
Abstract
Background:
Spinal muscular atrophy (SMA) is an autosomal recessive neuromuscular life-threatening disorder. Owing to high carrier frequency, population-wide SMA screening to quantify the copy number of SMN gene is recommended by American College of Medical Genetics and Genomics. An accurate, reliable, short runaround time and cost-effective method may be helpful in mass population screening for SMA.
Methods:
Multiplex ligation-dependent probe amplification (MLPA) is a gold standard to estimate the copy number variation (CNV) for SMN1 and SMN2 genes. In this study, we validated droplet digital polymerase chain reaction (ddPCR) for the determination of CNV for both SMN1 and SMN2 exon 7 for a diagnostic purpose. In total, 66 clinical samples were tested using ddPCR, and results were compared with the MLPA as a reference test.
Results:
For all samples, CNV for SMN1 and SMN2 exon 7 was consentaneous between ddPCR and MLPA test results (κ = 1.000, p < 0.0001). In addition, ddPCR also showed a significant acceptable degree of test repeatability, coefficient of variation < 4%.
Conclusion:
ddPCR is expected to be utilitarian for CNV detection for carrier screening and diagnosis of SMA. ddPCR test results for CNV detection for SMN1/SMN2 exon 7 are concordant with the gold standard. ddPCR is a more cost-effective and time-saving diagnostic test for SMA than MLPA. Furthermore, it can be used for population-wide carrier screening for SMA.
Introduction
Spinal muscular atrophy (SMA) is a neuromuscular disorder caused by the loss of motor neurons in the anterior horn of the spinal cord and brain stem nuclei. Genetically, SMA follows autosomal recessive pattern of inheritance caused by disruption in the survival motor neuron (SMN1) gene. Clinical SMA type is apprized by the age of onset and severity of the muscle weakness. Approximately, 1 in 6,000-10,000 live births is diagnosed with SMA, and carrier frequency is 1:51, globally (Sugarman et al., 2012). According to the age-related motor development, SMA is broadly classified into the following three classes: type I (never sit), type II (never walk unaided), and type III (independent walking ability). As per the research evidence, major clinical diagnostic categories in genetically confirmed SMA cases are (i) presymptomatic SMA, (ii) SMA type 0/Ia, (iii) SMA type Ib, (iv) SMA type Ic, (v) SMA type IIa, (vi) SMA type IIb, (vii) SMA type IIc, (viii) SMA type IIIa, (ix) SMA type IIIb, (x) SMA type IV, and (xi) SMA type minimal manifestation (Calucho et al., 2018; Cuscó et al., 2020; Talbot and Tizzano, 2017; Tizzano, 2019). Independent of the clinical severity, all classes of SMA are due to the loss of function of SMN1 gene located at chromosome position 5q13.
A nondiseased individual has at least one active copy of SMN1 gene. Approximately, 95% of patients with SMA have homozygous deletion of exon 7 in SMN1 gene, whereas the remaining 5% of patients harbor a compound heterozygous mutation, which can be missense, nonsense, or frameshift [pathogenic point mutation in SMN1 gene on one chromosome and SMN1 gene deletion in the other (Wirth, 2000)]. The two SMN genes, SMN1 and SMN2, are highly homologous to each other, with the only difference at five base pairs. Owing to only a single base difference in the coding region in exon 7 (NM_000344.3:c840C > T, rs1164325688) (https://www.ncbi.nlm.nih.gov/snp/), there is an inefficient SMN2 exon 7 splicing and production of the predominantly nonfunctional SMN protein (Singh and Singh, 2018).
The number of SMN2 copies determines the severity of the SMA phenotype (Cuscó et al., 2020), which is inversely associated with disease severity. SMN1 and SMN2 copy number alterations can be determined using different techniques such as real-time polymerase chain reaction (PCR) (TaqMan Platform), real-time PCR (LightCycler Platform), multiplex ligation-dependent probe amplification (MLPA), AmplideX PCR-CE, digital PCR, and next-generation sequencing (NGS). However, all these methodologies have their own advantages and limitations (Arkblad et al., 2006; Cavdarli et al., 2020; Feldkötter et al., 2002; Gómez-Curet et al., 2007; Tan et al., 2020).
