
Abstract
Objective:
To investigate the role of the SRY-box transcription factor 2 (SOX2) in endometrial carcinoma and the diagnostic value of serum SOX2 levels combined with magnetic resonance imaging (MRI).
Methods:
The present prospective observational study included 326 cases of endometrial carcinoma. All patients received measurements of serum SOX2 and MRI detection two weeks prior to surgery. Patients' demographic and clinical data including age, BMI, cancer stage, tumor differentiation, invasion, and lymph node metastasis were collected. All patients were followed for 5 years following surgery.
Results:
Deceased patients showed significantly higher ratios of: FIGO stage III-IV tumors; low tumor differentiation; myometrial invasion depths of >1/2 and cervical invasion. Lymph node metastases and distant metastasis were significantly lower in surviving patients than those in deceased patients. The serum levels of SOX2 were significantly higher in endometrial carcinoma patients compared with the healthy controls and were remarkably higher in deceased patients. Patients with elevated SOX2 levels also had higher rates of FIGO stage III-IV, higher rates of myometrial invasion depth >1/2 and higher rates of low tumor differentiation. Elevated SOX2 levels are correlated with higher rates of lymph node metastases, distant metastases and 5-year mortality. Serum SOX2 levels combined with MRI have the potential to improve the diagnosis of myometrial invasion and lymph node metastasis in endometrial carcinoma.
Conclusion:
Elevated serum SOX2 levels were associated with poor prognoses of patients with endometrial carcinoma. Serum SOX2 levels combined with MRI could be useful in the diagnosis and prognosis of endometrial carcinoma.
Introduction
Endometrial carcinoma is one of the most common gynecological cancers, with the highest incidence in North America and western Europe (Brüggmann et al, 2020; Dizdar and Kılıçkap, 2019; Mäenpää, 2020; Piulats et al, 2017). Patients with early stage of endometrial carcinoma usually have well prognosis, with a low mortality rate ranging from 1.7 to 3.6 in developed countries and 5-year survival rate up to 90% (Felix et al, 2018; Mäenpää, 2020; Visser et al, 2017). However, the 5-year survival rate of endometrial carcinoma patients with advanced endometrial carcinoma is usually low, especially for patients with distant metastasis (<20%) (Dizdar and Kılıçkap, 2019; Hammer et al, 2015; Visser et al, 2017). Thus, the early diagnosis of endometrial carcinoma is of great significance to enhance patients' prognosis.
There are several biomarkers reported in the diagnosis of endometrial carcinoma, such as ER, PR, and Ki67 (Buhtoiarova et al, 2016; Masjeed et al, 2017; Stoian et al, 2011). Some novel biomarkers are also reported. It was found HE4 was downregulated in endometrial carcinoma and the cutoff values <70 and <150 pM had the potential as diagnosis and prognosis biomarker for endometrial carcinoma (Angioli et al, 2013). In another research, a novel biomarker HSPA8 was found as a candidate biomarker for endometrial carcinoma, which was upregulated in endometrial carcinoma (Shan et al, 2016). Among the biomarkers, SRY-box transcription factor 2 (SOX2) was also reported to participate in endometrial carcinoma. It has been found that expression of SOX2 is associated with poor histological differentiation and survival, and that SOX2 promotes endometriosis and carcinoma cell migration (Lee et al, 2018). However, up to now, the clinical significance of SOX2 in endometrial carcinoma is still inadequate.
In this study, we performed an observational study to investigate the role of SOX2 in endometrial carcinoma patients and the possible combination use of serum SOX2 level and magnetic resonance imaging (MRI) in the diagnosis of endometrial carcinoma. It has been observed that higher SOX2 levels predict a poorer prognosis, and MRI combined with serum SOX2 levels is a potential method in the diagnosis of endometrial carcinoma.
Materials and Methods
Patients
This prospective observational study included 326 cases of endometrial carcinoma patients who came to our department from March 2013 to December 2015. All patients were diagnosed as endometrial adenocarcinoma. The inclusion criteria were as follows: (1) the diagnosis of endometrial carcinoma of all patients was confirmed by histological analysis; (2) all patients were diagnosed as primary endometrial carcinoma; and (3) the patients received no chemotherapy or radiotherapy before the study.
The following patients were excluded: (1) patients with other cancers; (2) patients who received endocrine therapy before; and (3) patients with severe cardiovascular, renal, or liver dysfunctions. Patients' cancer stage was evaluated according to the criteria of International Federation of Gynecology and Obstetrics (FIGO) (Soslow et al, 2019). Blood samples of 326 healthy individuals who came to our hospital for physical examination. This study was approved by the ethics committee of Jiading District Central Hospital Affiliated Shanghai University of Medicine & Health Sciences (SMHCU-201315).
