
Abstract
Objective:
Caspase-3 activation is central to apoptosis and is involved in periodontal disease pathogenesis. Thus, CASP3 gene polymorphisms in a population may influence the severity of periodontal disease. In this study we examined the association of the CASP3 rs4647602 alleles and genotypes with periodontitis using cohorts of periodontally diseased and healthy South Indian subjects of Tamil ethnicity.
Materials and Methods:
Allele specific polymerase chain reaction genotyping were performed to identify CASP3 rs4647602 gene polymorphism in 145 periodontally healthy subjects and 145 periodontitis patients. The associations between gene polymorphism frequencies and the risk of periodontitis were analyzed by the Pearson chi-square test, the Mann Whitney U test, t test, logistic regression and assessed by odds ratio (ORs) and 95% confidence interval (95% CIs).
Results:
The statistical test results demonstrated a significant difference in genotype distribution between the two groups (p < 0.001) with the variant GG genotype associated with a significantly increased risk for periodontitis (OR = 3.55, 95% CI = 1.89-6.68, p < 0.001). Furthermore, all clinical parameters were highly significantly correlated with the genotypes in periodontitis subjects (p < 0.05).
Conclusion:
The present study suggests that the rs4647602 GG genotype of CASP3 is associated with the increased periodontitis risk in South Indians of Tamil ethnicity.
Clinical Trial Registration Number
: (CTRI/2021/03/032412).
Introduction
Periodontal disease is caused by interplay between pathogens present in biofilm and the resultant inflammatory response, which is mediated by neutrophils, macrophages, and lymphocytes (Hajishengallis et al., 2012). The transition from commensal bacteria to pathogenic microbiota, also known as dysbiosis, produces “microbial shift” over time, resulting in oral dysbiosis, which transforms the symbiotic host-microbe interaction to a pathogenic condition. This dysbiosis in the subgingival biofilm could be the initiator for the periodontal disease. Furthermore, the immune inflammatory response in periodontal disease is not only microbial in origin but is also influenced by host-derived factors, such as systemic inflammatory burden, risk factors, such as diabetes and genetics (Van Dyke and Dave, 2005).
Genes are implicated in the progression of the disease and in determining the associated risks (Kinane et al., 1999). Despite common etiological, behavioral, and environmental factors, individuals exhibit differential susceptibility to the disease and this attributes to a genetic variance (Sofaer, 1990; Hodge and Michalowicz, 2001). Genes varying in their nucleotide sequences are referred to as alleles and prevalence of such alleles in at least 1% of the population is known as gene polymorphism (Nielsen, 2004). Single nucleotide polymorphisms (SNPs) within genes may be associated with alterations in protein expression, structure, and function. These, in turn, may lead to a phenotypic variation (Cantor and Nelson, 2005). The majority of periodontitis genetic research is focused on gene polymorphisms, such as cytokines, cell surface receptors, chemokines, enzymes, and other polymorphisms associated with antigen recognition that influence immunoregulation or metabolism (Laine et al., 2010). Studies have reported genetic factors to account for half of the variations seen in periodontal disease manifestation in humans (Michalowicz et al., 1991, 2000; Michalowicz, 1994).
Caspases are cysteine proteases that are involved in apoptosis, necrosis, and inflammation (Lozano et al., 2009). Caspases are subcategorized into initiator caspases, executioner caspases, and inflammatory caspases (Fan et al., 2005; Singh, 2007). Initiator caspases (2, 8, and 9) initiate the apoptosis signal while executioner caspases (3, 6, and 7) degrade into cellular components to induce morphological changes (Riedl and Shi, 2004). Inflammatory caspases (1, 4, 5, 11, 12, 13, and 14) are involved in inflammatory cytokine signaling and thereby contribute to apoptosis indirectly (Fernández and Lamkanfi, 2015).
Caspase-3 (CASP3) is a key executioner caspase that regulates a variety of important cellular substrates, and it can be easily identified in cells undergoing apoptosis when active (Wu et al., 2019). CASP3 is active in both acidic and basic pH when compared with other executioner caspases like Caspases 6 and 7 (Stennicke and Salvesen, 1998). CASP3 is known as executioner enzyme because it is activated by both intrinsic and extrinsic pathways.