MLPA is a gold standard test for detection of copy number variation (CNV) in SMN gene. MLPA, being a quantitative assay, requires normalization of results, and thus, control samples are required. Designing and validation of probes for MLPA remains a big challenge and has a complex assay run, which requires at least 48-73 h (Arkblad et al., 2006).
Droplet digital polymerase chain reaction (ddPCR) is a sensitive, cost-effective, and less complex test procedure. It is a quantitative assay that requires a low concentration of DNA. DNA is split into thousands of nanoliter-sized droplets, each having an independent amplification process (Shekhawat et al., 2021; Vidal-Folch et al., 2018). The concentration of the target gene in the sample is determined from the fraction of the droplet that has fluorescence signal. The Poisson algorithm is used to calculate the fraction of the positive droplet (presence of gene of interest), and no standard curve is required for an absolute quantification of the target gene (Prior and Nagan, 2016). The objective of the present study is to validate the execution of ddPCR for the determination of copy number alteration of the exon 7 of SMN1/SMN2 genes using different clinical samples and the application of ddPCR as an alternative cost-effective and time-saving diagnostic test for SMA.
Methodology
Patients and blood sample
The study protocol was approved by the Institutional Ethical Committee of All India Institute of Medical Sciences, Jodhpur, Rajasthan, India. Informed consent was obtained from the participants. Study duration was from April 2020 to July 2022. Clinical detail of the proband was collected; the spectrum is given in Table 1. Ethylenediaminetetraacetic acid blood samples (3 mL) of the patient suspected with SMA (index case, n = 22) and their parents (n = 44) were collected as per clinical and laboratory standards. Genomic DNA (gDNA) was isolated (peripheral blood, n = 65; fetus tissue, n = 1) using silica resin/column-based DNA isolation kits (Qiagen). gDNA quantity (ng/uL) was measured by a fluorimeter (Qbit), and quality (A260/A280) was estimated using a NanoDrop (Thermo Fisher) spectrophotometer.
Clinical Spectrum of Tested Samples
EDTA, ethylenediaminetetraacetic acid; GA, gestational age; SMA, spinal muscular atrophy.
ddPCR assay workflow
The ddPCR test was performed on a QX200™ Droplet Digital™ PCR System (Bio-Rad Laboratories). For each well, the final reaction volume was 20 μL containing 2xddPCR super mix for probe, primer, SMN1/SMN2 duplex assay (reference gene: RPP30), restriction enzyme HaeIII (10U/μL), and DNA template. Final concentration of DNA was 35 ng/μL. Nanoliter-sized droplet generation was carried through the addition of 20 μL of the reaction mixture and 70 μL of droplet generation oil. The oil emulsion (droplet, volume 40 μL) was then transferred to a ddPCR 96-well semi-skirted plate. After that plate was sealed using PX1 PCR plate sealer (PX1 Bio-Rad), endpoint PCR was performed, using deep-well PCR (CFX96 Touch™ Deep Well Real-Time PCR). The PCR cycle’s protocol was as per the manufacture guideline (enzyme activation at 95°C for 10 min, denaturation at 94°C for 30 s, annealing and extension at 58°C for 1 min, enzyme deactivation at 98°C for 10 min, and 40 cycles of denaturation and annealing/extension).
After gene amplification, the microfluidic droplet reader (QX200 Bio-Rad) was used for the absolute quantification of amplified product in form of fluorescent positive and negative droplets. Positive droplet contains at least one copy of the target DNA molecule. To classify the droplet cluster and Poisson algorithm application for the absolute quantification of SMN1, SMN2, and RPP30 gene copies, a QuantaSoft Analysis Pro version 1.7.4.0917 was used.
