
Abstract
Background:
At present, numerous clinical studies suggest a correlation between inflammatory bowel disease (IBD) and skin cancer. However, some articles present differing views that IBD does not increase the risk of skin cancer. The presence of potential reverse causality and residual confounding is inherent in conventional observational studies. Thus, this study used a two-sample Mendelian randomization (MR) study design to estimate the causal effect of IBD on the risk of skin cancer, including cutaneous malignant melanoma (CMM, also named melanoma skin cancer) and nonmelanoma skin cancer (NMSC).
Design:
In this study, a two-sample MR analysis was used to estimate the causal effect of IBD on skin cancer outcomes. The inverse-variance weighted (IVW) method was used as the main MR analysis, with multiple sensitivity analyses conducted to assess the robustness of findings.
Results
: In examining the association between IBD and NMSC, all p-values of the IVW methods were found to be <0.05, providing evidence for a causal effect of IBD on an increased risk of NMSC. However, IVW for IBD on CMM yielded p-values >0.05, indicating no causal relationship between IBD and CMM. These findings were consistent across other MR methods, with no evidence of pleiotropy or heterogeneity. Sensitivity analyses confirmed the robustness of our results.
Conclusion:
Using MR analysis, we found evidence for a causal effect of genetic liability for IBD on an increased risk of NMSC. However, our study did not find sufficient evidence to support a significant impact of IBD on CMM outcomes.
Introduction
Inflammatory bowel disease (IBD), encompassing Crohn's disease and ulcerative colitis, is a chronic immune-mediated disorder characterized by relapsing symptoms and variable clinical course, currently lacking curative interventions (Torres et al., 2017; Ungaro et al., 2017). The natural course of IBD, characterized by low mortality and improved survival rates, has led to an increased number of the disease (Hodson, 2016; Malik, 2015). According to a study covering 195 countries and territories, the global prevalence of IBD increased, and as of 2017, there were ∼3.9 million women and ∼3.0 million men living with this condition worldwide (2020).
Although gastrointestinal symptoms are the most prevalent in IBD, the disease's impact extends beyond the digestive system with some patients experiencing extraintestinal manifestations such as peripheral arthropathy, erythema nodosum, aphthous stomatitis, episcleritis, sweet syndrome, and so on (Garber and Regueiro, 2019). Numerous studies have been conducted to investigate the association between IBD and cancer, with particular emphasis on exploring the correlation between IBD and cutaneous malignancies (Cheng et al., 2023; Rajamäki et al., 2021).
The classification of skin cancer commonly encompasses cutaneous malignant melanoma (CMM, also referred to as melanoma skin cancer) and nonmelanoma skin cancer (NMSC), with the latter comprising basal cell carcinoma and squamous cell carcinoma as the predominant subtypes (Gordon, 2013; Perez et al., 2022). According to the global cancer statistics in 2018, the estimated number of newly diagnosed NMSC cases in the world was 1,042,056, accounting for the fifth new incidence rate of cancer (Bray et al., 2018). CMM increased the number of cases by 287,723, ranking in the middle (Bray et al., 2018). From the study of Global Cancer Statistics 2020, the ranking of new cases in NMSC has risen to the fourth place in research, and the number of new cases in CMM has also increased (Sung et al., 2021).
NMSC had a high incidence rate in North America, Australia, and New Zealand, resulting in an increase in social and family economic burden (Bray et al., 2018). Nevertheless, early detection of skin cancer can lead to effective treatment and lower mortality rates, and there is an urgent need to work together to identify the risk factors that lead to skin cancer for early prevention and intervention (Arivazhagan et al., 2022; Kornek and Augustin, 2013).