CASP3 levels were found to be elevated in periodontitis and CASP3 may serve as a biomarker for periodontal disease and its progression (Pradeep et al., 2016; Shoukheba, 2016; Loka et al., 2021).
Caspase-3 is encoded by CASP3 gene and elevated Caspase-3 gene expression was observed in immunohistochemistry studies in gingival tissue samples with periodontitis. It was suggested that CASP3 gene might be involved in the inflammatory process associated with periodontitis (Gamonal et al., 2001; Bantel et al., 2005; Gonzalez et al., 2011).
CASP3 gene polymorphism was studied among South Koreans, wherein genome-wide human assay analysis was performed and 201 SNPs of CASP3 were identified, out of which only three genotypes, that is, rs12108497, rs4647602, and rs113420705, were significantly associated with periodontitis. However, rs4647602 genotype was highly significant with periodontitis (Kang et al., 2015). Evaluating CASP3 gene polymorphisms in various ethnic groups with periodontitis will help to understand the exact role of CASP3 gene in periodontal disease pathogenesis. The objective of investigating gene SNPs in such circumstances is to find the possible indicators of susceptibility, severity, and clinical outcome (Barton and John, 2003; Villar et al., 2004). Therefore, the present study aims to determine the association of CASP3 (rs4647602) gene polymorphism with periodontitis in South Indians of Tamil ethnicity.
Materials and Methods
Study subjects and ethics clearance
Ethics clearance was given by the Institutional Review Board of SRM University, Ramapuram, Chennai (SRMDC/IRB/2019/MDS/NO.504). A total of 290 ethnic Tamil individuals were recruited from the outpatient clinic of SRM Dental College and Hospital, Ramapuram, Chennai, through convenience sampling. The study period for the recruitment of individuals and sample collection was from September 2020 to October 2021, all the subjects were explained about the study, and written informed consents were obtained. The current study design was a cross-sectional observational epidemiological study.
A customized case sheet was prepared for clinical evaluation of each subject based on their demographic details, socioeconomic status, and ethnicity, which included questions regarding whether patient was thoroughly Tamil lineage and whether they were residing in Tamil Nadu.
Tamil ethnic individuals of both genders between 18 and 60 years of age were recruited and categorized into two groups. Group I (Control group) comprised 145 systemically and periodontally healthy subjects, with probing pocket depth (PPD) ≤3 mm, no clinical attachment loss (CAL = 0), with the presence of local factors, and <10% of sites with bleeding on probing (BOP). Group II comprised 145 subjects with periodontitis. Diagnosis of periodontitis was based on the 2018 American Academy of Periodontology (AAP) (Papapanou et al., 2018) classification. The criteria for periodontitis were stage II, III, and IV with grade A. Stage II chronic periodontitis is defined as a CAL of 3-4 mm with a pocket depth of 5 mm and no tooth loss; stage III and IV chronic periodontitis is defined as a CAL of 5 mm with 4 or 5 tooth loss and a pocket depth of 6 mm, as well as furcation involvement of posterior teeth.
This study excluded patients with diabetes mellitus and diabetic complications, and pregnant and breastfeeding women, smokers, and those that use smokeless tobacco were also excluded. Since smoking and diabetes are considered as confounding variables for the study, these subjects were excluded from the study. Subjects who had undergone periodontal treatment in the previous 6 months, had taken antibiotics, immunosuppressants, or anti-inflammatory medicines in the previous three months, or had a prophylactic requirement for antibiotics before probing or any periodontal therapy were excluded from the research.
Oral examination was done to assess the clinical parameters, including plaque index (PI) (Silness and Loe, 1964), modified sulcus bleeding index (MSBI) (Mombelli et al., 1987), PPD, and CAL from all the subjects. University of North Carolina 15 probe (UNC-15 [Hu-Friedy]) probe was used to assess the periodontal clinical parameters and all the clinical parameters were recorded by a single calibrated Periodontist (D.P.). The intraclass correlation coefficient (ICC) was calculated for both intra- and interobserver reliability and it was presented with 95% confidence interval (95% CI) (p < 0.05) (ICC 0.82, CI: 0.74-0.89).
