
Abstract
Objective:
The clinical value of an automatic chromosome harvester was evaluated, which included a comparison between the manual and automatic harvesting for the isolation of amniotic fluid cell chromosomes.
Methods:
Amniotic fluid samples from 96 high-risk gravida cases identified at 17-25 weeks treated at the Prenatal Diagnostic and Reproductive Center from June to July 2022 were collected. These samples underwent both manual and automatic chromosome collection, and their harvest time and number of amniotic cells were compared. These chromosomes were then used to produce karyotypic data for each sample using an automatic chromosomal karyotype analysis system, scan karyotype.
Results:
The average automatic harvesting time per sample, 3.92 min, was significantly lower than that of the manual harvesting, 7.89 min (p < 0.001). In addition, the average number of cells from the automatic harvesting (4.16 × 106 pieces) was significantly increased when compared with those of the manual group (2.10 × 106 pieces; p < 0.001). Further karyotyping revealed that both sets of chromosomes produced clear bands and good dispersion data, producing no significant differences in these evaluations (p > 0.05). However, the number of analyzable karyotypes obtained using the automatic harvester was significantly higher than those of the manual harvesting (p < 0.001).
Conclusions:
The automatic chromosome harvester can effectively save time, manual labor and consumables, harvest more analyzable karyotypes, and improve the efficiency of clinical diagnosis. The automatic chromosome harvester is highly stable and repeatable, which has the potential to help achieve large-scale standardized chromosome harvesting and is worthy of widespread clinical promotion.
Introduction
Karyotype analysis of amniotic fluid samples is critical in both prenatal diagnostics and clinically assisted reproduction, with these evaluations often acting as an important predictive method in prenatal diagnosis and the gold standard for detecting fetal chromosomal abnormalities (Fan et al., 2008; Li et al., 2019). At present, the harvesting of chromosomes from the amniotic fluid is still primarily facilitated through traditional manual harvesting methods, which suffer from various disadvantages, including being manpower and time intensive, producing low yields and exhibiting a high rate of operator errors, resulting in a reduction in diagnostic efficacy. In addition, these challenges mean that these methods suffer from limited systemization and standardization.
Therefore, we wanted to evaluate the use of automatic chromosome harvester, in an effort to improve both efficiency and experimental outcomes for these evaluations. The use of automation has other advantages over more traditional methods including the whole course automation, speed, and ease of operation allowing the effective processing of several amniotic fluid specimens at the same time. In this study, we used the amniotic fluid samples from 96 pregnant women admitted to our hospital with high-risk pregnancies from June to July 2022 to evaluate the application of automatic chromosomal harvesting in clinical management settings.
Materials and Methods
Specimen source
Our study used amniotic fluid samples from 96 high-risk gravida pregnancies identified at 17-25 weeks and treated in the Prenatal Diagnostic and Reproductive Center of the Second Affiliated Hospital of Anhui Medical University from June to July 2022. These samples were then evaluated based on various prenatal risk factors including high-risk maternal serum screening, abnormal noninvasive prenatal testing, family history of hereditary disease or chromosomal abnormalities, history of exposure to radioactive material or poisons, advanced maternal age, history of poor pregnancy and childbirth outcomes, and ultrasonographic abnormalities, among others.
Amniotic fluid collection
All samples were collected through needle aspiration, with the puncture site identified using ultrasound guidance. All interventions were completed under sterile conditions, and 20 mL of fluid was extracted from each patient and split into two 15 mL sterile centrifuge tubes.
Main instruments and equipment
Our experiments used an automatic chromosome harvester (IEXLLC, American), ultrasonic diagnostic instrument (GE, American), super clean bench (ThermoFisher, Warrington, UK), carbon dioxide incubator (ThermoFisher), low-speed centrifuge (USTC ZONKIA, Anhui, China), automatic chromosome drip meter (ADSTEC, Japan), automatic cell counter (JIMBIO, Jiangsu, China), and automatic chromosomal karyotype analysis system (ZEISS, Oberkochen, Germany).