Some studies have found a correlation between IBD and skin cancer. In a cohort, IBD was associated with an increased incidence of CMM (incidence rate ratio [IRR], 1.29; 95% confidence interval [CI], 1.09-1.53), where the risk was greatest among individuals with Crohn's disease. The incidence of NMSC also increased among patients with IBD (IRR, 1.46; 95% CI, 1.40-1.53) (Long et al., 2012). In some studies, it has been found that immunosuppression increases the risk of CMM and NMSC among patients with IBD. The risk of CMM increased with the use of biologics, and the risk of NMSC increased with the use of thiopurines (Bahi et al., 2018; Long et al., 2012; Setshedi et al., 2012).
However, some studies hold the opposite view that the risk of NMSC in IBD patients who use thiopurine will not increase (van Schaik et al., 2011). Most articles believe that there is a correlation between IBD and skin cancer, whereas a few articles support the absence of a direct correlation between the two.
Mendelian randomization (MR) is an approach to investigate causality between risk factors and outcomes (Emdin et al., 2017). This method uses single nucleotide polymorphisms (SNPs) as unconfounded indicators for exposures, which can avoid reverse causality and residual confounding compared with conventional observational studies (Burgess et al., 2013). MR follows the randomly assorted meiosis principle of allele separation and the free recombination of nonalleles, in which the procedure mimics an randomized controlled trial (Davey Smith and Hemani, 2014; Sekula et al., 2016). Therefore, MR can be used as an important causal inference strategy. Here we conducted a two-sample MR study to investigate the causal association of IBD and skin cancer by using large-scale publicly available genome-wide association study (GWAS) data.
Materials and Methods
Data resources
GWAS predominantly relied on data from individuals of European descent. Summary statistics for IBD were obtained from the case-control GWAS meta-analysis, which included a total sample size of 59,957 participants of IBD (25,042 cases and 34,915 controls). The total sample size of Crohn's disease included 40,266 participants (12,194 cases and 28,072 controls), and total sample size of the ulcerative colitis included 45,975 participants (12,366 cases and 33,609 controls) (de Lange et al., 2017). GWAS data for skin cancer were acquired from the Medical Research Council Integrative Epidemiology Unit (MRC-IEU), which included 462,933 patients of European ancestry (1436 cases and 461,497 controls). For CMM, we used data from the UK Biobank, consisting of 375,767 Europeans (3751 cases and 372,016 controls). For NMSC, we also used data from the UK Biobank, consisting 395,710 Europeans (23,694 cases and 372,016 controls).
Selection of genetic instruments
We selected SNPs that were strongly associated with IBD of genome-wide significance (p < 5 × 10-8). To prune SNPs in linkage disequilibrium (R2 > 0.001 within a 10,000 kb window), we used the clump data function in the TwoSampleMR software package in R-Studio (Howe et al., 2021; Yavorska and Burgess, 2017) (Supplementary Data S1). These strictly selected SNPs were used to the final SNPs for subsequent MR analysis. The strength of the genetic instruments was represented by the F-statistic (Fig. 1 and Supplementary Data S2) (VanderWeele et al., 2014).
