
Abstract
Objective:
To examine the rate of recurrence for elevated isolated maternal serum alpha-fetoprotein (MSAFP) and its associated adverse outcomes during a subsequent pregnancy.
Materials and Methods:
A retrospective cohort study of pregnant multiparous women who had elevated MSAFP levels during an initial and a subsequent pregnancy between 1994 and 2020.
Results:
Twenty-seven out of 344 (7.8%) women with elevated MSAFP had recurrent elevated MSAFP in a subsequent pregnancy. Four women were excluded due to missing data. Of the 23 women included, 5 (22%) had fetal growth restriction (FGR), 2 (9%) had pre-eclampsia, 9 (35%) had preterm births, and 2 (9%) had fetal death/miscarriage in their subsequent pregnancy. Looking at individual outcomes, 60% of women had recurrence of preterm labor, 33% had recurrence of fetal death, and 25% had recurrence of FGR.
Conclusion:
Women with elevated MSAFP levels during an initial pregnancy should be informed during preconception counseling about their risk of recurring elevated MSAFP and its associated adverse outcomes risks.
Introduction
Alpha-fetoprotein is a glycoprotein that is produced by the fetal yolk sac, liver, and gastrointestinal system in early pregnancy (Cunnigham et al, 2010). Maternal serum alpha-fetoprotein (MSAFP) has traditionally been used as a primary screening measure during pregnancy to determine increased risk for open neural tube defects (Habib, 1977). MSAFP screening is done in the second trimester and levels are reported in multiples of the median (MoM) using unaffected pregnancies of the same gestational age as the reference group (Committee on Practice Bulletins-Obstetrics, 2017).
Although elevated MSAFP can indicate fetal abnormalities, many studies have shown a correlation between unexplained isolated elevated MSAFP levels and adverse pregnancy outcomes (Chandra et al, 2003; Crandall et al, 1991; Dugoff et al, 2005; Robinson et al, 1989). Isolated elevated MSAFP is an elevated MSAFP value >2.0-2.5 MoM (pending specific laboratory criteria), without associated fetal anomalies.
In the second trimester, unexplained isolated elevated MSAFP levels (i.e., correct gestational age and no structural fetal anomalies) have been associated with increased risk for fetal death, fetal growth restriction (FGR), low fetal birth weight, premature delivery, placental abruption, and pre-eclampsia (Başbuğ et al, 2017; Chandra et al, 2003; Crandall et al, 1991; Davidson et al, 2003; Dugoff and Society for Maternal Medicine, 2010; Dugoff et al, 2005; Jauniaux et al, 1996; MacRae, 1990; Milunsky, 1992; Öztürk et al, 2014; Robinson et al, 1989; Wapner et al, 2009). These adverse outcomes can be indicative of a defect in placentation. In fact, some studies have highlighted that elevated MSAFP levels are associated with placental pathology such as placental infarction, ischemia, chronic villitis, and thrombosis (Jauniaux et al, 1990; Morssink et al, 1996).
Since MSAFP testing is generally done throughout multiple pregnancies, recurrent elevation of MSAFP levels could incur a recurrent risk for adverse perinatal outcomes. There is a paucity of literature on MSAFP recurrence rates and associated outcomes in subsequent pregnancies (Dar et al, 1996; Wax et al, 2000). The aim of this study was to examine the recurrence rate of elevated MSAFP levels across multiple pregnancies among multiparous women and to assess the correlation of recurring elevated MSAFP levels with abnormal placental pathology and adverse perinatal outcomes (Redline, 2015).
Materials and Methods
A retrospective cohort study was performed using data from the Alpha genetic software database at Henry Ford Hospital. The research was determined to be exempt by the Henry Ford Health Institutional Review Board (No. 14087) as it involves a retrospective chart review with no patient identifiers requested or linked to study subjects. The study was performed in accordance with the Declaration of Helsinki. We used data describing pregnant multiparous women in southeast Michigan from January 1, 1994, to December 31, 2020. The women included in the study had at least one subsequent pregnancy with second trimester screening (between 15 and 22 weeks of gestation) within the study timeframe.
