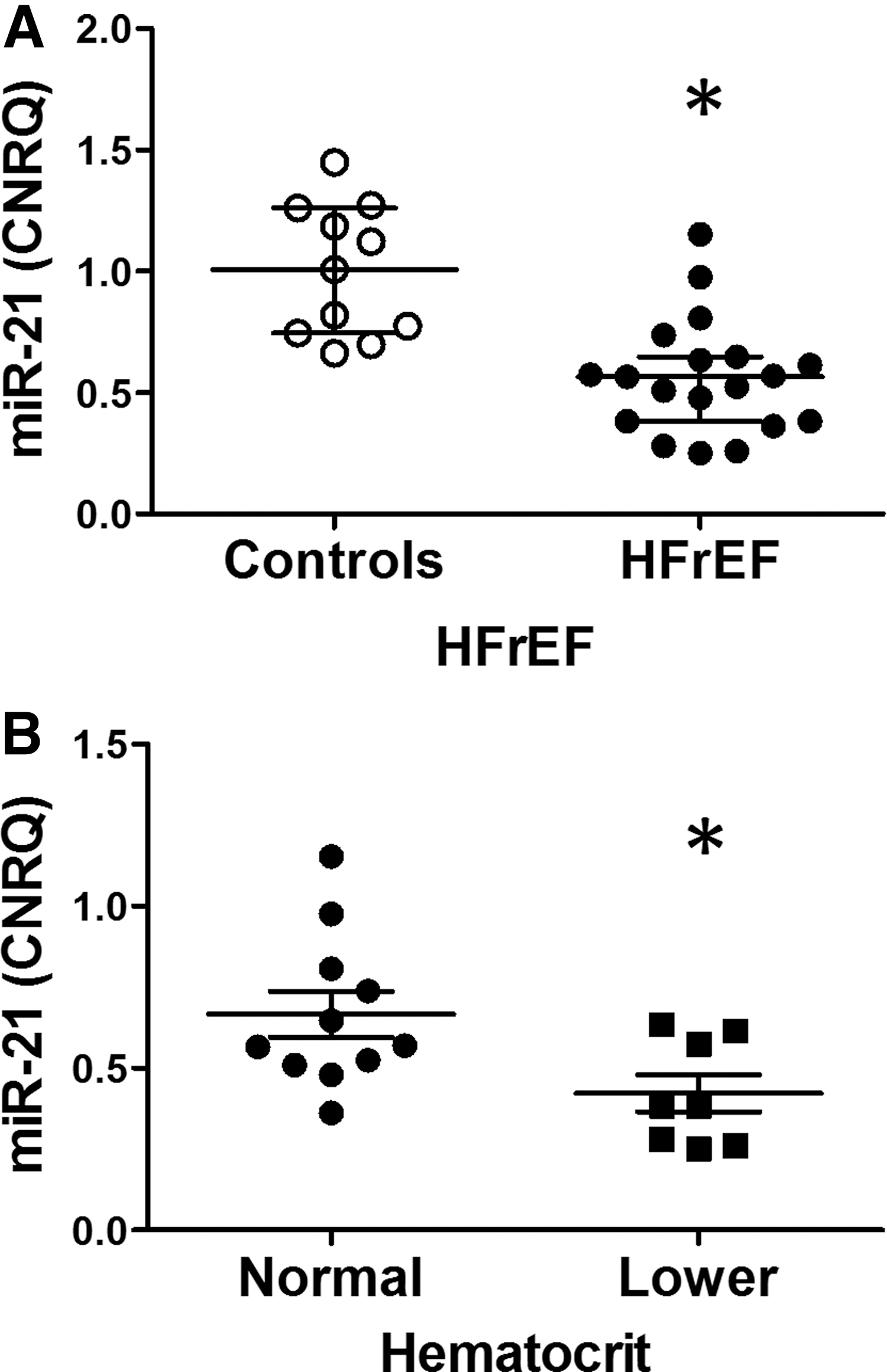
When dividing the cohort of HFrEF patients according to hematocrit, we found significantly lower circulating miR-21 levels in the group with lower hematocrits (Fig. 1B). Importantly, when evaluating the entire HFrEF cohort, hematocrit did not correlate with any of the analyzed measurements except for a significant negative correlation with the laboratory measurement of HF severity, that is, NT-proBNP (Spearman r = −0.5585; p < 0.05). In addition, anemic HFrEF patients had significantly higher NT-proBNP concentrations (by 338% on average, p < 0.05).