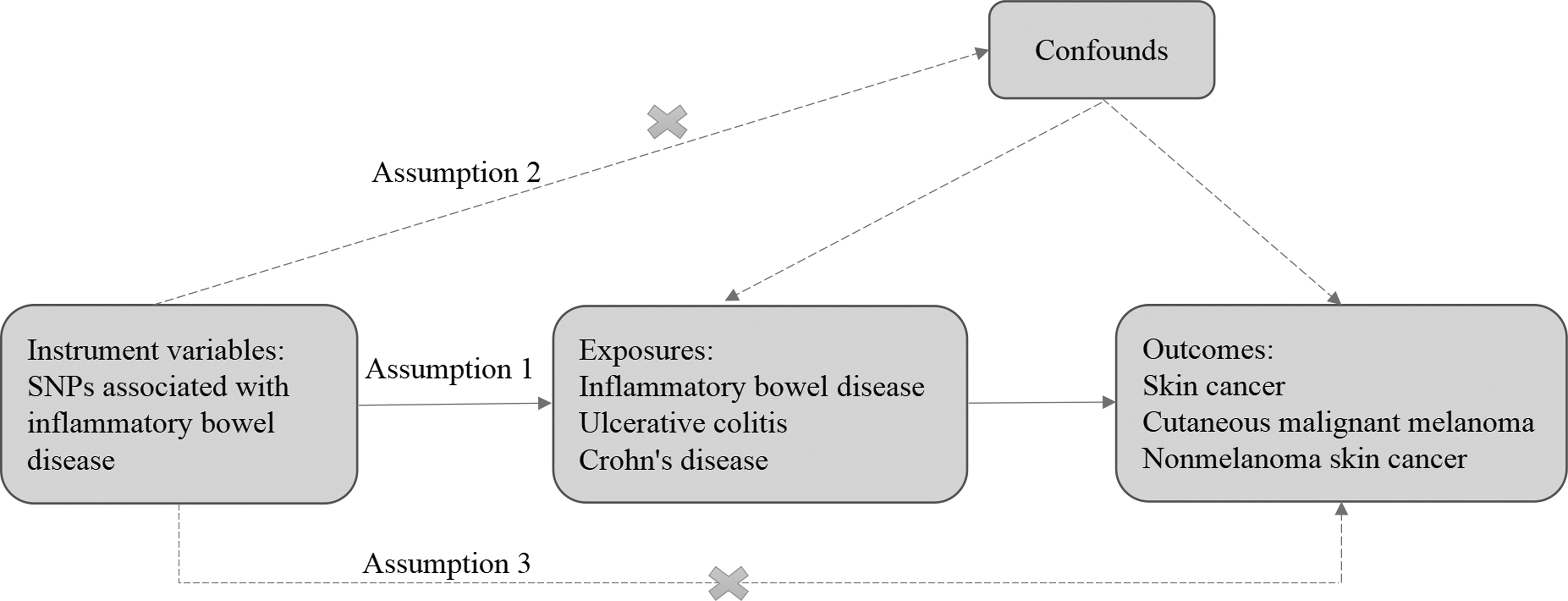
Conceptual framework for MR analysis of causal effects of IBD on the risk of skin cancer. Assumption 1, genetic variants are closely associated with exposure; assumption 2, genetic variants are not associated with potential confounders; assumption 3, genetic variants affect the outcomes only through the exposure of interest. IBD, inflammatory bowel disease; MR, Mendelian randomization; SNP, single nucleotide polymorphism.
Statistical analysis
We used a two-sample MR analysis approach to obtain a standardized estimate of the causal effect of the exposure on the outcome (Davies et al., 2018). For this analysis, we selected the random-effects inverse-variance weighted (IVW) method as our primary analytical approach, which utilizes Wald ratio estimates. In situations where there is no evidence of directional pleiotropy, this analysis is considered to be the most robust and reliable (Pierce and Burgess, 2013). We also utilized alternative analyses, including maximum likelihood, MR Egger, weighted median, penalized weighted media, simple mode, and weighted mode method. The weighted median assumes that at least 50% of the instruments are valid (Bowden et al., 2016). Assuming the invalidity of all instruments, as done by MR-Egger, represents a method with low power but still accounts for pleiotropy (Burgess and Thompson, 2017; Zheng et al., 2017). We considered a statistically significant causal relationship to be present when the p-value was <0.0056 (Bonferroni corrected for three exposures and three outcomes). To assess the risk of skin cancer, our MR results were reported as odds ratios (ORs) with corresponding 95% CIs.
Sensitivity analysis was conducted to assess any potential violations of MR assumptions. The Cochran Q-test statistics were utilized to identify heterogeneity in the IVW model (Greco et al., 2015). In the Cochran Q-test, when p value was <0.05 we considered that there was potential heterogeneity. Excessive heterogeneity indicates many invalid instruments in our study, and which would induce horizontal pleiotropy (Bowden et al., 2019). In this case, the weighted median model is recommended for analysis as it provides slightly less precise estimates, but for heterogeneous outliers that holds inherent robustness (Bowden and Holmes, 2019).