MRI detection
All patients underwent MRI detection 2 weeks before surgery using a Philips 3.0T body array coil. The depth of myometrial invasion, possibility of accumulation of cervical stroma, pelvic and/or para-aortic lymph nodes, signs of metastasis, and the size of intrauterine tumor were mainly concerned. Myometrial invasion was divided as <1/2 and >1/2. The FIGO stages were defined as follows: IA stage, the tumor only invaded the endometrium and did not reach the muscularis or the depth of muscularis invasion was <1/2; the IB stage, the tumors were only seen in the interior of the uterine body and the depth of muscularis invasion >1/2; II stage the tumor involved cervical stroma, but there was no clear extension of uterus in vitro; III stage, the invasion of uterine serosa, the involvement of vagina and adnexa, and the enlargement and metastasis of lymph nodes were observed; IV stage, distant metastasis was observed. The MRI results were evaluated and analyzed by two independent physicians who were blinded to the histological results of patients.
Measurement of serum SOX2 level
The measurement of serum SOX2 level was performed at 2 weeks before surgery. The fasting peripheral venous blood (5 mL) was collected in anticoagulant free tubes, following by centrifugation at 12,000 g for 15 min. The serum level of SOX2 were determined by enzyme-linked immunosorbent assay (ELISA) using commercial kit (MyBioSource; cat. no. MBS2513016) strictly according to manufacturer's instruction.
Data collection and follow-up
Patients' demographic data and clinical data, including age, BMI, cancer stage, tumor differentiation, invasion, and lymph node metastasis, were collected. All patients were followed up for 5 years. Survival duration was defined from admission to death or the last follow-up.
Statistical analysis
The normality of data distribution was tested by the Kolmogorov-Smirnov test. Data were expressed as mean ± SD. Comparison between two groups was conducted using Student's t-test. Receiver operating characteristic (ROC) curve was used for diagnostic analysis. The 5-year overall survival was analyzed by Kaplan-Meier (K-M) curve. All calculations were performed using SPSS 18.0. p < 0.05 was regarded as statistically different.
Results
Basic clinical characteristics of all patients
This prospective observational study included 326 cases of endometrial carcinoma patients. During 5 years' follow-up, 73 patients died and 253 patients survived (Table 1). The ratio of FIGO stage III-IV patients was markedly higher in deceased patients compared with the survival patients (p < 0.05). Meanwhile, ratios of patients with low tumor differentiation, myometrial invasion depth >1/2, cervical invasion, as well as lymph node metastasis and distant metastasis were all significantly lower in survival patients than those in deceased patients. No significant difference was found in age and BMI between endometrial carcinoma patients and the healthy control.
Basic Clinical Characteristics of All Patients
Comparisons for all variables were performed between the survival and deceased patients.
FIGO, International Federation of Gynecology and Obstetrics.
Serum SOX2 level was elevated in endometrial carcinoma patients
Serum SOX2 level was determined in endometrial carcinoma patients and the healthy control. It was found that serum SOX2 level was significantly higher in endometrial carcinoma patients compared with the healthy control (p < 0.05, Fig. 1). Besides, serum SOX2 level was remarkably higher in deceased patients than in the survival patients.