Experimental materials and reagents
Our evaluations also required the use of amniotic cell medium (Dahui Biology, Guangzhou, China), 15 mL sterile centrifuge tubes (GeneBrick, North Carolina), 25 cm2 sterile cell culture flasks (Corning, New York), 0.25% Trypsin-ethylenediaminetetraacetic acid (EDTA) (Dahui Biology, Guangzhou, China), potassium chloride (KCl), sodium chloride solution (Double-Crane Pharmaceutical Industry in Anhui Province), methyl alcohol and acetic acid (MACKLIN, Shanghai, China), colchicine solution (Dahui Biology), Giemsa staining solution (Ruixinde, Tianjin, China), microscope slides (Citotest, Jiangsu, China), phosphate buffered solution (Solarbio, Beijing, China), and sheath fluid and cleaning solution (JIMBIO).
Experimental methods
Using the double-line culture method, the collected amniotic fluid samples were numbered 1-96 in chronological order and placed in groups of 24 samples leaving us a total of 4 groups. Then, the same sample was split into two lines (I and II). Once the culture was completed, the cells were digested using pancreatic enzyme digestion solution, and the I and II lines were then mixed and divided into two equal parts before the amniotic fluid cells in each sample were harvested through automatic and manual methods, respectively. We then recorded the time to chromosome harvest and then applied an automatic cell counter to count the number of harvested amniotic fluid cells captured through each method. Once complete, the chromosomes were sent through the automatic karyotype analysis system to create independent karyotype results.
Amniotic fluid cells culture
Amniotic fluid samples were centrifuged at 432 g for 10 min before the supernatant was discarded and the cells were resuspended in 5 mL of amniotic fluid cell medium. These cells were then placed into a culture flask and incubated in a 5% carbon dioxide incubator set to 37°C. Cells were allowed to grow for 7 days before the medium was changed and then left to culture for an additional 2-3 days.
Amniotic fluid cells chromosome harvesting and filming
We then went on to collect cells for chromosome harvesting by adding 20 μg/mL colchicine to the culture flask and incubating under growth conditions for another 3 h. Cell lines I and II were then digested with pancreatic enzyme digestion solution containing 0.25% EDTA, mixed, and evenly divided into two 15 mL centrifuge tubes, one for each of the harvesting methods.
Automatic chromosome harvesting
Cells were placed into the corresponding volumes of hypotonic (0.075 mol/L KCl) and fixative solutions (methanol-glacial acetic acid = 3:1) as determined by the number of specimens.
The harvesting process was then automatic and completed using an automatic chromosome harvester (model IDEX P7M) set to the following parameters: (1) hypotonic step, centrifugation of 360 s at 341 g, discarding of supernatant, discard level set to 15 mm, addition of 6.5 mL of hypotonic solution, shock mixing for 10 s (shock mode A, shock intensity 1500 rpm/min), low permeability time 15 min, low permeability medium shock mixing 10 s (shock intensity 1200 rpm/min), air bath temperature 37°C; (2) prefixation step, inject 1 mL of prefixative solution, shake well for 20 s (shock mode D, shock intensity 1200 rpm/min), stand for 5 min, centrifuge at 341 g for 360 s; (3) fixation step, complete three times, discard supernatant, discard level set to 15/13/11 mm, inject the fixative solution, volume set to 6/6/1 mL, stand for 10 min after the first fixation, shock mix for 20/20/0 s (shock mode A, shock intensity 1200 rpm/min), and centrifuge at 341 g for 360/360/0 s, respectively. Remove the specimens at the end of harvesting, mix them well, and store them at 4°C.
Manual chromosome harvesting
Samples were taken, centrifuged at 432 g for 10 min, supernatant discarded, added 6.5 mL hypotonic solution (0.075 mol/L KCl prewarmed to 37°C), repeatedly blowing and mixing in a 37°C water bath for 15 min, added 1 mL fixative solution (methanol-glacial acetic acid = 3:1) mixed thoroughly, then pipetted up and down, and allowed to return to room temperature for prefixation.
Samples were centrifuged at 432 g for 10 min, supernatant was discarded, fixative solution added, 6 mL upside down, mixed well, and left at room temperature for 10 min, then the supernatant was centrifuged and discarded. The fixation steps were repeated once more, 1-2 mL of the fresh fixative solution was added to the cell pellet at the bottom of the centrifuge tube, gently pipetted and mixed. Then, samples were stored at 4°C.
Drops and staining
The stored samples were taken, centrifuged at 432 g for 10 min, the supernatant was discarded and then freshly formulated fixative solution was added, resuspended, and mixed well to create a homogeneous cell suspension. The cell suspension was placed into an automatic chromosome drip meter for tableting. One slide per sample was dropped, two drops per slide, 20 μL per drop. All specimens were then aged at 85°C for 3 h, treated with 0.005% trypsin for 2 min, and then subjected to Giemsa staining. Karyotyping results were analyzed with reference to the International System for Human Cytogenetic Nomenclature (McGowan-Jordan et al., 2016).
