
Abstract
Background:
Early screening for colorectal cancer (CRC) has the potential to improve patient prognosis, but current screening methods are limited. In this prospective study, we aimed to evaluate the multigene (Septin9, SDC2, KCNQ5, and IKZF1) detection in patient plasma for CRC diagnosis.
Methods:
Overall, 67 participants were enrolled, including 31 patients with CRC, 17 patients with colorectal polyp, and 19 normal controls who underwent colonoscopy. Carcinoembryonic antigen (CEA) and Septin9, SDC2, KCNQ5, and IKZF1 methylation tests were performed. Sensitivity, specificity, and the area under the receiver operating characteristic (ROC) curve were used to evaluate the diagnostic value of each biomarker. The association between positive rates of methylated Septin9, SDC2, KCNQ5, and IKZF1 and the clinicopathological characteristics of CRC was also analyzed.
Results:
The positive rate of multigene methylation detection was 87.1% (27/31) in patients with CRC, which was higher than single indicators: CEA (51.61%, 16/31), Septin9 (41.94%, 13/31), SDC2 (41.94%, 13/31), KCNQ5 (58.06%, 18/31), and IKZF1 (32.26%, 10/31). In the colorectal polyp group, the rate of multigene methylation detection is 88.24% (15/17), which was also higher than single indicator: CEA (17.65%, 3/17), Septin9 (11.76%, 2/17), SDC2 (64.71%, 11/17), KCNQ5 (58.82%, 10/17), and IKZF1 (35.29%, 6/17). The ROC curves further showed better diagnostic value of the multigene test for CRC than any single gene. Correlation analysis found that the positive rate of the test was not affected by patients’ clinicopathologic characteristics.
Conclusion:
The combination of methylated Septin9, SDC2, KCNQ5, and IKZF1 tests is preferable to individual gene tests for patients with CRC and polyp.
Introduction
Colorectal cancer (CRC) is caused by malignant lesions that develop in the mucosal epithelium of the large intestine due to various factors, such as environmental or hereditary influences. It is the most common malignant tumor in the digestive system. According to the 2018 Global Cancer Report, CRC has an incidence rate of 10.2%, ranking third, and a mortality rate of 9.2%, placing it in second place (Bray et al., 2018). Despite the high incidence and mortality rate, CRC is highly curable at the early stage. The 5-year survival rate for patients with CRC at stage I is over 90%, while it drops to 14% at stage IV, highlighting the difficulty in treating patients with advanced stages of CRC (Siegel et al., 2020). Developing CRC screening methods can detect the cancer at an early stage, improving survival rates and guiding subsequent treatment (Brenner et al., 2014; Lin et al., 2016).
CRC detection methods encompass various techniques, including fecal occult blood test (FOBT), serum carcinoembryonic antigen (CEA) test, colonoscopy, and computed tomography simulation. FOBT and colonoscopy are the main detection methods, but they both suffer from low specificity and sensitivity, as well as high invasiveness, making it difficult to widely promote CRC screening. Furthermore, FOBT can be easily affected by diet, which would compromise the accuracy of test results. Colonoscopy, while effective, is time consuming and labor intensive and may cause discomfort to patients, as well as being expensive makes its large-scale promotion challenging (Shaukat and Levin, 2022). Thus, there is a need for a sensitive and compliant test to diagnose CRC earlier. Numerous studies have demonstrated that DNA methylation is an early event in the development of various types of cancers, and the methylation of specific genes can serve as molecular markers for early tumor screening (Delpu et al., 2013; Klutstein et al., 2016). Several studies have confirmed the diagnostic value of genes such as SDC2 (Han et al., 2019; Jensen et al., 2019), CLIP4 (Jensen et al., 2019) KCNQ5 (Jensen et al., 2019), SFRP1 (Salehi et al., 2012; Barták et al., 2017), and IKZF1 (Young et al., 2021) in CRC. However, most of these studies focus on single- or double-gene detections. This study aims to investigate the significance of multigene methylation detection in plasma circulating tumor DNA (ctDNA) for the clinical diagnosis of CRC.