According to the STROBE checklist of observational studies, the study fulfilled all 22 criteria and the information for each criterion was presented clearly. Details regarding study design, participants, statistical design, results, and statistical design were clearly stated in the study.
Following which, 2 mL of venous blood was collected from the antecubital fossa using a 5-mL syringe from all the subjects. The extracted blood was immediately transferred into ethylenediamine tetraacetic acid-coated vacutainer and stored at −80°C in a deep freezer.
Genomic DNA extraction
The genomic DNA was extracted from the blood samples using the following protocol: 0.1 mL of peripheral blood was lysed in 100 μL of cell lysis buffer containing 36-50% guanidine hydrochloride (Nucleospin Blood DNA Kit; Machery Nagel, Germany) and incubated at 57°C for 2 h to enable complete lysis of leucocytes (Christopher et al., 2021).
Following lysis, an equal volume of 100% ethanol was added to precipitate the genomic DNA. Subsequently, the entire content was transferred to DNA spin columns containing silica membrane and centrifuged at 8000 revolutions per minute (rpm) for 1 min at room temperature. The silica columns were then washed twice with wash buffer (Machery Nagel). Degraded proteins and membrane lipid particles were washed off during the wash cycles. DNA captured from the silica membrane was eluted with 50 μL of elution buffer (Machery Nagel) after the two wash processes. The quality of DNA was examined by running a 2 μL aliquot of the stock in a 0.8% agarose gel. The concentration was determined by analyzing 1 μL of the sample in a fluorescence-based DNA quantifier (Qubit, Austria).
Allele polymerase chain reaction for CASP3 rs4647602 SNP
Nucleotide sequence and location of rs4647602 SNP in intron 1 of CASP3 gene are shown in Figure 1.
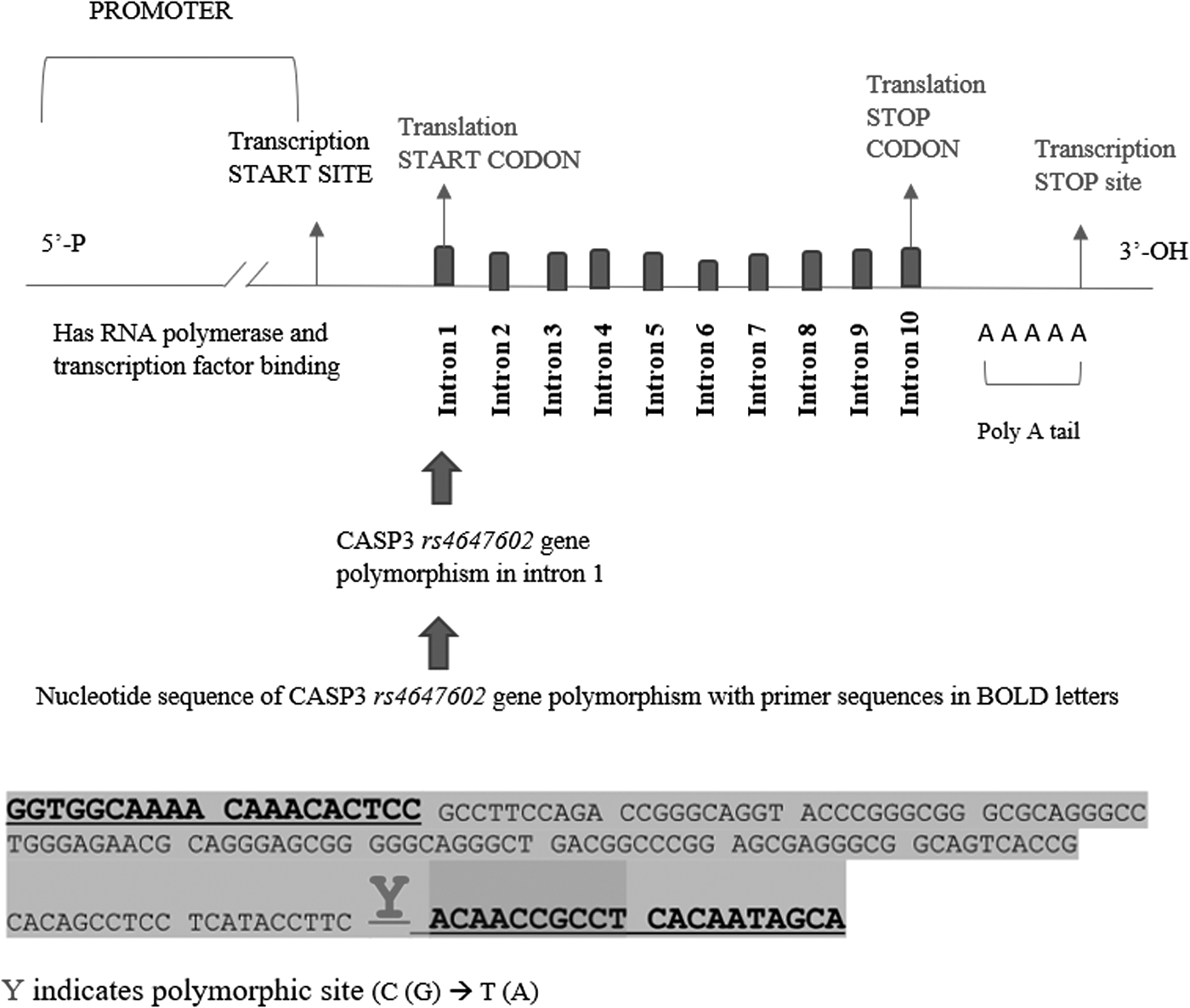
Nucleotide sequence and location of rs4647602 SNP in intron 1 of CASP3 gene. SNP, single nucleotide polymorphism.
The common forward primers used in the study were:
1. “GGTGGCAAAACAAACACTCC” and
2. “TGCTATTGTGAGGCGGTTGT