QuantaSoft measures the copy numbers of SMN1 and SMN2 exon 7 by multiplying the fluorescent ratio between the target and the reference gene. RPP30 gene was used as a reference gene. In ddPCR data from a duplex test, targeted amplicon was plotted in a two-dimensional plot in which channel 1 fluorescence (6-Carboxyfluorescein) was plotted against channel 2 fluorescence (Hexachloro-fluorescein) for each droplet. Three controls (CNV0, CNV1, and CNV2 copies for SMN1 and CNV2, CNV3, and CNV4 for SMN2) and no template control were tested in each batch.
Test accuracy performance
For evaluation of the accuracy of the ddPCR test results, MLPA was used as a reference standard. MLPA testing for all index cases was performed from outsourcing. P021 probemix (MRC Holland) was used to access the SMN1/SMN2 CNV. The MLPA test was performed as per the kit instructions. Briefly, denatured at 98°C for 5 min followed by hybridization with the probe overnight at 60°C. The ligation reaction was performed at 54°C for 15 min using ligase-65 enzyme, followed by 5 min of heat inactivation of the enzyme at 98°C. After that, PCR amplification was done using Deep Well Real-Time PCR (CFX96 Touch Bio-Rad). A 24-capillary Sanger sequencer (3500xL Applied Biosystems) was used for fragment analysis followed by data analysis using GeneMarker software (SoftGenetics).
Test precision
Ten samples were used with 0, 1, and 2 copy numbers for SMN1 exon 7 and 0, 1, 2, 3, and 4 copy numbers for SMN2 exon 7. The test was examined in three batches to estimate between-run precision of ddPCR.
Statistical analysis
ddPCR test precision was calculated in mean, standard deviation, and coefficient of variant (CV). Performances of MLPA and ddPCR test results were compared using weighted K statistics. Class of accuracy of K statistics was classified as follows: 0.81-1.0, perfect; 0.61-0.80, good; 0.41-0.60, moderate; 0.21-0.40, weak; and <0.20, poor. In addition, p < 0.05 was considered significant. Statistical data were analyzed using the Statistical Package for the Social Sciences for Windows version 21.
Results
In ddPCR reaction, the average total number of droplets generated per reaction was 16,952 (range, 2,623-21,920). As results (n = 66) for SMN1 gene, 12, 16, and 38 patients had 0 copy, 1 copy, and 2 copies, respectively. For SMN2 gene 5, 34, 16, and 1 patients had 1 copy, 2 copy, 3 copies, and 4 copies respectively (Table 2). For all index cases (n = 22), the copy number of SMN1 and SMN2 exon 7 was concordant between MLPA and ddPCR (Table 3).
ddPCR Test Results for Copy Number Alteration for SMN1 and SMN2 Exon 7 (N = 66)
ddPCR, droplet digital polymerase chain reaction; SMA, spinal muscular atrophy.
Comparison between ddPCR and MLPA Results for CNV of SMN1 and SMN2 Exon 7 (N = 22)
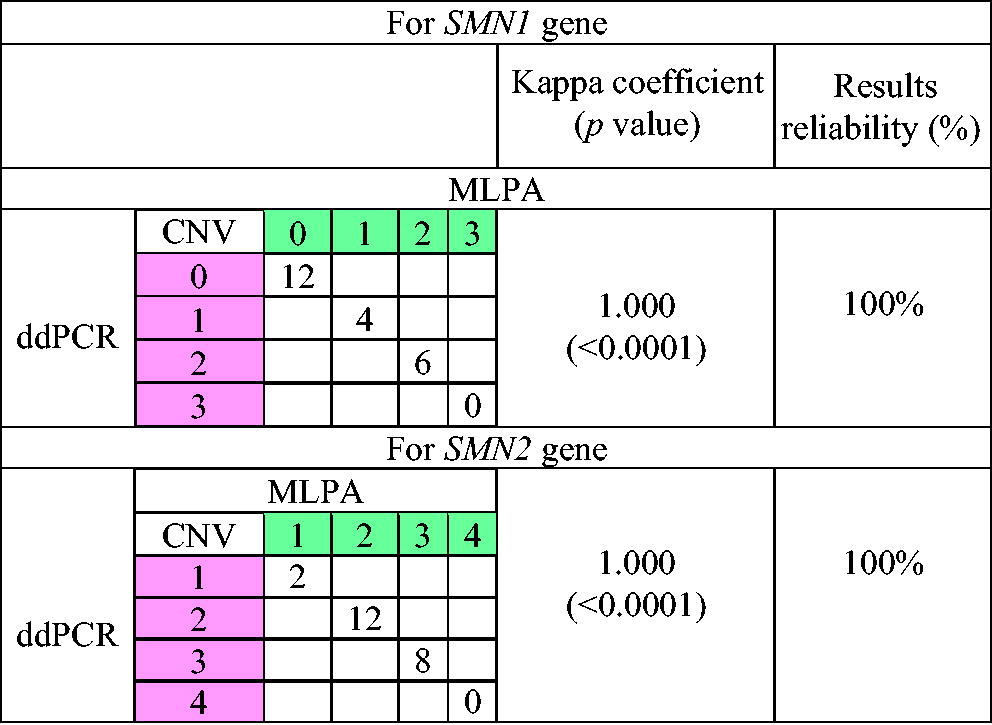
p < 0.05 was considered significant.