Materials and Methods
Participants and samples
A total of 69 patients were screened from January 2023 to August 2023 in the Department of Anorectology of the Second Hospital of Tianjin Medical University. Ultimately, 67 participants were enrolled. The participants were divided into three groups: CRC group, colorectal polyp group (confirmed pathologically as adenomatous polyps), and control group. All blood samples in this study were collected at the Second Hospital of Tianjin Medical University in Tianjin, China. The recruitment flow diagram is depicted in Figure 1.
Flow chart of participants through the study.
Inclusion criteria: 18-85-year-olds; underwent colonoscopy; could provide complete clinical information. Main exclusion criteria: a history of radiotherapy or chemotherapy for CRC; a history of other malignant tumors. The pathological results of the samples were examined and confirmed by at least two attending pathologists. The diagnostic criteria referred to the diagnostic criteria of colorectal adenomatous polyps and CRC in the Clinical Guidelines for Gastrointestinal Diseases. This study was approved by the Ethics Committee of the Second Hospital of Tianjin Medical University (approval number: KY2023K207), and all participants signed informed consent forms.
DNA isolation and methylation testing
Blood samples were collected using a K2EDTA anticoagulant blood collection tube (10 mL specification single-use free DNA preservation tube, Kangwei Century, SUMCI 20192220059).
Each tube was gently inverted and mixed five to six times after blood collection. Each sample was then centrifuged immediately to prepare plasma, and the free DNA in the plasma was extracted using the VAHTS Serum/Plasma Circulating DNA Kit (N902-00, Lot#30825) from Novozymes, with a 2 mL sample volume. A total of 100 μL was used for the final elution. The operational procedure followed the instruction manual. Subsequently, 60 μL of the extracted product was treated with bisulfite using Epigenetics’ EZ DNA Methylation-Gold Kit, D5006, Sulfurization Kit, and 35 μL was used for the final elution. The operational procedure was described in the instruction manual.
Quantitative polymerase chain reactions (qPCR) were prepared according to the sample volume, with the following reaction conditions: pre-denaturation at 95°C for 5 min, denaturation at 95°C for 15 s, annealing and extension at 57°C for 60 s, 40 cycles, and finally, fluorescence values were recorded. Primers and probe sequences are shown in Table 1.
Primers and Probe Sequences
After the reaction was completed, the threshold and baseline of each channel were adjusted according to the situation. The cycle threshold (Ct) value of each sample was determined, and the difference between the Ct value of each target gene and the Ct value of the ACTB gene (internal reference control) was calculated as ΔCt [ΔCt = Ct (target gene) − Ct (ACTB)]. If no signal was detected from PCR, the Ct value was assigned as 40 (the maximum number of PCR cycles). The methylation status of Septin9, SDC2, KCNQ5, and IKZF1 was determined by calculating the ΔCt values compared with ACTB. When the ΔCt values were ≤4.02, ≤10.94, ≤5.36, and ≤6.49, respectively, the genes Septin9, SDC2, KCNQ5, and IKZF1 in the test sample were identified as positively methylated. If any one gene showed positive methylation, it was considered that all four genes were positively methylated.
Methylation detection in HCT116 and 293T cell lines
The HCT116 cell line, known for having methylation in all Septin9, SDC2, KCNQ5, and IKZF1 genes, was used as a positive control. In contrast, the 293T cell line, known for having no methylation in any of these four genes, was used as a negative control. Quantitative PCR was performed to detect the performance of methylation status of the Septin9, SDC2, KCNQ5, and IKZF1 genes.
CEA testing
CEA in serum was measured using the Roche Cobas 8000 electrochemiluminescence instrument. A CEA level of ≤5 ng/mL was considered the normal reference range for patients with a smoking history, whereas a CEA level of ≤3.5 ng/mL was the normal reference range for patients without a smoking history. Samples with values exceeding the upper limit of the normal range were classified as positive.
