
Abstract
Aims:
This study aimed to investigate the impact of genetic polymorphisms of thiopurine methyltransferase (TPMT) and NUDT15 on pharmacokinetics profile of mercaptopurine in healthy adults in China.
Methods:
Blood samples were obtained from 45 healthy adult volunteers who were administered azathioprine. Genomic DNA was extracted and sequenced for TPMT and NUDT15. The plasma concentrations of 6-mercaptopurine (6-MP) were determined by ultra-performance liquid chromatography-tandem mass spectrometry. Finally, pharmacokinetic parameters were calculated based on the time-concentration curve.
Results:
Among the 45 healthy adult volunteers enrolled in the study, two TPMT allelic variants and three NUDT15 allelic variants were detected. In total, six genotypes were identified, including TPMT*1/*1&NUDT15*1/*1, TPMT*1/*1&NUDT15*1/*2, TPMT*1/*1&NUDT15*1/*9, TPMT*1/*1&NUDT15*2/*5, TPMT*1/*6&NUDT15*1/*2, and TPMT*1/*3&NUDT15*1/*2. The results indicated that Area Under Curve (AUC) of 6-MP in volunteers with TPMT*1/*3&NUDT15*1/*2 and TPMT*1/*6&NUDT15*1/*2 were 1.57-1.62-fold higher than in individuals carrying the wild type (TPMT*1/*1&NUDT15*1/*1). Compared with wild type, the half-life (T1/2) of TPMT*1/*6&NUDT15*1/*2 was extended by 1.98 times, whereas T1/2 of TPMT*1/*3&NUDT15*1/*2 decreased by 67%. The maximum concentration (Cmax) of TPMT*1/*3&NUDT15*1/*2 increased significantly by 2.15-fold, whereas the corresponding clearance (CL/F) decreased significantly by 58.75%.
Conclusion:
The findings of this study corroborate the notion that various genotypes of TPMT and NUDT15 can impact the pharmacokinetics of mercaptopurine, potentially offering foundational insights for personalized mercaptopurine therapy.
Introduction
Azathioprine (AZA), a member of the mercaptopurine family, is widely used in the treatment of acute lymphoblastic leukemia, inflammatory bowel disease (IBD) to achieve clinical remission and reduce of steroid dependence, and various autoimmune diseases (Harmand and Solassol, 2020; Kakuta et al., 2018). It acts as a potent cytotoxic and immunosuppressive agent. 6-Mercaptopurine (6-MP), directly metabolized from AZA, has limited oral bioavailability and needs to be activated by drug metabolizing enzymes such as other inactive thiopurines (Fernández-Ramos et al., 2017). These prodrugs were transformed into intracellular thioguanine nucleotides to exert immunosuppressive and cytotoxic effects. Its main cytotoxic mechanism is to replace guanine (G) into DNA to form DNA-TG as a substrate of deoxyribonucleic acid polymerase, and mismatch with thymine (T) during subsequent DNA replication, then activating the mismatch repair mechanism, finally leading to DNA damage and cell apoptosis. The common adverse reactions of AZA include leukopenia and hepatotoxicity (Relling et al., 2019a).
Thiopurine methyltransferase (TPMT), the key enzyme of AZA metabolism, can use S-adenosyl-L-methionine as a methyl donor. It can combine with substrate 6-MP, then catabolize mercaptopurine into inactive methyl mercaptopurine bases, reducing the amount of parent drug. Thus, the ultimate formation of active thioguanine nucleotides is reduced. Many studies believe that TPMT activity is related to the efficacy and adverse effects of purine drugs. Therefore, the polymorphism of the TPMT gene determines the enzymatic activity (Zimdahl Kahlin et al., 2021).