Polymerase chain reaction (PCR) was performed on 50 ng of DNA samples with Emerald Amp GT PCR Taq Master mix (Clontech-TaKaRa, Japan) in TaKaRa thermal cycler. The PCR amplification was started at 94°C for 5 min, followed by denaturation for 35 cycles at 94°C for 30 s. The annealing phase was carried out at 60°C for 60 s. The primer extension was done at 72°C for 60 s, followed by final primer extension for 5 min at 72°C. Agarose gel electrophoresis was conducted to confirm the specificity of primers and DNA bands were captured with gel documentation unit (UV range 302 and 364 nm).
Optimized conditions of allele-specific PCR were used to analyze all periodontitis samples and normal controls through allele-specific real-time PCR using the aforementioned set of primers and PCR conditions. The amplification reactions were performed in the presence of BRYT green real-time PCR master mix (Cat. No. A6001; Promega Corporation, Madison, USA). Primers were synthesized at Bioserve Biotechnologies, Hyderabad (Telangana, India). The amplification reactions were performed in a rotor-gene Q real-time PCR system (Qiagen, Germany). Following amplification, the fluorescence values were normalized with the RGQ software and amplification curves were analyzed.
To optimize the specificity of allele-specific PCR primers in the detection of the “A” or “G” alleles in the samples, DNA samples extracted from positive controls of the alleles (obtained from in-house-developed control samples) were amplified with primers under the conditions described in the aforementioned methodology. The PCR products thus obtained were subjected to agarose gel electrophoresis in a 1.5% gel. Subsequently, the gel was visualized in a gel documentation unit. Data analysis indicated the presence of allele-specific PCR products with each of the allele-specific primers.
PCR products seen in test sample 1 and 6 indicated the presence of AG heterozygous alleles; PCR products seen in test samples 2 and 4 indicated the presence of GG homozygous alleles; PCR products in test samples 3 and 5 indicated the presence of AA homozygous alleles (Fig. 2).