We also used the intercept term of MR-Egger regression to judge the horizontal pleiotropy tests (Bowden et al., 2017). If the p-value was >0.05, indicating no evidence of horizontal pleiotropy in this analysis, the results of MR analysis were reliable. The symmetry of funnel plot was also used to gauge the reliability of the MR analysis. Moreover, to examine the impact of each SNP on the overall data statistics, we used the leave-one-out method as a sensitivity analysis. In this method the MR was performed again but leaving out each SNP in turn, to determine whether any SNP is excluded from affecting the analysis results.
Results
Through analysis, we found that IBD (including Crohn's disease and ulcerative colitis) had a direct causal relationship with NMSC, but not with CMM or skin cancer.
Mendelian randomization
We used a robust statistical technique known as two-sample MR to discern the causal relationship between the two phenotypes. To derive the MR estimate, we conducted an IVW meta-analysis of individual Wald ratios. There was significant association between IBD and NMSC outcomes (all p < 0.05) (Table 1). The occurrence of NMSC was associated with IBD, where IBD served as a predisposing factor for NMSC (IVW for IBD on NMSC [OR, 1.0025; 95% CI, 1.0007-1.0044]; IVW for Crohn's disease on NMSC [OR, 1.0021; 95% CI, 1.0004-1.0039]; IVW for ulcerative colitis on NMSC [OR, 1.0025; 95% CI, 1.0006-1.0044]; Table 1). The causal estimates between different MR models were generally consistent (Table 1). Through MR analysis, no associations were found between IBD and CMM (all p > 0.05; Supplementary Data S3).