Another enzyme that plays an important role in the metabolism of AZA is NUDT15 (Moriyama et al., 2017). As a nucleoside diphosphatase, NUDT15 catalyzes the conversion of cytotoxic metabolites (TGTP) to nontoxic thioguanine monophosphate (TGMP). The decreased capacity of TGTP transformation mediated by NUDT15 leads to the incorporation of more TGTP into DNA to form DNA-TG, which leads to DNA damage and cell apoptosis, resulting in severe myelosuppression in patients (Moriyama et al., 2017). It has been reported that polymorphisms of the NUDT15 gene has a greater effect on the metabolic toxicity of AZA than TPMT in an Asian population (Banerjee et al., 2020; Sutiman et al., 2018; Zhu et al., 2016).
Appropriate medication guidance based on the patient’s genotype is important in the treatment of leukemia to maximize the efficacy of thiopurine drugs and reduce cytotoxicity (Suiter et al., 2020). To systematically characterize TPMT and NUDT15 polymorphisms associated with AZA metabolic capacity and bioavailability, herein we sequenced all exonic regions of the two genes in 45 volunteers. Subsequently, the pharmacokinetics profile of 6-MP was determined. The study here would aim to personalize the use of AZA.
Materials, Methods, and Subjects Studied
Volunteers and AZA administration
This test screened a total of 48 healthy adult males and nonpregnant nonlactating females, who were given 50 mg AZA tablets each to carry out fasting pharmacokinetics tests. Before the start of the formal trial, one subject withdrew from the trial owing to an adverse effect reaction. After the administration, two subjects withdrew from the trial, one at their own request, and the other tested positive for Treponema pallidum-specific antibodies and was mistakenly included initially. Thus, 45 subjects remained at the final safety follow-up.
Single Nucleotide Polymorphism (SNP) selection and targeted genotyping
Based on the TPMT and NUDT15 genetic polymorphisms downloaded from the PubMed and PharmGKB database. We used the Maxwell® 16 System to purify the genomic DNA from peripheral blood samples. Genomic DNA with a high concentration (>100 ng/µL) was directly utilized for Polymerase Chain Reaction (PCR) reactions after a short centrifugation. The products were subsequently sequenced by an ABI (Applied Biosystems) 3730 automated sequencer. Sequence data comparisons and analyses were performed using DNASTAR SeqMan.
Pharmacokinetic study of 6-MP
Forty-five volunteers were treated with oral doses of 50 mg AZA each to assess their pharmacokinetics. All the experimental procedures were in accordance with the Guide for the Good Clinical Practice (ICH E6(R2)). Diet was prohibited for 12 h before the experiment. Water was prohibited for 1 h before the experiment. Blood samples were collected from the vein into heparinized tubes (10 mL at 0 h and each 4 mL at 0.25, 0.5, 0.75, 1, 1.25, 1.5, 1.75, 2, 2.25, 2.5, 3, 4, 5, 6, 8, and 10 h after administration). Each blood sample was centrifuged at 1500×g for 10 min at 4°C, then immediately transferred into anticoagulant tubes and stored at −80°C until analysis. Plasma concentrations 6-MP versus time data for each volunteer were analyzed by WinNonlin7.0.
Detection of 6-MP concentration
Ultra-performance liquid chromatography-tandem mass spectrometry (UPLC-MS/MS) was employed for the quantification and identification of 6-MP in human plasma using the Exion AD-SCIEX TRIPLE QUADTM 5500 from SCIEX. Chromatographic separation was conducted on a Waters ACQUITY UPLC® Hss T3 column (2.1*50 mm, 1.8 μm). We procured 6-MP and 6-MP-13C2,15N (Internal standards, IS) from Toronto Research Chemicals. The mobile phase (solvent A) consisted of a 0.05% formic acid aqueous solution, whereas the organic phase (solvent B) comprised a 0.05% formic acid acetonitrile solution. The gradient program was as follows: 0.01-0.30 min 7% B, 0.40 mL/min; 0.30-0.50 min 7-40% B, 0.35 mL/min; 0.50-1.30 min 40-95% B, 0.35 mL/min; 1.30-2.30 min 95% B, 0.35 mL/min; 2.30-2.80 min 95-7% B, 0.40 mL/min; 2.30-2.80 min 95-7% B, 0.40 mL/min; 2.80-3.80 min 7% B, 0.40 mL/min. The total running time was 4.0 min. In the positive ion mode, the peak area of the mass-to-charge ratio (m/z) 153.1→119.1 for 6-MP was measured against the peak area of the (m/z) 153.1→122.0 for IS. The precision (%CV) of the Low Level Quality Control (LQC), Geometric Medium Level Quality Control (GMQC), Medium Level Quality Control (MQC), and High Level Quality Control (HQC) concentration quality control products was ≤3.59%, and the accuracy deviation range of each quality control sample was −3.75% to 0.21%.