Abnormal elevation in MSAFP was defined as a value ≥2.2 MoM and was based on Henry Ford Laboratory testing criteria. Inclusion criteria included the following: multiparous women with more than one newborn delivered, women with singleton live births, reliable pregnancy dating from either certain last menstrual period or ultrasound in the first trimester, and MSAFP screening in the second trimester between 15 and 22 weeks gestation. Exclusion criteria included the following: women with multiple gestations and pregnancies complicated by fetal anomalies or chromosomal abnormalities (Fig. 1). MSAFP testing was done using blood sample drawn from pregnant women within the appropriate gestational age already described.

Selection algorithm for study participants, data from January 1, 1994, and December 31, 2020. MSAFP, maternal serum alpha-fetoprotein.
Adverse perinatal outcomes included preterm birth (<37 weeks), pre-eclampsia, FGR, fetal death or miscarriage, and abnormal findings from placental pathology. Data were extracted from patient records at Henry Ford Health System in the EPIC system (Epic Systems Corporation, Verona, WI) if they occurred after 2013 and from the CPNG system (Reliance Software Systems, Inc., Farmington Hills, MI) if they occurred before 2013.
Statistical analysis
Paired t-tests and chi-square tests were used to compare the characteristics for the two pregnancy groups—women in the initial pregnancy with elevated MSAFP versus the same women in the subsequent pregnancy with recurrent elevated MSAFP. Microsoft Excel 2019 software, by Microsoft corporation, was used to perform the statistical analysis. Recurrence rates for isolated elevated MSAFP and rates for adverse pregnancy outcomes were derived by calculating percentages based on the values in the initial and subsequent pregnancies.
Results
A total of 99,709 MSAFP tests were performed between 1994 and 2020, and 2.8% were elevated MSAFP values. A total of 344 multiparous women had positive isolated elevated MSAFP values and met the inclusion criteria defined in the Materials and Methods section, of which 27 (7.8%) had a recurrent elevated MSAFP value in a subsequent pregnancy. There was no significant difference (p = 0.228) in the mean age (±standard deviation) of women with recurrent elevated MSAFP values (27.1 years ±6.8) and of women without the recurrence (26.1 years ±5.5). There was no significant difference (p = 0.548) in the MSAFP MoM values between women with recurrent elevated MSAFP values (median 2.75, interquartile range [2.3-3.3]) and women without recurrence (median 2.60, interquartile range [2.4-3.2]).
Of the 27 women with recurrent elevated MSAFP values, 54 records were reviewed. Results for 47 of the 54 records were available in the electronic medical record. A total of three women had missing results for pregnancy outcomes for both pregnancies, and one woman had missing results for pregnancy outcomes of her subsequent pregnancy secondary to moving abroad. Because of the missing data for one or both pregnancies, these 4 participants were eliminated from the final data analysis, leaving 23 women whose records were analyzed. In this group of 23 women, 56.5% (n = 13) were African American, 21.7% (n = 5) were White, 8.6% (n = 2) were Hispanic, 8.6% (n = 2) were Arabic, and 4.3% (n = 1) were Asian.
Table 1 summarizes the characteristics of the 23 women at their initial and subsequent pregnancies. Of the initial pregnancies analyzed, the majority of women were either primiparous or were having their second pregnancy. The average age in either pregnancy remained below the advanced maternal age (defined as 35 years old at estimated date of delivery), which is a known risk factor for many adverse obstetrical and perinatal outcomes. The mean ± standard deviation MSAFP levels were not significantly different between initial pregnancies (3.0 MoM ±0.7) and subsequent pregnancies (3.2 MoM ±1.7).
Characteristics of Women Who Had Recurrent Maternal Serum Alpha-Fetoprotein Levels at an Initial and Subsequent Pregnancy
p Values from paired t test comparing initial pregnancy with subsequent pregnancy.
MoM, multiples of the median; MSAFP, maternal serum alpha-fetoprotein; n/a, not applicable; SD, standard deviation.
Body mass index was also comparable between both pregnancies and averaged below the level of obesity, which is a contributing risk factor for morbidity and mortality in pregnancy. There was also no significant difference in history of chronic hypertension. Only one woman had gestational diabetes in her initial pregnancy, and none of the women had prepregnancy diabetes.
Table 2 summarizes the pregnancy outcomes for women in their subsequent pregnancy. The majority of the placentas analyzed during the second pregnancy were noted to have an abnormal pathology, although it is worth noting that 11 out of the 23 subsequent pregnancies had placentas that were not sent to pathology. Abnormal placental pathology was defined as placenta showing placental vascular processes, placental inflammatory immune processes, or other placental processes incorporating the 2014 Amsterdam Placental Workshop Group criteria (Phillips et al, 2017).