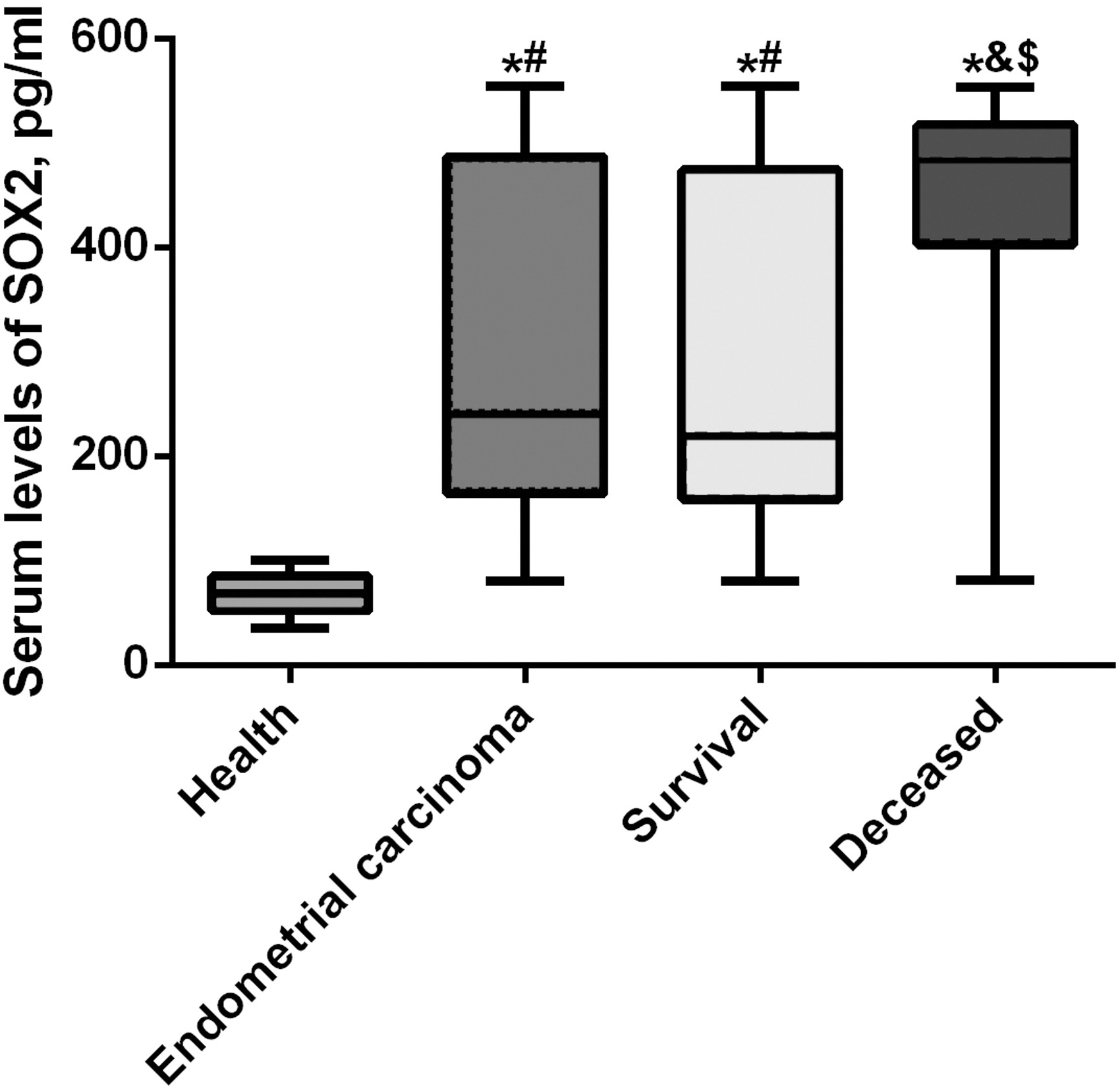
Serum level of SOX2 in all endometrial carcinoma patients, survival and deceased patients, as well as in healthy control. *p < 0.05 compared with the health group; #p < 0.05 compared with the endometrial carcinoma group; &p < 0.05 compared with the endometrial carcinoma group; $p < 0.05 compared with the survival group. SOX2, SRY-box transcription factor 2.
Higher serum SOX2 level predicted poorer clinical outcomes
To further investigate the role of SOX2 in endometrial carcinoma, all patients were divided into high group and low group based on the mean level of SOX2 at 239.65 pg/mL. It was found that patients with higher level of SOX2 showed higher rates of FIGO stage III-IV, higher rates of myometrial invasion depth >1/2 and higher rates of low tumor differential (p < 0.05, Table 2). Moreover, higher level of SOX2 also predicted higher rates of lymph node metastasis, distant metastasis, and 5-year mortality.
Clinical Characteristics of Patients with High or Low SOX2
Comparison for all variables was performed between the SOX2 high/low groups of patients.
SOX2, SRY-box transcription factor 2.
Diagnostic value of serum SOX2 in endometrial carcinoma, myometrial invasion, and lymph node metastasis
Then, ROC curve was employed to show the diagnostic value of SOX2 for endometrial carcinoma. It was found the cutoff value of SOX2 for endometrial carcinoma was 93.61 pg/mL, with area under curve (AUC) of 0.993, sensitivity of 97.5%, and specificity of 90.2% (Fig. 2). The cutoff value of SOX2 for myometrial invasion >1/2 was 227.28 pg/mL, with AUC of 0.699, sensitivity of 65.3% and specificity of 72.0%. The cutoff value of SOX2 for lymph node metastasis was 227.28 pg/mL, with AUC of 0.725, sensitivity of 69.1%, and specificity of 73.8%.