Statistical analyses
The plasma concentration-time profiles of 6-MP were evaluated by noncompartmental analysis. The area under the plasma concentration-time curve from time zero to infinity [AUC (0-∞) and AUC (0-t)], T1/2, Cmax, and Tmax were calculated by WinNonlin7.0. The student t-test was used to analyze pharmacokinetic and pharmacodynamic differences in catalytic activity between the TPMT*1/*1&NUDT15 *1/*1 and TPMT*1/*1&NUDT1*1/*2 subjects. Statistical analyses were performed with the SPSS package (version 19.0; SPSS, Chicago, IL), with p < 0.05 considered to be statistically significant.
Ethics
The study protocol was approved by the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University (REC number: LCKY2019-190) in July 2019. The procedures followed were in accordance with the Declaration of Helsinki. Written informed consent was obtained before the study entry.
Results
Demographic characteristics of volunteers
There were 48 healthy volunteers enrolled in our study. Of these, three were excluded owing to mistaken inclusion, AE occurred or at the request of the subject. Thus, 45 adults, aged 18-50 years were included in the analyses. Each volunteer received a standard dose of 50 mg of AZA tablets. Demographic data for volunteers are summarized in Table 1.
Demographic Data of Volunteers
TPMT and NUDT15 genotype and distribution frequency
Forty-five volunteers included 8 females and 37 males, of which no mutations were detected in 32 subjects. Ten subjects had one mutant allele and three subjects had two mutant alleles (shown in Fig. 1). For TPMT genotype, the TPMT*1 distribution frequency was 97.78%, which is similar to previous counting results of South Asian and East Asian (https://cpicpgx.org/); TPMT*3 and *6 mutation frequencies were both 1.11%. As for NUDT15 genotype, our results showed that the NUDT15*1 distribution frequency was 84.44%, NUDT15*2 mutation frequency was 13.33%, and NUDT15*5 and *9 mutation frequency were both 1.11%. The frequency of NUDT15*1 of this study is close to previous East Asian study results.

Sanger sequencing of the mutated regions confirms the findings of next generation sequencing in several individuals.
TPMT and NUDT15 genotype and pharmacokinetic characteristics
The pharmacokinetic parameters of AUC (0-∞), AUC(0-t), Cmax, oral clearance (CL/F), and T1/2 were calculated to functionally characterize the catalytic activities of TPMT alleles and NUDT15 alleles, and the concentration-time curves of 6-MP were shown in Figure 2 and the pharmacokinetic data were shown in Table 2.