Statistical analysis
All evaluations were completed in GraphPad Prism 8, with all measurements, including harvest time and number of harvested cells, expressed as
Results
Automatic harvesting significantly reduces overall processing time
Given the fact that processing time is often a critical factor in clinical applications, we decided to compare the total time required to harvest samples using each of the two processing methods described above. We then used this information to calculate the average time required to harvest a single sample and then compared these values. Our data revealed that the average time required to harvest a single sample when using a fully automatic process was 3.92 min, while the average processing time for manual extraction was 7.89 min, clearly demonstrating that automatic harvesting required significantly less time per sample. Further evaluation revealed that automatic methods reduced processing time by nearly 50%, and paired t-test confirmed that these differences were statistically significant (t = 18.95, p = 0.0003, p < 0.05; Table 1).
Comparison of the Average Time Required to Process Single Amniotic Fluid Cell Samples By Automatic and Manual Harvesting
Note: 24 samples per group.
Automatic harvesting produces significantly more cell volume than manual harvesting
Amniotic fluid samples were arranged in chronological order and the volume of their precipitates was compared. These comparisons revealed that the volume of the amniotic fluid cells mass obtained using automatic harvesting was significantly larger than that of manual harvesting (Fig. 1). This observation was validated by the fact that there were significantly more amniocytes harvested through the automatic method, 4.16 × 106 pieces on average versus 2.10 × 106 pieces on average. Wilcoxon paired signed rank test (p < 0.001) revealed that these differences were statistically significant, and when taken together, these data suggest that the automatic harvesting was significantly more efficient than the manual harvesting (Fig. 2).
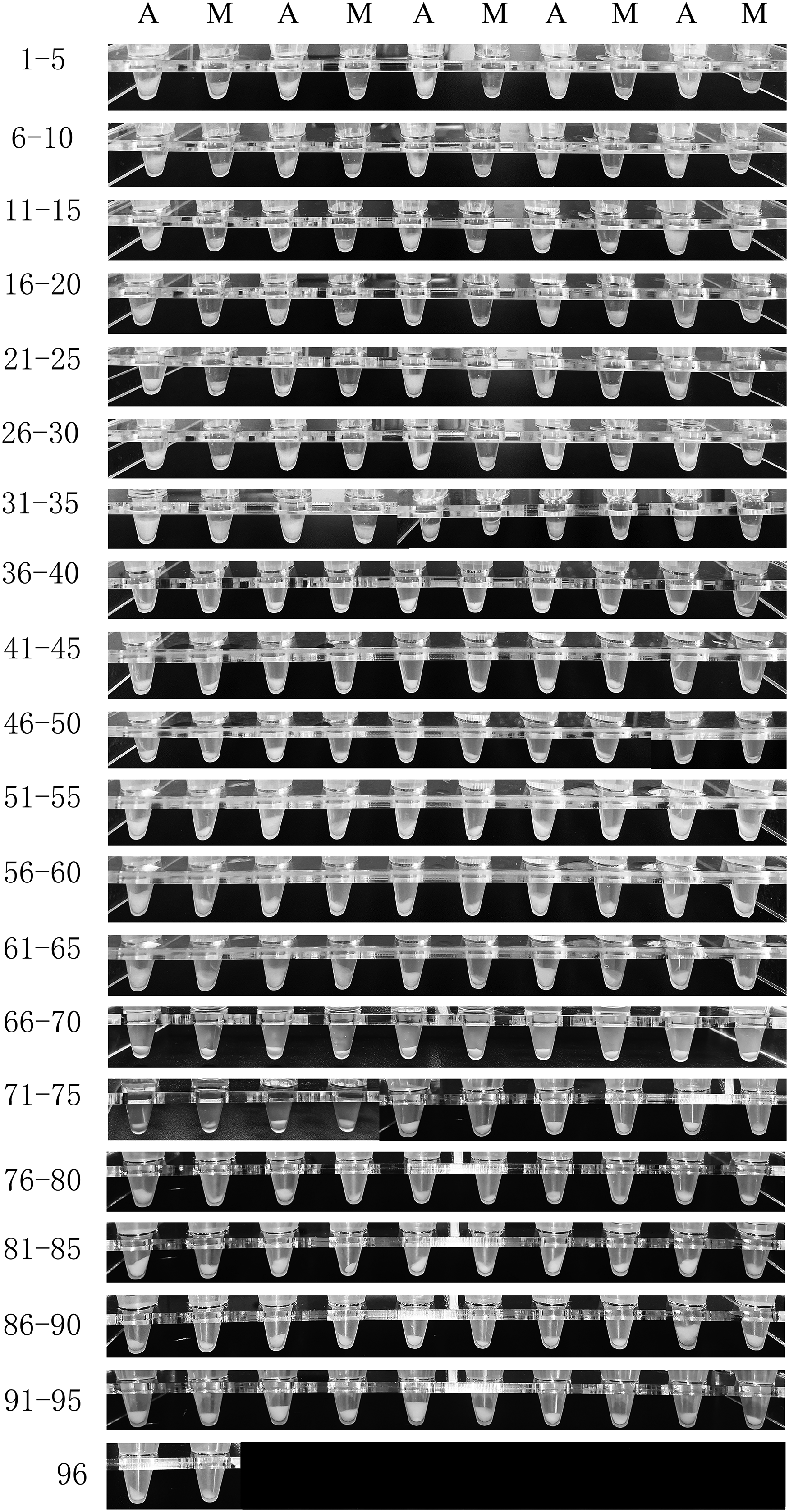
Comparison of the sedimentation volumes for amniotic fluid cells obtained by automatic and manual harvesting. A, automatic harvesting; M, manual harvesting.
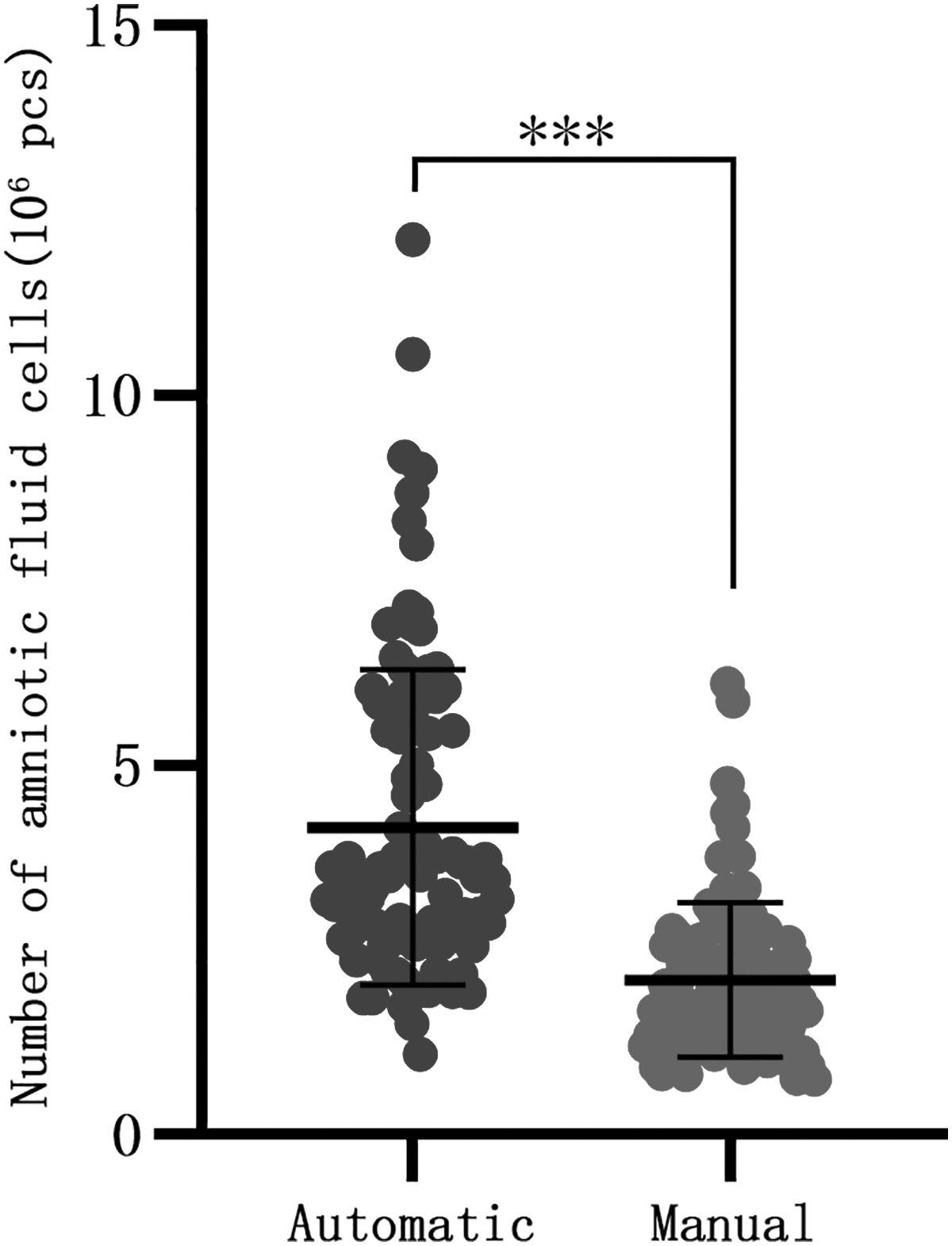
Comparison of the number of amniotic fluid cells obtained by automatic and manual harvesting. ***p < 0.001.