CNV, copy number variation; ddPCR, droplet digital polymerase chain reaction; MLPA, multiplex ligation-dependent probe amplification.
Comparisons of MLPA and ddPCR test results were significant for SMN1 and SMN2 genes. Kappa coefficient was 1.000, and p value was <0.0001 for both SMN1 and SMN2 exon 7. The percentage of data that was reliable for ddPCR test results in comparison to MLPA was 100% for all CNV in both SMN1 and SMN2 exon 7. ddPCR test repeatability showed a CV < 4% for CNV in SMN1 and SMN2 exon 7. These details are described in Table 4.
Repeatability of ddPCR Test for CNV Detection
CNV, copy number variation; CV, coefficient of variation; ddPCR, droplet digital polymerase chain reaction; SD, standard deviation.
Time frame and cost per test for MLPA versus ddPCR
MLPA is a complex, long turnaround time assay. The whole process (DNA isolation to MLPA test result interpretation) required 72-90 h, whereas the complete ddPCR test procedure does not require more than 8 h. These details are described in Table 5.
MLPA Versus ddPCR Test Procedure and Cost per Test
ddPCR, droplet digital polymerase chain reaction; MLPA, multiplex ligation-dependent probe amplification; PCR, polymerase chain reaction.
Discussion
In this study, we describe the detection of copy number alteration in SMN1/SMN2 gene using ddPCR. MLPA test results were used as a reference method to validate the ddPCR results. The ddPCR approach is a sensitive method and has a very low chance of false-positive results because during the test, we observed ≥5,000 positive droplets for each target and reference amplicon.
In the present study, the ddPCR assay showed perfect agreement with MLPA for the determination of CNV in both SMN1 and SMN2 exon 7. Moreover, the precision performance of ddPCR was very good for determining the copy numbers of SMN1 and SMN2 in this study. Park et al. also support our finding (Park et al., 2020). Interpretation of the test results is more definite with ddPCR compared with MLPA because CV of the fluorescent ratio between the target and the reference gene could be obtained by dividing the copy number by 2.
Advancement in the characterization of the genetic makeup of SMA has enabled rapid development in the targeted therapy. Currently, three Food and Drug Administration-approved drugs are available with the medical community. For example, first, nusinersen (Spinraza, Biogen Cambridge) is a 2′-O-methoxyethyl phosphorothioate-modified drug that modulates alteration of the SMN2 pre-RNA splicing process by inhibiting the splicing factors. Spinraza targeting antisense oligonucleotide therapy is used for both adults and children (Food and Drug Administration, 2016). Second, Onasemnogene abeparvovec-xioi (Zolgensma, Novartis) is an adeno-associated virus vector-based gene therapy for use in patients younger than 2 years of age (Food and Drug Administration, 2019). Third, risdiplam (Evrysdi, Roche) modifies SMN2 pre-mRNA splicing and is used for patients with SMA who are 2 months and older (Baranello et al., 2021). These available therapies have driven a demand for increasingly more reliable, rapid, and cost-effective diagnostic tests.