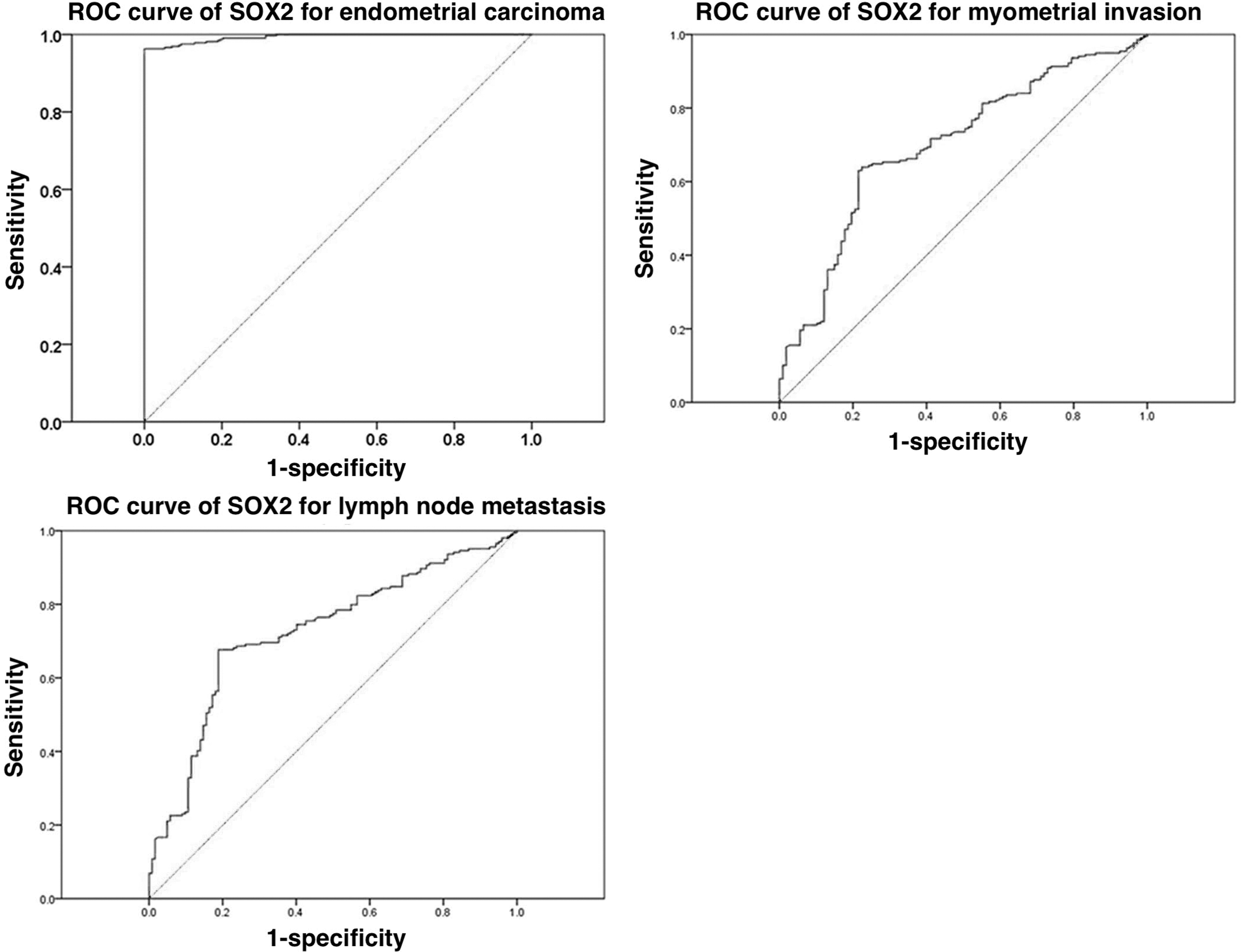
ROC curves for SOX2 in diagnosis of endometrial carcinoma, myometrial invasion, and lymph node metastasis. ROC, receiver operating characteristic.