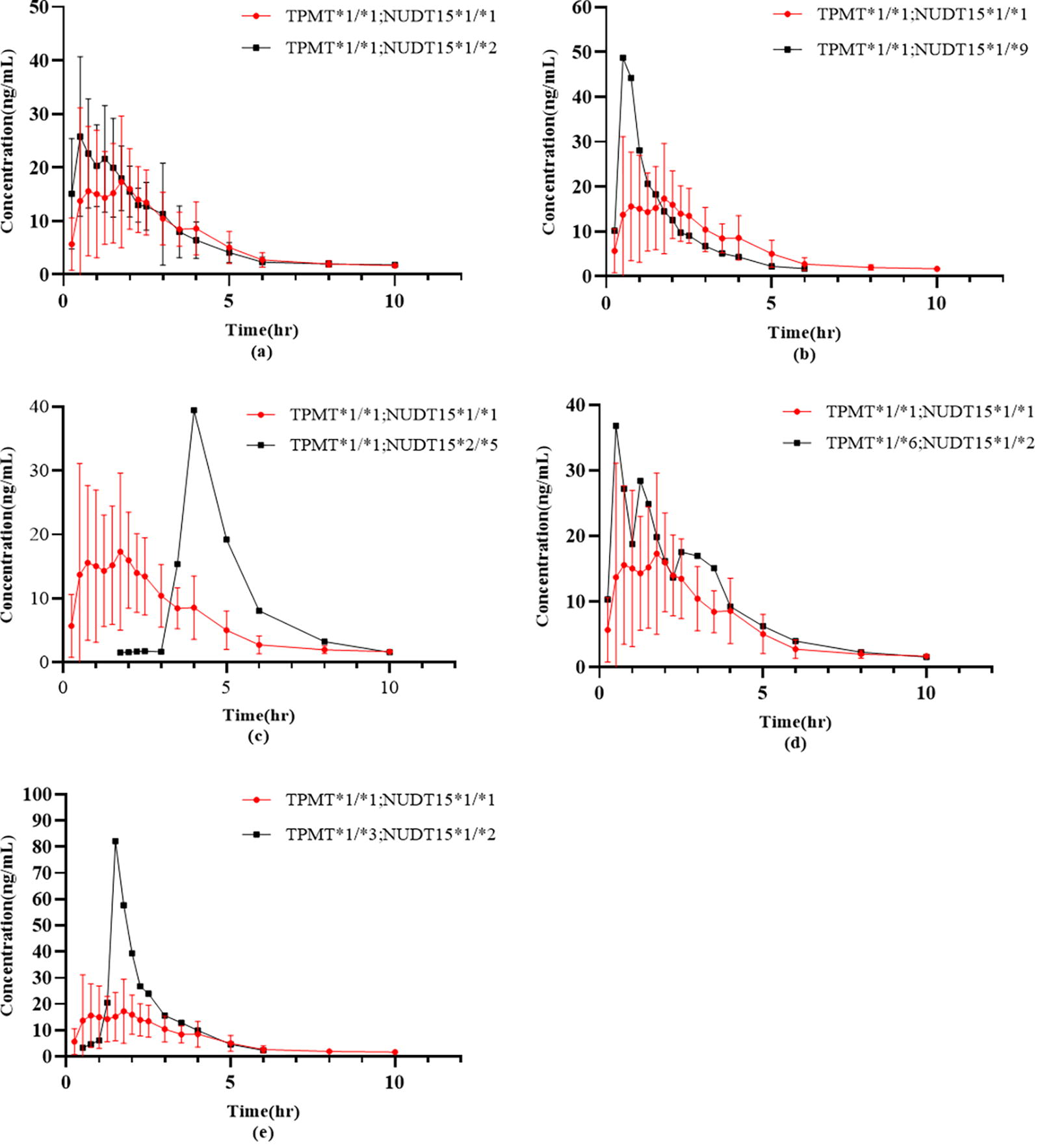
Mean plasma concentration-time curves of 6-MP after a single dose of AZA in 45 healthy subjects with different genotypes under fasting conditions (mean ± SD, n = 45). Compared with wild types of TPMT and NUDT15,
Pharmacokinetic Parameters of 6-MP in Healthy Subjects
Values are mean ± SD. *, **Indicate significant difference from wild-type TPMT and NUDT15 at p < 0.05 and p < 0.01, respectively.
Based upon results, we found that the genetic polymorphisms in the TPMT and NUDT15 were associated with 6-MP metabolism. The areas under the drug time curve of the mutants were higher than those of the wild type, especially the double mutants in TPMT and NUDT15 alleles. Pharmacokinetic parameters from TPMT and NUDT15 polygenic mutations also indicated that there were significant differences between wild-type and single NUDT15 gene heterozygote.