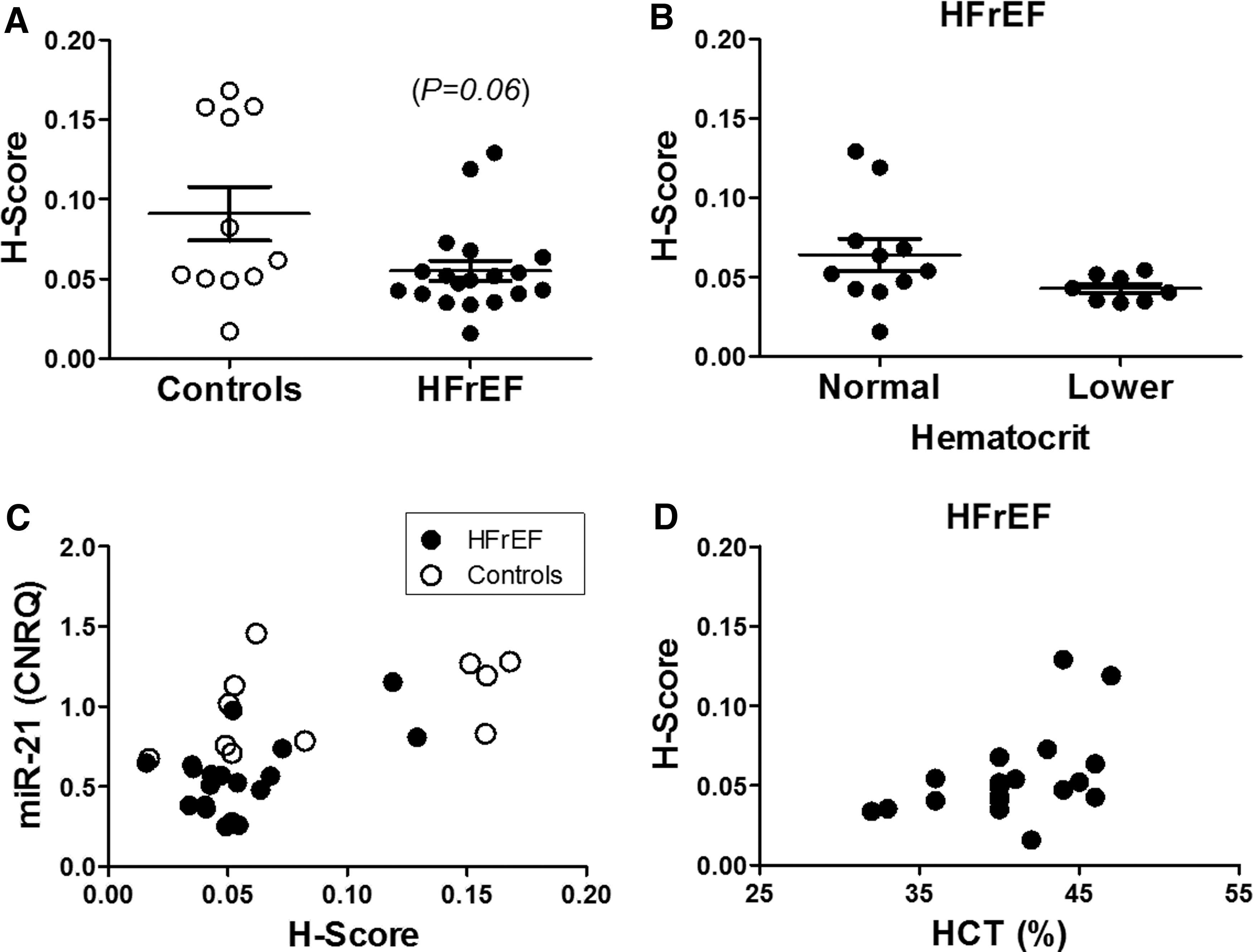
We observed a nonsignificant tendency toward a lower H-score in the controls when compared with HFrEF patient samples (Fig. 2A). The difference between HFrEF patients with anemia as compared with those with normal hematocrits was even less pronounced (Fig. 2B), although HFrEF patients exhibited a significant relationship between hematocrit level and H-score (Fig. 2D). We also observed a significant correlation between H-score and miR-21 levels in the controls but not in for the HFrEF cohort (Fig. 2C).