MRI combined with serum SOX2 level in the diagnosis of myometrial invasion and lymph node metastasis
MRI combined with serum SOX2 level were utilized in the diagnosis of endometrial carcinoma, myometrial invasion, and lymph node metastasis. All patients received MRI at 2 weeks before the surgery (Fig. 3). In this study, we used the cutoff values of SOX2 aforementioned as the diagnostic cutoff values for myometrial invasion (227.28 pg/mL) and lymph node metastasis (227.28 pg/mL). As shown in Table 3, for myometrial invasion >1/2, the sensitivity and specificity were 99.09% and 97.20%, respectively, for MRI, whereas were 65.30% and 71.96%, respectively, for SOX2, and were 99.54% and 70.09%, respectively, for SOX2/MRI. For lymph node metastasis, the sensitivity and specificity were 99.02% and 98.36%, respectively, for MRI, whereas were 69.12% and 73.77%, respectively, for SOX2, and were 100% and 72.13%, respectively, for SOX2/MRI.
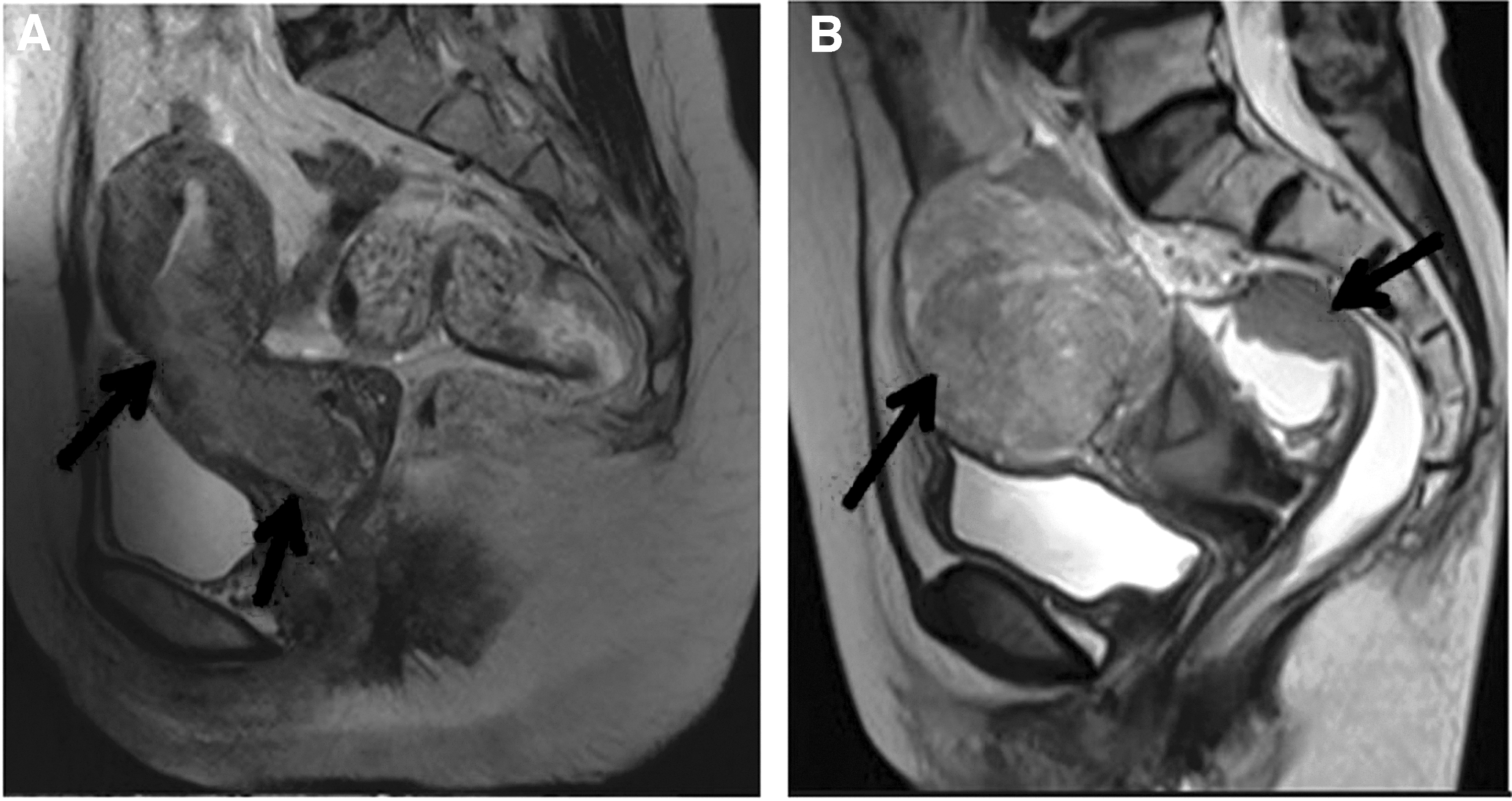
Magnetic resonance imaging results for endometrial carcinoma patients.