Pregnancy Outcomes for Women in Their Subsequent Pregnancy
Total number of abnormal placentas sent for pathology was 12 for the subsequent pregnancies.
Preterm birth was the adverse outcome that occurred the most frequently during the subsequent pregnancy (35%, n = 8), followed by FGR (22%, n = 5) and then fetal death and pre-eclampsia each occurring at 9% (n = 2). It is worth noting that no significant differences were observed in the occurrence of any adverse outcome—FGR, pre-eclampsia, preterm birth, fetal death, and abnormal placental pathology—between the initial and subsequent pregnancy (Table 2).
Figure 2 highlights the rate of recurrence of maternal outcomes in the subsequent pregnancy compared with the initial pregnancy. Of the 11 women who had a normal initial pregnancy, 8 (73%) had a subsequent normal pregnancy. Of the 12 women with an abnormal initial pregnancy, whether due to fetal death or miscarriage, preterm labor, FGR, or pre-eclampsia, 8 (67%) had a subsequent abnormal pregnancy. Regarding initial pregnancies with FGR, pre-eclampsia, preterm labor, or fetal death/miscarriage, 1 out of 4 (25%) had subsequent FGR, 0 out of 3 (0%) had subsequent pre-eclampsia, 6 out of 10 (60%) had subsequent preterm labor, and 2 out of 6 (33%) had subsequent fetal death/miscarriage. Of those eight women with abnormal placental pathology in the initial pregnancy, six (75%) had a subsequent abnormal placental pathology.
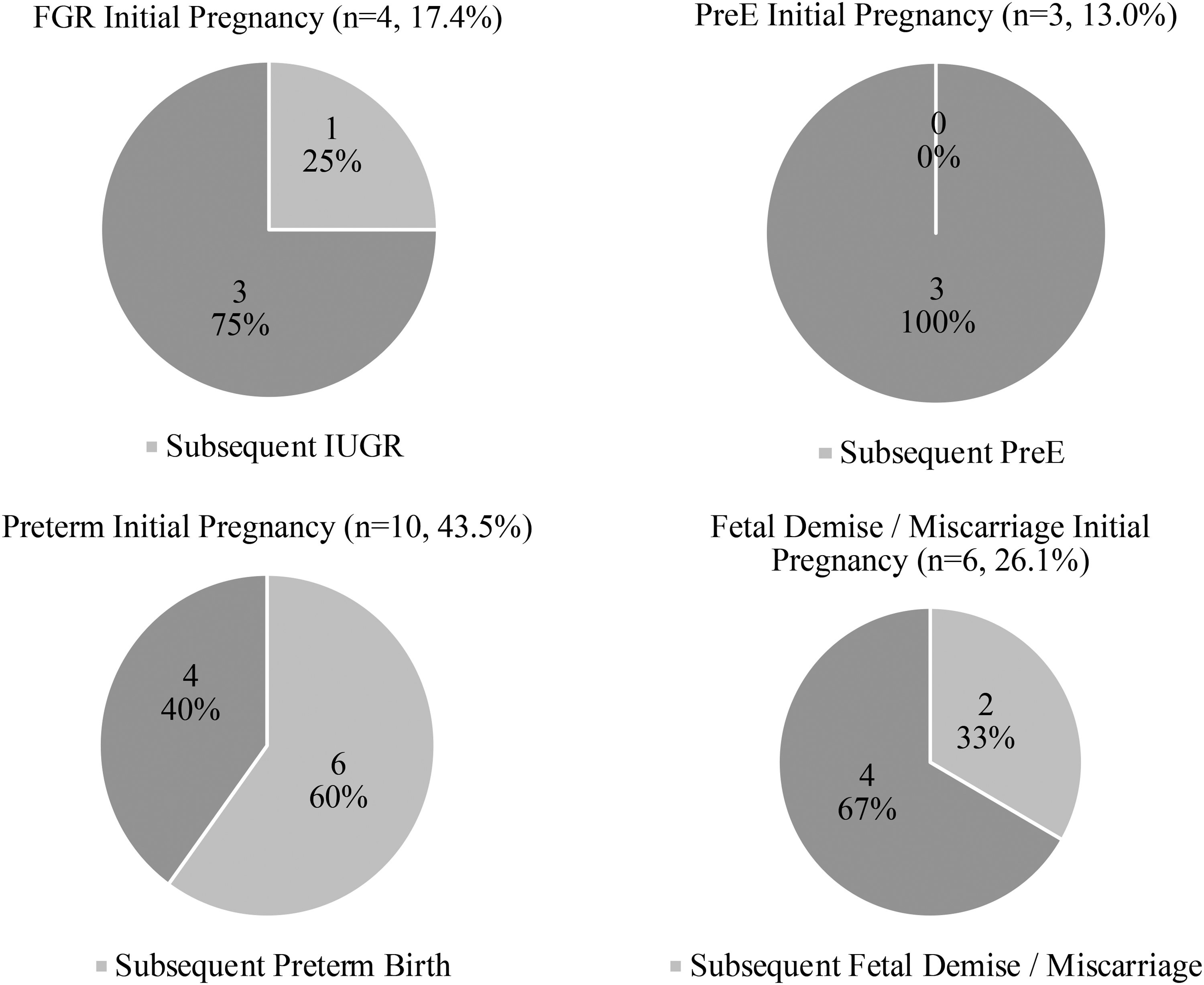
Recurrence of adverse outcomes between initial and subsequent pregnancies. FGR, fetal growth restriction; PreE, pre-eclampsia.
Discussion
In this study, we found a 7.3% recurrence rate for elevated isolated MSAFP value in a subsequent pregnancy. Only two studies have looked at recurring rates of elevated MSAFP values in the literature, and only one of those looked at the impact of such recurrence on adverse pregnancy outcomes (Dar et al, 1996; Wax et al, 2000). The first study focused on completely unaffected uncomplicated singleton pregnancies with no adverse outcomes, and, hence, was not relevant to our hypothesis (Dar et al, 1996). The second study, however, looked at recurrence rates and pregnancy outcomes, among other aneuploidy markers (Wax et al, 2000).