Statistical analyses
All statistical analyses were performed using SPSS software (version 26.0, IBM), and the count data were expressed as rates (%). For continuous variables, differences between two groups were compared using the chi-square test, while comparisons among more than two groups were conducted using a one-way analysis of variance test. Sensitivity, specificity, and area under the curve (AUC) were used to evaluate the performance of methylated Septin9, SDC2, KCNQ5, and IKZF1 for predicting CRC. The ROC curve was obtained by importing ΔCt values of each gene in the CRC group and the control group into SPSS software, and then ROC analysis was performed. Based on the results output by SPSS software, we calculated the Youden index and determined the cutoff values. All statistical tests were two-sided, and a p-value <0.05 was considered statistically significant.
Results
Participants
The 67 participants were divided into three groups. The CRC group comprised 31 patients with CRC, including 20 males and 11 females, with ages ranging from 41 to 85 years and an average age of 70.38 ± 9.94 years. The colorectal polyp group contained 17 patients with polyp, including 12 males and 5 females, aged 34-75 years and an average age of 60.07 ± 11.95 years. The control group consisted of 19 cases, with 14 males and 5 females, aged 20-72 years and an average age of 45.00 ± 12.57 years (Table 2).
Clinical and Pathological Data of Patients and Healthy Controls
CRC, colorectal cancer.
Methylation detection of Septin9, SDC2, KCNQ5, and IKZF1 in HCT116 and 293T cell lines
As shown in Figure 2, significant differences in the amplification curves of Septin9, SDC2, KCNQ5, and IKZF1 were observed between HCT116 and 293T cell lines, demonstrating the validity of the method used in this study.

The amplification curves of Septin9, SDC2, KCNQ5 and IKZF1 in HCT116 cell line and 293T cell line.
Positive detection rates of methylated Septin9, SDC2, KCNQ5, IKZF1, and CEA