Mendelian Randomization Associations of Nonmelanoma Skin Cancer with Inflammatory Bowel Disease from Different Models
CI, confidence interval; IVW, inverse variance weighted; MR, Mendelian randomization; NMSC, nonmelanoma skin cancer; OR, odds ratio.
Scatter plot estimates the genetic risk of IBD on skin cancer. Scatter plot illustrated the genetic effects on IBD versus their effects on skin cancer. Each line corresponded to the estimated MR effect from different methods (Fig. 2). Based on the analysis results, the presence of a positive causal relationship between IBD and NMSC could be deduced, thereby suggesting that IBD was a risk factor for NMSC (Fig. 2). The results of IVW and MR Egger could be more intuitively explained by the forest plot (Fig. 3). Here, only the statistical graphs depicting the relationship between IBD and NMSC were presented, the rest of the statistical graphs are given in Supplementary Data S4.
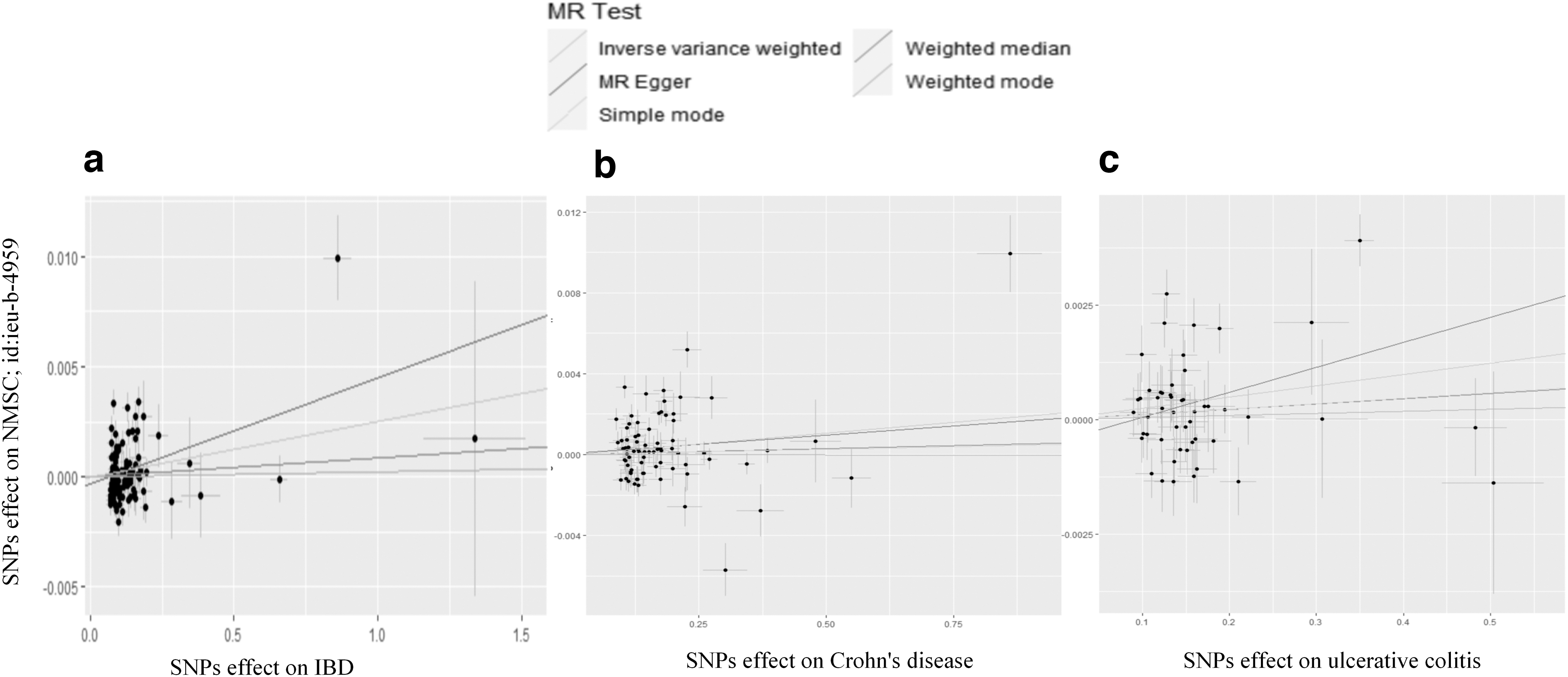
Scatter plots estimate the genetic risk of IBD on NMSC. The slope of each line corresponds to the estimated MR effect from different methods. The results depicted in all three graphs demonstrate a positive correlation between IBD, encompassing both Crohn's disease and ulcerative colitis, and NMSC. Scatter plot for IBD on NMSC