Automatic harvesting produces more analyzable karyotypes than manual harvesting
After droppings and staining, the harvested karyotypes were observed under a microscope (Fig. 3). We then relied on evaluations of the nuclear band standard in the guidelines and the degree of chromosome dispersion to determine karyotype quality. This method allowed us to divide our data into three categories, facilitating the enumeration of metaphase chromosomes: Type I: unanalyzable, <320 bands; Type II: analyzable, 320-400 bands; Type III: analyzable, ≥400 bands.

Comparison of the karyotype quality obtained by automatic and manual harvesting, as visualized through light microscopy.
The results showed that a total of 192 slides and 12,473 karyotypes were prepared by the 2 harvesting methods, including 6651 karyotypes obtained by automatic harvesting and 5822 karyotypes obtained by manual harvesting. Among the karyotypes obtained by automatic harvesting, Type II: 2977 (44.8%), Type III: 1391 (20.9%); among the karyotypes obtained by manual harvesting, Type II: 2671 (45.9%), Type III: 1135 (19.5%); according to the χ2 test, there was no significant difference in the percentage of analyzable karyotypes at Types II and III levels obtained by the two methods (χ2 = 4.025, p = 0.134, p > 0.05; Table 2).
Comparison of Analyzable Karyotype Rates Obtained By Automatic and Manual Harvesting
Note: χ2 = 4.025, p = 0.134, p > 0.05, the difference was not statistically significant.
However, because the total number of karyotypes obtained by automatic harvesting is more than those obtained by manual harvesting, the number of analyzable karyotypes obtained by automatic harvesting is more than those obtained by manual harvesting, and the difference was statistically significant after the t-test, Type II (320-400 bands): t = 3.88, p = 0.0002; Type III (≥400 bands): t = 4.25, p < 0.0001; the sum of Types II and III (≥320 bands): t = 5.43, p < 0.0001, p < 0.05 (Fig. 4).
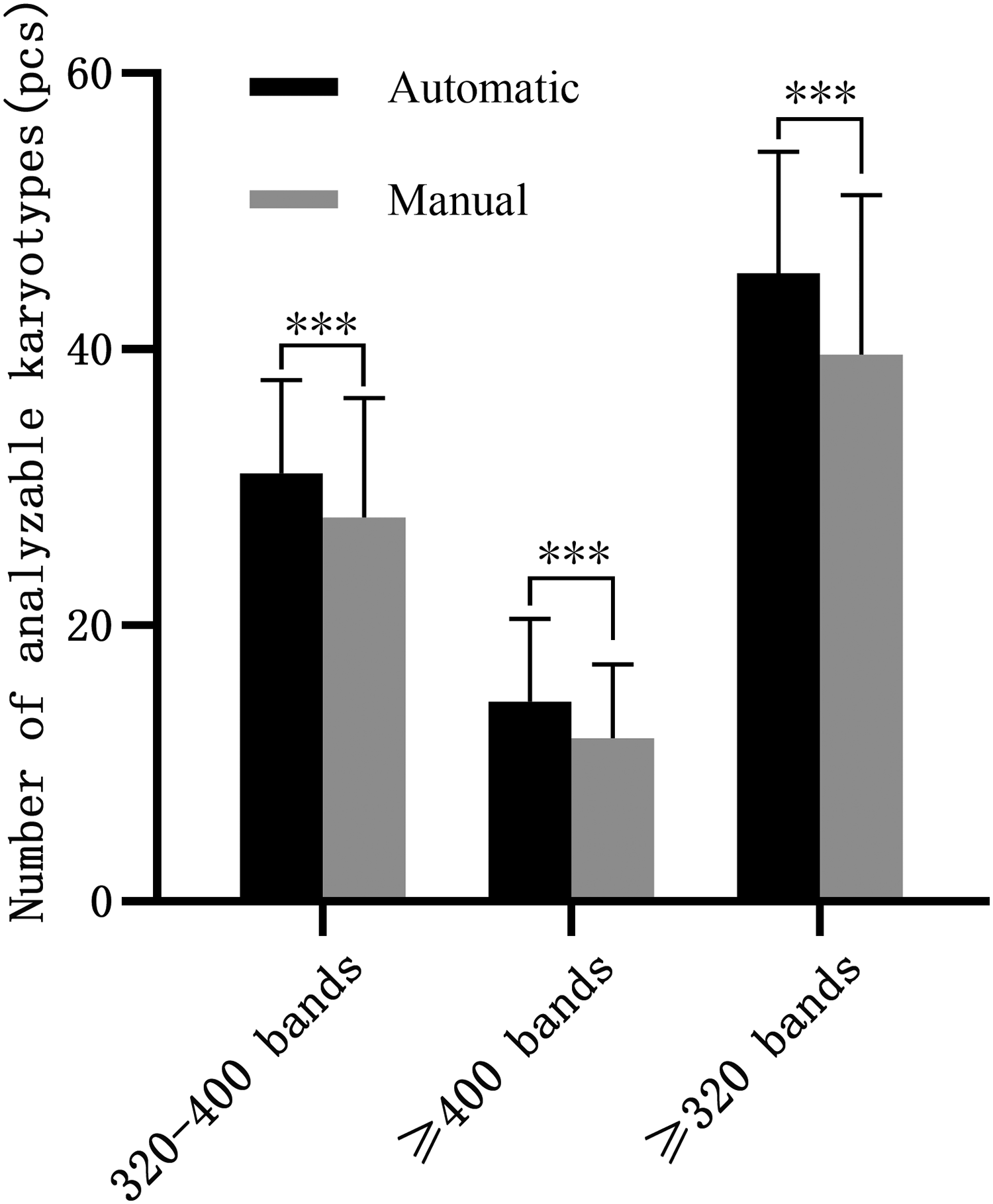