It assessed a total of 538 women, where 23 had elevated MSAFP. Of those with elevated MSAFP levels in the first pregnancy, four (17.4%) had a recurrent elevation in the next pregnancy, which is higher than what we observed but not significantly different from it (p = 0.08). It is worth noting that the number of pregnant women with elevated initial MSAFP values in our study was much higher than that in the Connecticut study (Wax et al, 2000), bringing more power to our results.
In terms of adverse outcomes, we showed in the subsequent pregnancy, 34.8% (n = 8) of subjects having preterm labor, 21.7% (n = 5) having FGR, 8.7% (n = 2) having pre-eclampsia, 8.7% (n = 2) having fetal death or miscarriages, and 83.3% having abnormal placental pathology. The Connecticut study (Wax et al, 2000) did not look at the frequency of the different adverse outcomes because relatively few pregnancies with anomalous analytes experienced adverse perinatal events.
The study showed that only one out of six (16.7%) pregnancies with recurrent elevated MSAFP levels had an adverse event, which was statistically lower than our 67% adverse event recurrence rate (p = 0.045). The study also did not specify which adverse event was noted, and overall, it did not demonstrate an increased risk of adverse perinatal events in pregnancies complicated by recurrent elevated MSAFP.
Our study was able to look into specific adverse events and their recurrence rates between the initial and subsequent pregnancy as shown in Figure 2. We showed that the majority of women (73%) with elevated isolated MSAFP levels with a normal initial pregnancy (i.e., lacking adverse outcomes) continued on to have a normal subsequent pregnancy. Similarly, the majority of women (67%) who had an abnormal initial pregnancy with adverse outcomes had a subsequent abnormal pregnancy with adverse outcomes. We found 60% recurrence of preterm labor, 33% recurrence of fetal death, and 25% recurrence of FGR. It is worth noting that in the general population with normal MSAFP values, the literature cites a recurrence rate for preterm labor, fetal death, and FGR at 23%, 7%, and 20%, respectively (Patterson et al, 1986; Phillips et al, 2017; Sneider et al, 2016).