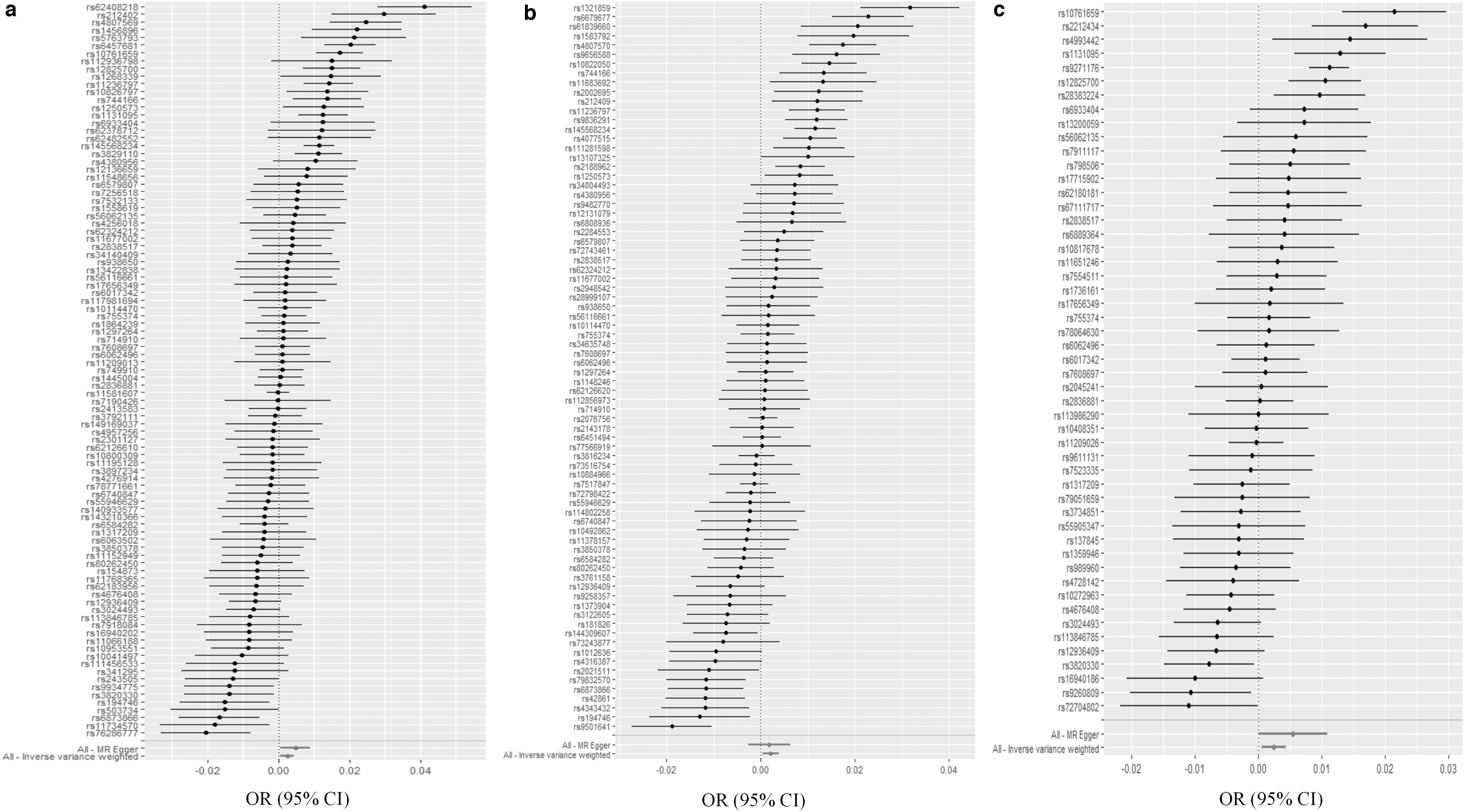
Forest plots of IBD and NMSC. Every horizontal line denotes a 95% CI of different SNPs. Two lines at the bottom indicate the pooled MR Egger and IVW MR estimate. Forest plot for IBD on NMSC
Sensitivity analyses
Cochran's Q-test showed that no heterogeneity was detected in the IVW model (Table 2). MR Egger intercept showed no directional pleiotropy detected (Fig. 2). The effect size of each SNP on skin cancer is given in Supplementary Data S3.
Sensitivity Analyses with Different Methods
CMM, cutaneous malignant melanoma (also referred to as melanoma skin cancer).
Moreover, leave-one-out analysis proved that the IVW estimate was not reliant upon any single SNP (Fig. 4). From the funnel chart, it could be known that the genetic variants estimation is basically symmetrical, and there was little possibility of bias (Fig. 5). Please refer to Supplementary Data S3 for additional analytical data.

Leave-one-out analyses estimate each genetic risk of IBD on NMSC

These funnel plots show relatively robust symmetry. Funnel plot for IBD on NMSC
Discussion
This study used a novel two-sample MR analysis to assess the causal impact of IBD on skin cancer outcomes. Our MR analysis did not provide evidence supporting an increased risk of skin cancer and CMM associated with the IBD gene, but it did indicate an elevated risk of NMSC.