When methylated Septin9, SDC2, KCNQ5, and IKZF1 were combined for CRC detection, the positivity rate was higher than that of the healthy group. In patients with CRC, the combined methylation test of the four genes has a positive rate of 87.10%, higher than that of CEA (51.61%), Septin9 (41.94%), SDC2 (41.94%), KCNQ5 (58.06%), and IKZF1 (32.26%). When these five indicators were tested in combination, the positive rate reached 90.32%. In patients with polyp, the positive rate of the four-gene combined test was 88.24%, higher than that of CEA (17.65%), Septin9 (11.76%), SDC2 (64.71%), KCNQ5 (58.82%), and IKZF1 (35.29%) (Table 3).
Comparison of Positive Methylation Rates in Three Groups (n [%])
CEA, carcinoembryonic antigen.
Diagnostic value of methylated Septin9, SDC2, KCNQ5, and IKZF1 for CRC
ROC analyses showed that when Septin9, SDC2, KCNQ5, and IKZF1 were detected individually, the AUC (sensitivity and specificity) values were 0.747 (51.60%, 100%), 0.657 (45.20%, 94.70%), 0.760 (64.50%, 94.70%), and 0.700 (58.10%, 100%), respectively. The AUC (sensitivity and specificity) was 0.818 (61.30%, 100%) in the four-gene combination test, as shown in Table 4 and Figure 3.
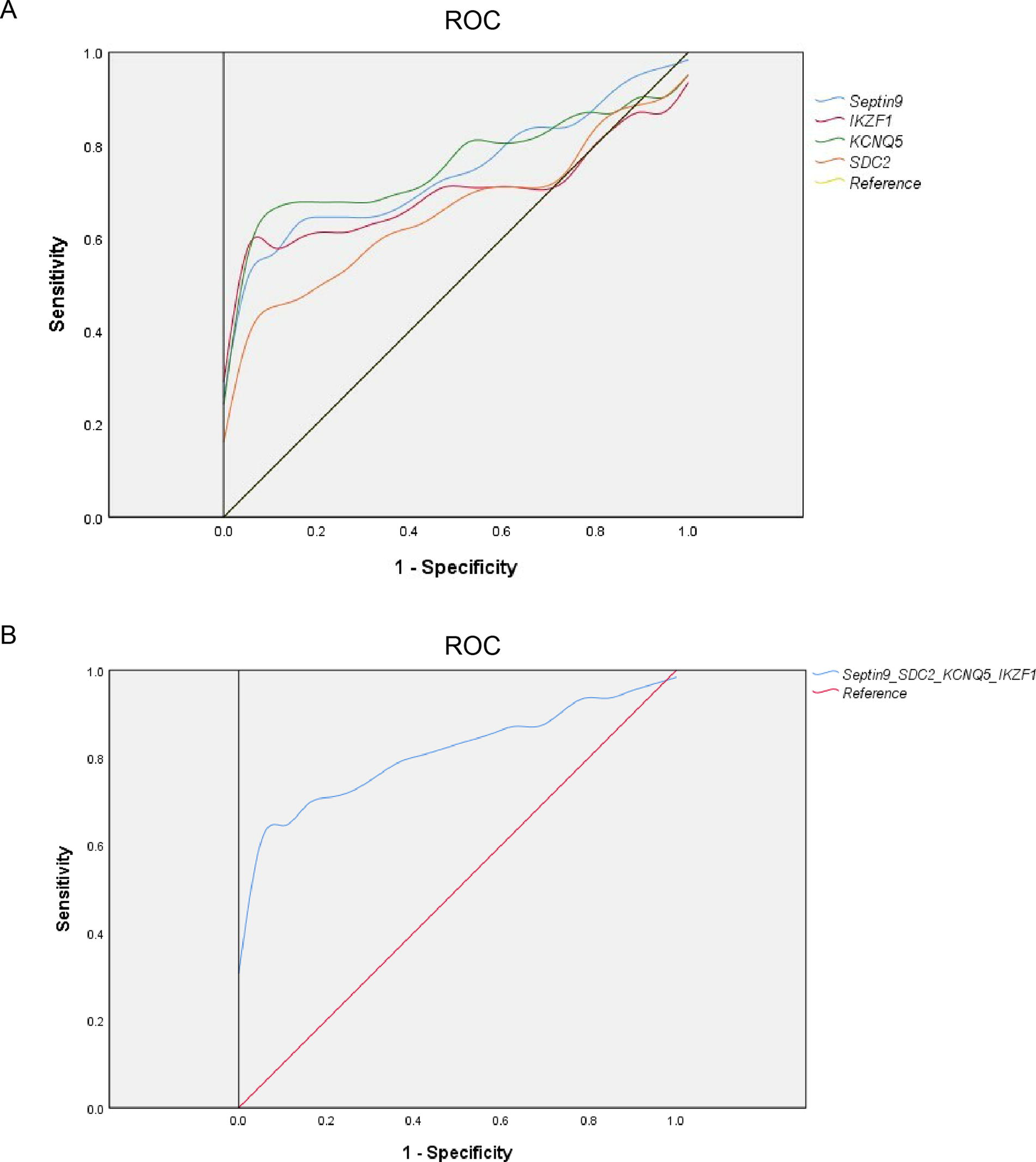
Diagnostic performance of Septin9, SDC2, KCNQ5, and IKZF1.
Analysis of the Diagnostic Value of Each Single and Combined Index for Colorectal Cancer
AUC, area under the curve; CI, confidence interval.
Analysis of the correlation between a four-gene combination test and clinicopathologic characteristics of patients with CRC
No statistically significant correlation was found between the positivity rate of the four-gene combination test and the age, gender, history of diabetes, primary tumor location, gross type, TNM stage, or degree of differentiation of patients with CRC (p > 0.05), as presented in Table 5.
Association of Plasmatic Methylated Genes Positivity with Clinicopathological Characteristics of Colorectal Cancer Patients
Discussion
CRC is a preventable cancer, with its pathogenesis varying due to genetic or epigenetic changes. Approximately 70% of patients have sporadic cases. It follows an adenoma-to-cancer progression pattern, which typically takes 5-15 years, providing a window of opportunity for the prevention and early diagnosis of CRC (Markowitz and Bertagnolli, 2009). This makes CRC one of the few malignant tumors that can be screened to reduce morbidity and mortality rates.