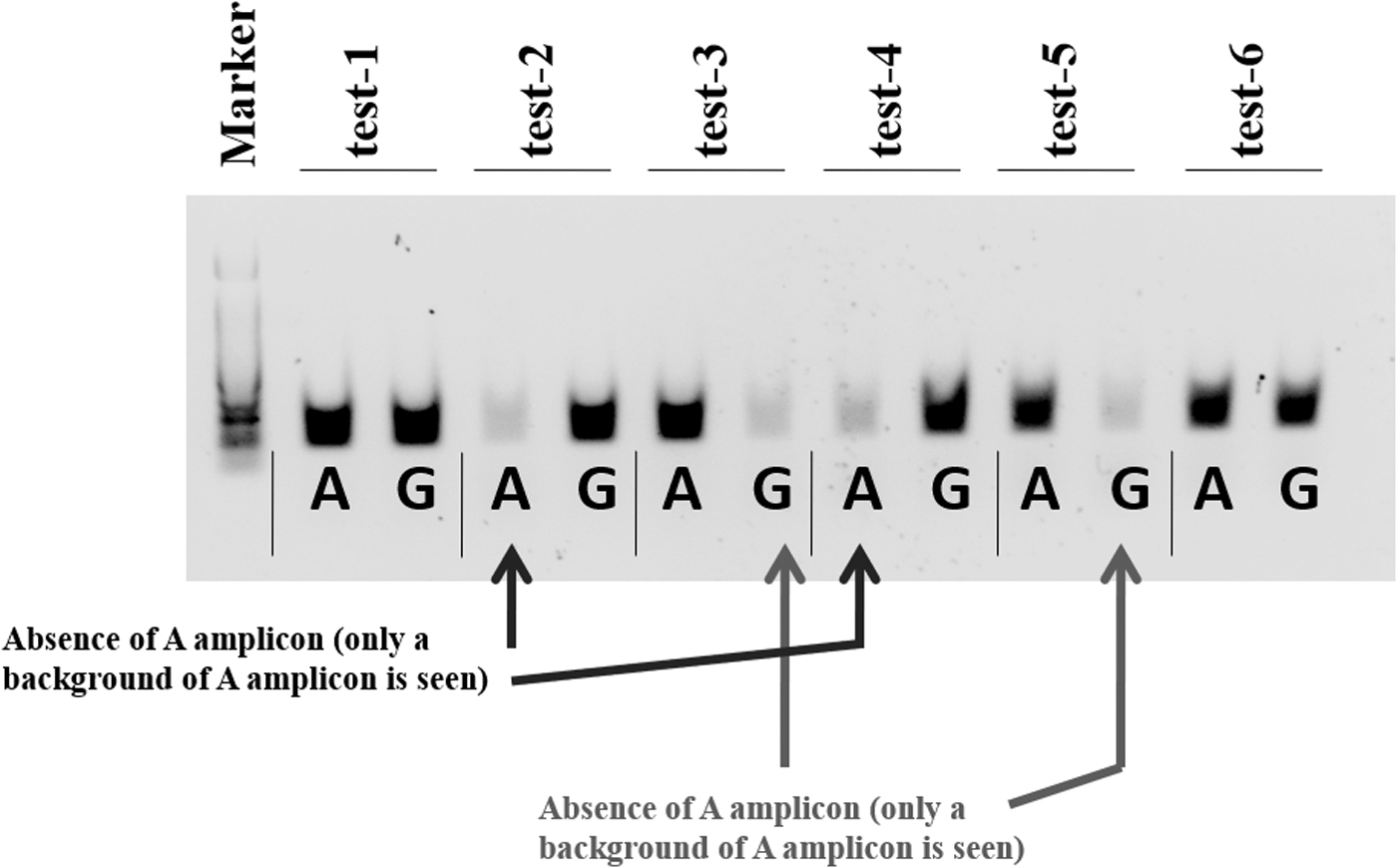
Agarose gel electrophoresis of allele-specific PCR products. PCR, polymerase chain reaction.
The allele frequencies were checked for equilibrium using the Hardy-Weinberg equation. Differences among the mean of age and clinical parameters between the two independent groups were analyzed statistically using independent t test. Pearson's chi-squared test was used to identify the association among the categorical variables. The strength of association between the genotype/allele (exposure) and periodontitis (outcome) was determined using univariate binary logistic regression analysis (odds ratio [OR]).