At present, the existing research on the association between IBD and skin cancer consists of case-control studies and case reports, lacking direct evidence from basic research. In a cohort study conducted by Long et al., individuals with IBD demonstrated an increased incidence of CMM (IRR, 1.29; 95% CI, 1.09-1.53). In addition, the incidence of NMSC also exhibited an increase among patients with IBD (IRR, 1.46; 95% CI, 1.40-1.53). Of note, in the nested case-control studies, therapy with biologics increased the risk of CMM (OR, 1.88; 95% CI, 1.08-3.29). Patients treated with thiopurines had an increased risk of NMSC (OR, 1.85; 95% CI, 1.66-2.05). This study suggested that immunosuppression might have contributed to an elevated risk of melanoma and nonmelanoma skin cancer in individuals with IBD (Long et al., 2012). The utilization of biological agents elevated the susceptibility to CMM, whereas the administration of thiopurines heightened vulnerability to NMSC (Long et al., 2012).
Therefore, existing articles suggested the necessity of conducting risk assessment before the administration of immunosuppression. It was crucial for patients undergoing immunosuppression to have access to appropriate preventive and therapeutic measures for skin cancer (De Luca et al., 2013; Kimmel et al., 2016; Siao and Velayos, 2014).
Our study suggested that there was a direct causal relationship between IBD and NMSC. Nevertheless, no evidence supported a distinct causal relationship between IBD and skin cancer, or between IBD and CMM. Patients with IBD often experienced comorbidities affecting multiple organ systems, including the skin, which was commonly affected in these patients. However, there was insufficient experimental data to support a direct causal link between IBD and skin cancer. Some studies suggested that the immunosuppressive therapy used by IBD patients might increase the risk of developing skin cancer. Nevertheless, Van Schaik et al. indicated that the use of thiopurines in patients with IBD did not elevate the risk of NMSC (van Schaik et al., 2011). Thus, subsequent MR studies could be conducted to investigate the causality between immunosuppression and skin cancer.
Strengths and Limitations
This study has several key advantages. First, alleles are randomly assorted at conception, so bias caused by reverse causation can be largely avoided (Fu et al., 2021). Second, compared with conventional epidemiological studies we used a two-sample MR analysis to assess independent effects of the IBD on multiple skin cancer outcomes, offering the possibility to overcome traditional limitations. Third, our study benefits from a large sample size that enables us to conduct robust MR analysis.
This study has several limitations. First, although we utilized the largest GWAS available, only a limited number of SNPs met genome-wide significance, potentially resulting in weak genetic instruments (Ran et al., 2023). However, it was reassuring that effect estimates were robust by different MR models and the sensitivity analyses based on various assumptions failed to detect any horizontal pleiotropy in our study. Second, owing to the lack of original data, we were unable to analyze the impact of different stages of IBD on skin cancer. Finally, this article solely investigated the correlation between IBD and skin cancer without further exploring the potential impact of immunosuppressive drugs (a therapeutic option for IBD) on skin cancer.
Conclusions
Through this research, noteworthy discoveries were made in our investigation. Specifically, IVW revealed a significant p-value when examining the relationship between IBD and NMSC establishing a positive causal relationship. IBD was considered a risk factor for NMSC. In addition, MR analysis showed no direct genetic causation between IBD and CMM, or between IBD and skin cancer. Every sensitivity analysis underscored the robustness of our MR analysis. Nevertheless, it was crucial to acknowledge existing literature that highlighted a potential relationship between immunosuppression in IBD treatment and an increased risk of skin cancer. This finding may guide our further research directions.
Footnotes
Acknowledgment
The authors thank all the investigators for sharing summary-level data on GWAS for IBD and skin cancer.
Authors' Contributions
A.L.: wrote the article and data analysis. M.Y.: Organized data and materials. K.W.: data analysis and data interpretation. L.L.: revised the article and provided suggestions. X.S.: designed the study and provided support.
Ethics Statement
According to local legislation and institutional requirements, ethical review and approval was not required for this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.