Results from single allele mutation of NUDT15 gene heterozygote (NUDT15*1/*1 and NUDT15*1/*9) showed slightly higher AUC and Cmax than the wild type (TPMT*1/*1&NUDT15*1/*1); and the CL/F of 6-MP were lower than wild type. Furthermore, double allele mutation of NUDT15 gene heterozygote (NUDT15*2/*5) showed even more higher AUC and Cmax than single-allele mutations of NUDT15. In addition, more striking pharmacokinetic differences can be found in TPMT and NUDT15 polygenic mutations. Subjects with genotypes of TPMT*1/*6&NUDT15*1/*2 and TPMT*1/*3&NUDT15*1/*2 had 1.62-fold and 1.57-fold increases in AUC0→∞, as well as both 1.62-fold increases in AUC0→t, respectively, when compared with subjects with genotype of TPMT*1/*1&NUDT15*1/*1. Meanwhile, when compared with the wild-type, t1/2 of TPMT*1/*6&NUDT15*1/*2 prolonged 1.98-fold, however t1/2 of TPMT*1/*3&NUDT15*1/*2 decreased to 67%. For Cmax and the CL/F, we found no difference between genotypes TPMT*1/*6&NUDT15*1/*2 and TPMT*1/*1&NUDT15*1/*1, but Cmax of TPMT*1/*3&NUDT15*1/*2 significantly increased with a 2.15-fold of wild-type, corresponding CL/F significantly decreased by 58.75%.
Discussion
Metabolic enzymes TPMT&NUDT15 are involved in AZA metabolism, and their polymorphisms are ethnically different and are closely associated with adverse reactions, such as 6-MP induced White blood cell (WBC) reduction or myelosuppression. However, the effect of TPMT&NUDT15 polymorphism on the pharmacokinetics of 6-MP is sparse. Thus, we sought to evaluate the correlation between 6-MP pharmacokinetics and major polymorphisms of NUDT15&TPMT in Chinese volunteers.
We enrolled 45 volunteers and used standard dose of 50 mg AZA to examine the relationship of the concentration of 6-MP and genetic polymorphisms. It is necessary to validate the effect of an at-risk genotype on 6-MP metabolism, and then predict its toxicity in individuals. AZA was converted to 6-MP in vivo, then, converted into the inactive product 6-methylmercaptopurine (6-MMP) under the action of TPMT, or into the active metabolites 6-thioguanine nucleotides (6-TGN) through a series of metabolic enzymes. Cytotoxic 6-TGNs that chelate DNA and RNA could be dephosphorylated by NUDT15, and converts to noncytotoxic mono phosphoric acid 6-TGMP. Genetic mutations of TPMT and NUDT15 could lead to leukopenia and hepatotoxicity by inhibiting nucleosides and protein synthesis (Kakuta et al., 2016; Zhu et al., 2016).
We studied the individual differences of 6-MP concentrations based on the functional characteristics of 2 TPMT allelic variants and 3 NUDT15 allelic variants in vivo. Our results indicated six different types of genotypes in volunteers as follows: TPMT*1/*1&NUDT15*1/*1, TPMT*1/*1&NUDT15*1/*2, TPMT*1/*1&NUDT15*1/*9, TPMT*1/*1&NUDT15*2/*5, TPMT*1/*6&NUDT15*1/*2, and TPMT*1/*3&NUDT15*1/*2. The genotypes identified in this investigation, specifically TPMT * 1/* 3 and NUDT15 * 1/* 2, have been reported as intermediate metabolic phenotypes. Likewise, NUDT15 * 2/* 5 has been reported as possible intermediate metabolic phenotypes (Relling et al., 2019).