Comparison of the number of analyzable karyotypes obtained by automatic and manual harvesting. Note: 320-400 bands: t = 3.88, p = 0.0002; ≥400 bands: t = 4.25, p < 0.0001; ≥320 bands: t = 5.43, p < 0.0001; ***p < 0.001.
Thus, we can conclude that although the automatic chromosome harvesting did not produce a higher percentage of analyzable karyotypes, the number of analyzable karyotypes harvested was significantly increased in these samples, which may in turn help to reduce diagnostic complexity, improving the diagnostic efficiency.
Discussion
Advanced maternal age (Zhang et al., 2022), recurrent miscarriage (van Dijk et al., 2020), birth defects (Hvide et al., 2021), and various hereditary disorders (Stone and Reed, 2020) seriously endanger children's survival, health, and quality of life, placing a heavy burden on society and families. The main reason for the above factors to harm children is chromosomal abnormalities (Liu et al., 2020; Mikwar et al., 2020). This means that it is crucial that effective prenatal diagnosis of high-risk pregnancies helps to reduce miscarriage and birth defect rates.
Karyotyping of amniotic fluid cells remains an important means of prenatal diagnosis, and assisted reproduction often helping to identify potential fetal chromosomal abnormalities and improve eugenics and fertility (Fan et al., 2008; Li et al., 2019). In fact, some scholars believe that screening for chromosomal abnormalities should be common practice regardless of parental age (ACOG Committee on Practice Bulletins, 2007).
Irrespective of this viewpoint, karyotyping of amniotic fluid cells requires the development of high-quality amniotic fluid cell culture and harvesting. We observed that the automatic chromosome harvester not only saved time, but also improved the efficiency of chromosome harvest in amniotic fluid samples. For now, the automatic chromosome harvesters are expensive, their superiority is not recognized, and not needed by laboratories with fewer specimens. Therefore, their applications have not been widespread in diagnostics laboratories today.