Relative to the general population, our study showed significantly higher recurrence rates for preterm labor and fetal death when MSAFP was elevated (p = 0.006 and p = 0.017, respectively), but no significant difference for FGR (p = 0.807). Although the etiology of recurrent elevated MSAFP values remains unknown, some suggested causes are intrinsic biological variability, genetic predisposition, and environmental factors that may lead to recurrence in subsequent pregnancies (Dar et al, 1996; Wax et al, 2000). We hope that further larger studies can help us better understand the association between recurrent elevated MSAFP and adverse pregnancy outcomes.
The adverse outcome with the highest percentage in the initial and recurrent pregnancies in our study was abnormal placental pathology (72%), with the highest percentage of that subset being attributed to chorionic villitis at 72% (13 out of 18). There is a paucity of literature that looked into the correlation between elevated MSAFP and placental pathology findings. Such literature has highlighted the association between MSAFP levels and placental infarction, ischemia, chronic villitis, and thrombosis (Jauniaux et al, 1990; Morssink et al, 1996). Because most of these studies had small sample sizes or had described lesions as a group, we cannot discern whether the effect of MSAFP levels on placental lesions is significant.
As placental pathology research continues to improve, and with studies that hopefully can include larger populations where placentas are sent for pathological analysis, we hope that we can delve deeper into the significance of the association between MSAFP levels and placental pathology along with characteristic lesions (Redline, 2015). One future direction could be looking at the placental pathology reports for all pregnancies with elevated MSAFP values and deducing the most common reported abnormal processes as defined by the Amsterdam Placental Workshop Group criteria (Redline, 2015).
Recent evidence suggests that epigenetic changes, in particular altered expression of selective miRNA, could play a key role in placental-induced adverse pregnancy outcomes such as pre-eclampsia and intrauterine growth restriction (Chiofalo et al, 2017; Laganà et al, 2018). The miRNA technology can be a significant breakthrough as it allows for associating biomarkers, whether in placenta or maternal serum, with pregnancy complications such as pre-eclampsia (Laganà et al, 2017; Laganà et al, 2016). Such knowledge and findings can be helpful in terms of the utility of serum biomarkers such as MSAFP as well as other biomarkers as they help predict pregnancy outcomes such as pre-eclampsia, growth restriction, among others.
Some limitations of our study include the small sample size, missing data, and grouping of spontaneous and induced preterm labor patients into one category. Given the small sample size, we did not adjust for maternal weight, race, and maternal insulin-dependent status, as factors into MSAFP, MoM values. Another limitation was not including consecutive pregnancies, as in other studies (Dar et al, 1996; Wax et al, 2000), but rather assessing any subsequent pregnancy with elevated MSAFP values. This approach, however, allowed us to have a larger data set and it did not compromise the aim of our study.
Lastly, we were limited by not being able to perform additional analyses for relative ratios and examining adverse outcomes in pregnancies with nonelevated MSAFPs (Chandra et al, 2003; Dar et al, 1996; Puntachai et al, 2015). That was due to the limitation with pulling data from our health system before 2013 that comprised a large percentage of our patient population. This led us to analyze our results from a different lens and focus, as described in the results section, on data from the literature regarding recurrence rates of adverse outcomes from the general population with normal MSAFP values.
Conclusions
Our study is unique in showing both the recurrence rate of elevated MSAFP levels and the increased risk for adverse pregnancy outcomes in recurrent pregnancies. We highlight the significance of abnormal placental pathology that was present in the majority of our study population. For women with a history of elevated isolated MSAFP, we recommend communicating rates of elevated MSAFP recurrence and associated adverse pregnancy outcomes at the preconception counseling visits to better educate and inform patients of their risks. Consideration should be made for antenatal testing and closer follow-up for high-risk women with prior pregnancies that were complicated by isolated elevated MSAFP and adverse outcomes, as this could indicate a likelihood of recurring elevated MSAFP and adverse outcomes.
Footnotes
Acknowledgments
The authors thank Karla D. Passalacqua, PhD, at Henry Ford Hospital for her editorial assistance and Stephanie Stebens, MLIS, at Sladen Library, Henry Ford Hospital, for her input in reviewing this article.
Authors' Contributions
M.A. contributed to original draft (lead), methodology (equal), formal analysis (lead), review, and editing (equal). M.K. was involved in methodology (equal), review, and editing (equal). J.R. was in charge of methodology (lead), review, and editing (equal). M.S. carried out conceptualization (lead), methodology (lead), review, and editing (equal).
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.