Results
The mean age of subjects in Group I and Group II was 32 and 42 years, respectively, and the intergroup comparison of age-based subjects through independent t test showed a statistically significant difference between the two groups (Table 1). The number of male and female subjects was 65 and 80 in Group I, and 75 and 70 in Group II, respectively. Pearson's chi-squared test showed no statistically significant difference in gender distribution, indicating a gender match between the groups (p > 0.05) (Table 1). The mean values of PI, MSBI, PPD, and CAL were analyzed between the two groups using Mann-Whitney U test, which showed a statistically significant difference between the two groups (Table 1).
Baseline Characteristics and Clinical Parameters Among the Groups
Highly significant.
represents that they are STATISTICALLY HIGHLY SIGNIFICANT.
mCAL, mean clinical attachment loss; mMSBI, mean modified sulcus bleeding index; mPI, mean plaque index; mPPD, mean pocket probing depth.
Table 2 shows the group-wise distribution of CASP3 rs4647602 TT, GT, and GG genotypes. Distribution of polymorphic genotypes between the two groups was statistically significant (p < 0.001).
Genotypes Distribution Between the Groups
represents that they are STATISTICALLY HIGHLY SIGNIFICANT.
N, no. of subjects.
The association of polymorphic genotypes and alleles with periodontitis was estimated using the OR, 95% CIs, and p-value (Table 3).
Association of CASP3 rs4647602 Gene Polymorphic Genotypes and Alleles with Periodontal Disease
represents that they are STATISTICALLY HIGHLY SIGNIFICANT.
95% CI, 95% confidence interval; LL, lower limit; UL, upper limit; OR, odds ratio; N, no. of subjects.
The association and increased risk for periodontitis were with the variant genotypes GT and GG with OR = 1.79 (95% CI = 1.05-3.08, p = 0.034) and OR = 3.55 (95% CI = 1.89-6.68, p = 0.001), respectively. G allele was highly significant with periodontitis (OR = 2.12, 95% CI = 1.52-2.96, p < 0.001).
Table 4 shows the association of clinical parameters with polymorphic genotypes in periodontitis subjects. All polymorphic genotypes were highly significant with the clinical parameters.
Comparison of Genotypes with Respect to Clinical Parameters
Significant.
CAL, clinical attachment loss; MSBI, modified sulcus bleeding index; PI, plaque index; PPD, probing pocket depth; SD, standard deviation.
Discussion
CASP3 gene encodes for the Caspase-3 apoptotic marker and exhibits several SNPs found in its exonic, intronic, promoter, and UTR regions. Despite the availability of studies on CASP3 gene polymorphism in several chronic inflammatory diseases, no scientific literature reporting the association of this gene polymorphism with periodontitis subjects in the Indian population of Tamil ethnicity has been reported yet. Therefore, the present study shows the frequency of CASP3 rs4647602 polymorphism and its association with periodontitis in South Indian population with Tamil ethnicity.
The genotype frequencies of CASP3 rs4647602 in periodontitis followed the Hardy-Weinberg Equilibrium (p = 0.0002). The homozygous TT genotype was present in 46.9% of periodontally healthy subjects and in 27.6% of subjects with periodontitis. The distribution of the heterozygous GT genotype was 37.2% and 39.3% in periodontally healthy and periodontitis subjects, respectively. The homozygous GG genotype occurred in 15.9% of periodontally healthy subjects and in 33.1% of periodontitis subjects. All polymorphic genotypes (TT, GT, and GG) had a statistically significant difference between the test group and the control group (p < 0.001). Furthermore, it needs to be highlighted that the TT genotype was higher in periodontally healthy subjects, whereas the GT and GG genotypes were higher in subjects with periodontitis in South Indian population with Tamil ethnicity. Similarly, Kang et al. (2015) noticed similar results in GT genotype distribution in the South Korean population, where a higher OR was observed in periodontitis subjects (OR = 14; 95% CI = 2.46-79.55, p = 0.003).