This study found that the application of an automatic chromosome harvester significantly shortened the time required for harvesting and saved on both labor and reagent costs. The manual process of harvesting chromosomes is cumbersome and requires experienced employees to complete, and manual operation cannot work as continuously, uninterruptedly, or as quickly as a machine. In addition, continuous manual operation will eventually result in fatigue, further reducing the speed of the operator.
Comparisons of the experimental process also reveal that the use of an automatic chromosome harvester dramatically simplifies the complex manual operation steps, making it easier to learn and increasing repeatability. These methods are also highly stable and reduce the novice stage effects. Taking a single harvest of 24 samples as an example, it takes 1.56 h for automatic harvesting and 3.16 h for manual harvesting, and automatic harvesting saves ∼50% of the time. If it runs 8 h a day, the automatic harvester can operate two times and harvest 64 samples each time for a total of 128 samples.
However, only ∼64 samples can be harvested by manual harvesting in the same period. Increased throughput capacity also means that this method is more suited to harvesting a large number of samples, effectively eliminating many of the obstacles for this kind of evaluation. In addition, the automatic chromosome harvester can be completely unattended, and the staff can do more other work during this time when it runs. Furthermore, in a laboratory with a large number of specimens, an automatic chromosome harvester can perfectly play its advantages, but in a laboratory with fewer specimens, these advantages may be limited.
We also found that although automatic chromosome harvesting did not obtain a higher percentage of analyzable karyotypes, the number of analyzable karyotypes harvested in these samples increased significantly due to a significant increase in the number of amniotic fluid cells obtained and the total karyotype. Subsequent literature review revealed that there are many possible reasons for these outcomes with most supporting a difference in operational hypotonic time, fixed time, or blowing force as the major cause for these differences (Bangs and Donlon, 2005; Bayani and Squire, 2004).
Hypotonic and fixation steps are essential for metaphase chromosome preparation with good distribution and clear bands. The main effect of hypotonicity is swelling of amniotic fluid cells, unwinding of chromosomes in metaphase, and moving chromosomes from the central position of the cell to a more peripheral position, which is conducive to the dispersion of chromosomes (Claussen et al., 2002; Rønne, 1989). The role of the fixative is to rapidly permeate cells to denature nuclear proteins and preserve chromosomal structure (Rønne, 1989).
Manual harvesting is impossible to accurately control hypotonic time, fixed time, and blowing force, which can be extremely reliant on personal experience. In addition, the literature suggests that a shorter hypotonic time limits chromosomal spread, but a longer hypotonic time increases chromosomal expansion and lead to chromosomal band blurring, which affects interpretation (Bayani and Squire, 2004). Too much blowing or too long in the hypotonic solution can also lead to cell rupture and chromosome loss, whereas if the fixation time is too short, the chromosomal morphology will begin to blur.
In contrast, if the fixation solution is added too quickly, mixed too quickly, or blown too hard, the cells can fragment, the chromosomes can be lost, and there can be both distortion and deformation of the karyotype (Bangs and Donlon, 2005; Bayani and Squire, 2004). Given this, it makes sense that automatic harvesting where all of these parameters are preset and consistently applied ultimately provides more reproducible outcomes and improved clinical diagnosis.
Automation has been applied to many clinical departments with its advantages of high efficiency, standardization, and reduced error rates, making it an obvious choice in diagnosis and management (Buonanno et al., 2023; Lemieux et al., 2023; Tan et al., 2023). We believe that widespread adoption of the automatic chromosome harvester would facilitate improved diagnostic outcomes and may serve to support the implementation of systematic and standardized amniotic fluid cell chromosome harvesting. We also believe that automatic harvesting will eventually replace all manual harvesting in clinical practice.
Footnotes
Authors' Contributions
Y.W. was involved in the design of the study, acquisition of data, statistical analysis, and writing and revision of articles. Y.F. was involved in the acquisition of data and statistical analysis. C.M. and J.Z. helped with performing part of the experiments and statistical analysis. S.S. was involved in the design of the study, funding acquisition, and revised the article. All authors read and approved the final article as submitted.
Ethical Approval
The study was conducted following all guidelines laid by Declaration of Helsinki. All specimens were obtained with written informed consent, and this study was approved by the ethics committee of the Second Affiliated Hospital of Anhui Medical University, ethics batch number YX2022-034 (F1).
Author Disclosure Statement
The authors state no conflicts of interest regarding this study.
Funding Information
This research was supported by National Natural Science Foundation of China (Grant No. 81801511).