ROC analysis (for details see Supplementary Fig. S4) indicated excellent diagnostic accuracy for serum miR-21 levels (AUC: 91.4%; 95% confidence interval: 82.5-100) to distinguish between healthy volunteers and HFrEF patients.
Discussion
MiR-21 is of particular interest for use in HF diagnostics (Huang et al., 2019); however, its utility is still uncertain. Mir-21's upregulation during the cardiac tissue remodeling process is well known (Thum et al., 2008), but the concomitant rise of its circulatory form in HF is likely not as inevitable as suggested. Similarly, a significant downregulation of serum miR-21 was documented in hypertensive patients with symptomatic HF (Tomaniak et al., 2018). Moreover, additional cardiovascular complications contribute to a confusing picture. Atherosclerosis increases (Tsai et al., 2013) the presence of atrial fibrillation rather than decreasing circulating miR-21 (Sieweke et al., 2020). These controversies likely mirror paradoxical properties of miR-21's role in the heart, where cardiac repair and beneficial protection of cardiomyocytes (Luther et al., 2018) may be overwhelmed by negative consequences of its antiapoptotic action in fibroblasts boosting cardiac fibrosis (Dong et al., 2014). From this perspective and being in line with observations that miR-21 mediates cardioprotection (Luther et al., 2018), the reduction of miR-21 levels suggests a rather unfavorable long-term outcome.
Other explanations for confounding miR-21 findings from various clinical observations may be related to differences in sample quality, and the methods used for analysis (Meyer et al., 2010). In particular, hematocrit levels may influence the extent of hemolysis (Mayr et al., 2017). Consequently, these variables may have an impact on miR-21 concentrations (Kirschner et al., 2013), as was confirmed in this study. Other explanations may include variations in the clinical features of the participants included in the different studies (e.g., gender, age, pharmacotherapy, and disease duration).
Interestingly, decreased erythrocyte-related measures (hematocrit and hemoglobin) were the only abnormalities correlated with suppressed circulatory miR-21 levels in HFrEF patients. Although not significantly related to red blood cell counts, some association between miR-21 and erythrocytes is conceivable. MiR-21 has been documented to suppress erythropoiesis in bone marrow (Bhagat et al., 2013) and to regulate neocytolysis after hypoxic conditions (Song et al., 2017). The lowered circulating miR-21 levels in anemic individuals herein reported is a novel finding and sheds additional light on the link between anemia and HF.
This study has certain limitations. First, we are unable to provide a more detailed characterization of blood samples, yet hematocrit is one of the standard parameters used in diagnostics of anemia (Androne et al., 2003). Second, determination of serum miR-21 levels is challenging, but RT-qPCR remains the primary method for quantitation despite its known limitations. Currently, there is no consensus on how to normalize RT-qPCR results, and the choice of normalization method could represent an important bias (Meyer et al., 2010).
Conclusion
Our findings suggest that miR-21 levels mirror other characteristics of patients with HFrEF rather than standard identifiers of HF severity and progression (LVEF, NT-proBNP). We documented associations of miR-21 levels to hematocrit as well as to hemoglobin, suggesting a role in modulating HFrEF-related anemia. Despite the limited sample size, our observations challenge the use of miR-21 in assessing HF, as well as the hypothesis that there is an inverse relationship between miR-21 levels and erythropoiesis, at least in HFrEF. In addition, our findings also highlight the importance of solving the technical aspects of analysis before introducing miR-21 in HF diagnostics.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.