The association of alleles was correlated with periodontitis using logistic regression analysis. It was found that G allele was significantly linked with periodontitis (OR = 2.12, 95% CI = 1.52-2.96, p < 0.001), suggesting that polymorphic G allele was associated with periodontitis. The results were similar to those of Kang et al. (2015), who demonstrated that the C, G, and T alleles of the CASP3 rs4647602 were associated with advanced periodontal disease.
Further G allele of CASP3 rs4647602 has been associated with carcinomas. Heidari et al. (2020) observed that G allele of CASP3 rs4647602 was associated with papillary thyroid carcinoma in an Iranian population, suggesting that CASP3 rs4647602 gene polymorphism plays a role in carcinogenesis through the dysregulation of apoptosis through caspase activation. Similarly, Chen et al. (2008) concluded that rs4647602: C allele may be a risk allele for squamous cell carcinoma of head and neck in the Chinese population.
Assessment of periodontal clinical parameters gives a better understanding of gene polymorphism and association of disease severity. In the present study, all clinical parameters were significantly associated with all polymorphic genotypes, GG, GT, and TT. Furthermore, the polymorphic GG genotype was highly significant with the periodontal clinical parameters, namely, PPD, CAL, PI, and MSBI. Kang et al. (2015) observed CASP3 gene polymorphism in periodontitis subjects with CAL and increased probing depth. However, they did not correlate the clinical parameters with the polymorphic genotypes and alleles.
The results of the present study are in accordance with those of Kang et al. (2015) among the South Korean population. The similarity observed with the present ethnic group is possibly due to the similar frequency of CASP3 rs4647602 distribution between the two populations.
The frequency distribution of the polymorphic alleles observed in the present study population could not be compared due to the unavailability of CASP3 gene polymorphism studies among periodontally healthy and periodontitis subjects in India.
It is suggested that CASP3 rs4647602 gene polymorphism could be a risk factor for periodontitis among the samples of ethnic Tamil individuals.
CASP3 rs46476032 GG genotype was found to be associated with periodontitis in Tamil ethnic population, whereas GT genotype SNP was more associated with periodontitis in South Korean population. Such a finding is reasonable because the genetic variants influence disease susceptibility in polygenic disease by acting collectively with other disease-modifying genes or in combination with environmental, hormonal, or metabolic factors. However, such a cause-effect relationship needs to be further confirmed in longitudinal studies.
The present study has few limitations. First, the present study is observational in design and hence, causal relationships cannot be demonstrated. Second, sampling is based on convenience sampling, and it may therefore not represent the population. Third, the present study is conducted on South Indians belonging to Tamil ethnic background. Assessment and comparison of CASP3 rs4647602 gene polymorphism in various ethnic populations gives more insight about the role of CASP3 gene polymorphism in association with periodontitis.
CASP3 rs4647602 SNP is present among South Indian individuals belonging to Tamil ethnic background and a significant association was observed between the CASP3 rs4647602 gene polymorphism and the periodontitis subjects. The variation of CASP3 genotype in Tamil ethnicity could be of importance as there is a difference of dietary habits like consuming carbohydrate-rich diet, specific cultural practices, and people living in rural areas have no access to dental care. Considering the above variables, it can be suggested that the disease severity can be different across ethnicities. To conclude, CASP3 gene polymorphism may be a predictable indicator of susceptibility to periodontal disease in the Indian population. Larger population-based studies on CASP3 gene polymorphism needs to be conducted in the future.
Footnotes
Acknowledgments
The authors thank SRM Dental College, Ramapuram, Chennai for providing the study participants, and Dr. Arvind Ramanathan, BDS, MSc (Molecular Biology), PhD (Molecular Oncology, Tokyo, Japan), Director of Research, Enable Biolabs, for carrying out the research work.
Authors' Contributions
A.M.L.: Conceptualization (lead); resources (lead); formal analysis (equal); formal analysis (equal); and funding and acquisition. D.P.: Supervision (lead); validation (lead); visualization (lead); writing—original draft (lead); investigation (lead); and formal analysis (equal). H.P.: Project administration (supporting); and supervision (supporting). A.T.: Project administration (supporting); and supervision (supporting). D.J.V.: Writing—review and editing (equal); and data curation (lead).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.