The allelic variants found in this study, such as TPMT*3, TPMT*6, NUDT15*2, NUDT15*5, NUDT15*9, have been reported previously, and their distribution frequency was similar to previous counting results reported for South Asian and East Asian (https://cpicpgx.org/). As reported in previous studies, the TPMT variants were extremely low (with a mutation rate of 2.2%) in our study population, which was similar with the results of Asians from Clinical Pharmacogenetics Implementation Consortium (CPIC) and other reports (Jena et al., 2021; Kakuta et al., 2018; Wang et al., 2018). Thus, TPMT variants were inappropriate for use as a pharmacogenetic marker for thiopurine therapy in Chinese patients. The frequencies of NUDT15 variants were observed to be 15.6% in our study, which is similar to 19.75% in Chinese Bai children (Pu et al., 2021) and 13.2% in Korean (Kim et al., 2017). Therefore, NUDT15 is indicated as a potential marker of 6-MP sensitivity, especially for people with a low frequency of TPMT variants, as reported (Yang et al., 2014).
According to Figure 2 and Table 2, we found that NUDT15 c.415C>T (NUDT15*1/*2) had a lower effect on 6-MP concentration in volunteers than NUDT15*1/*9, which is consistent with the results of Lee et al (Lee et al., 2021). We also found that the AUC of 6-MP of subjects with double mutation of TPMT and NUDT15 was obviously higher than that of subjects with nonmutated and single-mutant individuals. At the same time, comparing individuals with only NUDT15 mutations, it was found that NUDT15*2/*5 individuals had a higher AUC compared with NUDT15*1/*9, and the AUC of NUDT15*2/*5 was between the double-metabolic enzyme mutant and the single-metabolic enzyme unit point mutation. It is speculated that TPMT and NUDT15 mutations cause a decrease in metabolic enzyme activity and an increase in the concentration of the prodrug 6-MP. Considering the narrow therapeutic window and the severe adverse reactions for 6-MP, the use of AZA/6-MP is not recommended in patients with double-mutation of NUDT15, as reported (Lee et al., 2017; 2021). In brief, the variants of two mutant alleles (TPMT&NUDT15) present many differences in the AUC (0→∞), AUC(0→t), C max, and T1/2, respectively, compared with subjects with one allelic mutant.
In conclusion, we selected AZA as the probe drug and identified the catalytic activity of six genotypes of TPMT and NUDT15 in vivo. Our results showed that mutations in these genes can affect the metabolism of 6-MP in the body to a certain extent. For example, affecting the path of 6-MP and increasing its blood concentration. During the treatment, attention should be paid to patients with intermediate and weak activity of TPMT and NUDT15 to avoid a high concentration of 6-MP, which could induce AZA intolerance. These in vivo studies provide the pharmacokinetic parameters of these allelic variants and support the preemptive TPMT and NUDT15 genotype-guided thiopurine dosing to prevent toxicity in Chinese patients in the future.
However, because the present pharmacokinetic study involved only one subject for individual genotypes and lacks in vitro enzyme activity tests, further large-scale clinical studies are needed to accurately assess the effects of TPMT and NUDT15 genetic variations on 6-MP dosing in vivo.
Conclusions
This study identified the catalytic activity of six genotypes of TPMT and NUDT15 in vivo, and the polymorphisms identified were reported as weak metabolite genotypes; also found that the distribution frequencies of allelic variants of TPMT and NUDT15 found in this study were similar to previous counting results of South Asian and East Asian. We also found that individuals with two mutant alleles (TPMT&NUDT15) exhibit much greater differences in the pharmacokinetic parameters, respectively, when compared with subjects with one allelic mutant. These findings support implementation of the TPMT and NUDT15 genotype-guided thiopurine dosing to prevent toxicity in Chinese patients in the future.
Footnotes
Acknowledgments
We sincerely thank the study participants for their contribution to the research, as well as current and past investigators and staff.
Authors’ Contributions
This work was carried out in collaboration with all authors. T.L.: Contributed to the study design. T.L. and Q.K.: Participated in drafting of the article. Q.K., Q.Z., D.C., J.L., J.Z., and M.C.: Conducted the experiments and data analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the