There are various methods available to detect CNV in SMN1/SMN2 gene. NGS is the most popular test of sequence analysis nowadays. However, NGS test procedure is complex and laborious and has a long turnaround time (2-3 weeks), and the interpretation of results requires specialized bioinformatics tools. All these make NGS testing very expensive. In India, private laboratories charge $70-90 for exon sequencing of SMN1/SMN2 gene. MLPA is also not cost-effective (charge $40-45), and the test has a complex workflow that goes up to 3-4 days. MLPA requires a control sample to normalize the results, and the test is not available in most of diagnostic laboratories because of the requirement of advanced equipment. That can be challenging to execute mass population screening for SMA.
Owing to the complex test protocol, high cost, and long turnaround time of MLPA and NGS, there is a need to develop an alternative method. We have validated the determination of CNV using the ddPCR platform, which has a good result accuracy as MLPA (Table 3) with very good test reliability (CV < 4%). It is also a very less time-consuming test (6-8 h), and the result interpretation does not require the usage of any complex bioinformatics tools. The test run cost of ddPCR being less than $8 proves to be a cost-effective technique. Our data suggest that ddPCR assay for the determination of CNV of SMN1/SMN2 gene is simple, affordable, robust, and time-saving. These details are described in Table 5.
ddPCR exhibits proficiency in discerning the copy number of exon 7 within the SMN1 gene. Nonetheless, prevailing dosage testing methodologies encounter challenges in accurately phasing alleles, a pivotal consideration for distinguishing individuals with the standard SMN1 genes on both alleles (1 + 1) from silent carriers (2 + 0). Silent carriers harbor two SMN1 copies on one chromosome and lack any copies on the other, emphasizing the need for improved phasing capabilities in genetic assessments.
Furthermore, beyond the widely recognized pathogenic variant involving the loss of c.840C in SMN1, there exist additional pathogenic variants that elude detection through current methodologies. These undetected variants contribute to the genetic complexity associated with SMN1, underscoring the necessity for refined diagnostic approaches to comprehensively identify and characterize the spectrum of pathogenic alterations in the SMN1 gene. A precise sequencing of extended DNA fragments (long-read sequencing) is ideal for resolving areas characterized by significant sequence similarity (Chen et al., 2023).
SMA is a complex disease condition requiring detailed knowledge on the public and the clinician (Carré and Empey, 2016; Moultrie et al., 2016). Owing to high carrier frequency of SMA, there are high chances of a child being born with a homozygous deletion of exon 7 in SMN1 gene. This has a very serious clinical implication, and the treatment for the same becomes a concern as it is highly expensive and not affordable by the general population. Therefore, the American College of Medical Genetics and Genomics’ guidelines recommend population-based genetic screening for SMA (Prior, 2008), and the American College of Obstetricians and Gynecology recommends DNA testing for SMA in all couples seeking preconception or prenatal care (Anonymous, 2017).
In the present study, we tested CNV for SMN1/SMN2 gene in the proband and their first-degree relatives using ddPCR, which proved to be a reliable molecular test with high specificity and sensitivity besides being rapid and cost-effective. This test can thus provide important prognostic and diagnostic information that can be used for SMA prevention and treatment.
Conclusion
CNV determination for exon 7 of SMN1/SMN2 using ddPCR showed acceptable test results. Its performance showed excellent agreement with the gold standard test, MLPA. ddPCR is a reliable, cost-effective, and short-time assay; therefore, it is expected to be useful for diagnosis and mass screening of newborns and pregnant women for carrier detection of SMN1/SMN2 gene and prevention of homozygous birth.
Footnotes
Acknowledgments
The authors thank all colleagues for their confidence, information, and reference of the patients for the study.
Authors’ Contributions
D.S.S. designed and conducted experiments and analyzed the data. D.S.S., S.D., S.G.D., and P.S. wrote the original article. K.S. conceptualized and wrote the original draft.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research study was supported by a grant from the Department of Biotechnology, Government of India (BT/NIDAN/03/05/2018).