Combination of MRI and Serum SOX2 in Diagnosis of Endometrial Carcinoma, Myometrial Invasion, and Lymph Node Metastasis
Sensitivity = true positive/(true positive + false negative) × 100%; specificity = true negative/(true negative + false positive) × 100%; accuracy = (true positive + true negative)/(true positive + false negative + false positive + true negative) × 100%.
MRI, magnetic resonance imaging.
Association between serum SOX2 level and 5-year overall survival of endometrial carcinoma patients
At last, the 5-year overall survival of endometrial carcinoma patients was analyzed in patients with high/low SOX2 level. As shown in Figure 4, K-M curve showed higher serum SOX2 level showed significantly shorter overall survival (p < 0.05), suggesting higher serum SOX2 level predicted poor prognosis in endometrial carcinoma patients.

K-M curve. The 5-year overall survival was analyzed by the K-M method. K-M, Kaplan-Meier.
Discussion
Although the prognosis of early endometrial carcinoma is favorable, advanced endometrial carcinoma patients usually suffer from low 5-year survival (Lax, 2017). Thus, novel biomarkers and diagnostic methods for endometrial carcinoma are still needed. In this research, we demonstrated that serum SOX2 level was elevated in endometrial carcinoma patients and higher serum SOX2 level predicted poor clinical outcomes and prognosis, whereas MRI combined with serum SOX2 level had the potential to be used in the diagnosis and prediction of endometrial carcinoma.
SOX2 has been reported as a tumor-related protein in several cancers, including endometrial cancers. A recent research demonstrated that SOX2 predicted poor histological differentiation and survival condition, and also facilitated cell proliferation and migration of endometrial carcinoma cells (Lee et al, 2018). It was also found in endometrial cancer stem-like cells, the demethylation of SOX2 could promote the tumor initiation capacity (Chen et al, 2020). Yamawaki et al (2017) also found that SOX2-dependent inhibition of p21 was associated with poor prognosis of endometrial cancer. Whereas in small cell neuroendocrine carcinoma of the endometrium, SOX2 also showed positive expression (Ebisu et al, 2020). In this research, we found that SOX2 was upregulated in serum of endometrial carcinoma patients and was associated with the prognosis of patients. However, the molecular mechanism of SOX2 in the development of endometrial carcinoma is still unclear and needs further studies to confirm.
MRI is a common and widely applied method in cancer diagnosis, including endometrial carcinoma (Faria et al, 2015). It was found preoperative tumor texture analysis on MRI had the potential to predict prognosis in endometrial cancer, in which high tumor entropy in apparent diffusion coefficient (ADC) maps predicted deep myometrial invasion (Ytre-Hauge et al, 2018). Engerud et al (2019) found that high tumor volume detected by preoperative MRI was associated with high plasma GDF-15. In another research, Jiang et al (2018) demonstrated that the ADC value by diffusion-weighted MRI was negatively correlated with expression of Ki67 in endometrial carcinoma. In our research, we found that the application of MRI could achieve acceptable sensitivity and specificity in the diagnosis of endometrial carcinoma, myometrial invasion, and lymph node metastasis, whereas MRI combined with serum SOX2 level showed better sensitivity and accuracy.
This study also has some limitations. First, the sample size is small from a single center. Second, the molecular mechanism for SOX2 in the development of endometrial carcinoma is still unknown. Third, the relationship between SOX2 and other biomarkers for endometrial carcinoma is not clear. All these need more studies to further clarify.
Conclusion
In conclusion, this observational research demonstrated that the upregulated serum SOX2 level predicted poor clinical outcomes and prognosis of endometrial carcinoma patients, and combination of MRI and SOX2 might be a potential method in diagnosis of endometrial carcinoma. This research might provide novel research targets for endometrial carcinoma (Sode-Carlsen et al, 2010).
Footnotes
Authors' Contributions
Review and editing (equal) by T.B. Conceptualization (lead), writing—original draft (lead), formal analysis (lead), writing—review and editing (equal), software (lead), and writing—review and editing (equal) by C.L. Methodology (lead) and writing—review and editing (equal) by K.L. Conceptualization (supporting), writing—original draft (supporting), and writing—review and editing (equal) by X.Y. and T.B.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study is supported by Key Medical Subject of Jiading District (2020-jdyxzdzk-02) and Scientific research project of Jiading District Health Committee of Shanghai (2021-KY-02).