CRC screening methods include colonoscopy, FOBT, sigmoidoscopy, colon capsule endoscopy, colon imaging technology, fecal DNA test, blood tumor marker test, and DNA methylation test. Currently, the most common approach to CRC screening involves conducting FOBT for individuals over 40 years old, followed by colonoscopy for high-risk populations. While fecal testing is convenient for sampling, many individuals struggle to accept the fecal collection process. FOBT results can be influenced by food, drugs, and other bleeding disorders, leading to a high rate of false positives and result in instability. Colonoscopy is undoubtedly the gold standard for early CRC screening and diagnosis. However, it is an invasive procedure with low patient compliance. Patients must prepare their intestines in advance, which can result in missed diagnoses if the preparation is inadequate or if the lesion is located in a challenging area to visualize. Additionally, colonoscopy carries risks of bleeding and perforation, and the side effects of general anesthetics during the procedure may not be suitable for elderly individuals and those with cardiorespiratory conditions. Moreover, the current colonoscopy equipment and availability of specialized medical personnel in China are insufficient to meet the demand for widespread CRC screening. Besides, a survey on sample preference during CRC screening revealed that 78% of participants preferred to provide blood samples (Osborne et al., 2018). Blood testing is convenient, easy to implement, and well-received, increasing population screening participation. It has the advantages of high sensitivity and specificity, convenient operation, cost-effectiveness, and practicality. These characteristics make it suitable for early screening of high-risk populations and hold significant application and promotion value.
Epigenetics refers to heritable changes in gene expression that depend on modifications of DNA and histones rather than alterations in the nucleotide sequence. DNA methylation is one of the most common types of epigenetic modification. In tumor cells, DNA methylation inheritance usually manifests as a decrease in the overall methylation level of the genome and an aberrant increase in the methylation level of CpG islands in the promoter regions of specific genes. Several aberrant DNA methylations are associated with early events in CRC and commonly exist in tumor tissues (Esteller, 2005).
A variety of DNA methylation markers has been reported. Most of them focus on single-gene detection, which tends to have low positive detection rates and limitations in the early detection of adenomas or CRC. Multigene methylation detection has emerged as a future trend. Relevant studies have reported on the application of various combined gene methylation assays. For instance, the sensitivity of the combined detection of SFRP2-TFPI2-NDRG4-BMP3 for CRC was 94.3%, which was about 30% higher than that of the single target (Sun et al., 2019b). However, it was also discovered that the compliance rate of the KCNQ5-C9orf50 combined assay was comparable with the performance of the single-targeted assay of C9orf50 (Cao et al., 2021). Therefore, gene combination is essential for CRC diagnosis.
Septin9 is a commonly used molecular marker for CRC screening. However, studies have indicated that its detection rate for early CRC and advanced adenomas is still inadequate when applied alone (Church et al., 2014; Sun et al., 2019a). SDC2, a transmembrane heparan sulfate proteoglycan, has higher mRNA and protein levels in human colon adenocarcinoma tissue samples than in normal epithelial tissues (Ryu et al., 2009). Oh et al. (2013) reported that the sensitivity of the SDC2 gene in serum DNA testing of patients with CRC was 87.0%, and the specificity was 95.2%. IKZF1 is associated with tumor growth and invasion, and its methylation level is elevated in various tumors (Vincent et al., 2011). A study involving over 1,300 participants demonstrated that blood BCAT1/IKZF1 double-gene methylation detection for CRC diagnosis was more sensitive and specific than the fecal immunochemical test (FIT) (Symonds et al., 2016). KCNQ5 belongs to the potassium channel gene family, and research has shown that detecting KCNQ5 has a sensitivity of 83% in CRC (Jensen et al., 2019). All four genes demonstrated specific advantages in individual CRC detection, but the diagnostic performance of the combination of these four genes has not been reported.
In this research, we found that when Septin9, SDC2, IKZF1, and KCNQ5 were tested in combination, the positivity rate of patients with CRC and colorectal polyp was significantly higher than that of the tumor marker CEA test. The diagnostic value of the combined four-gene test for CRC was found to be superior to that of any single-gene test by analyzing the ROC curve. Additionally, it was also found that there was no correlation between the methylation status of Septin9, SDC2, IKZF1, and KCNQ5 genes in plasma ctDNA and the gender, age, history of diabetes, primary tumor location, gross type, TNM stage, and degree of differentiation of patients with CRC (p > 0.05). This suggests that the markers of the four-gene methylations have strong stability in patients with CRC, making them equally efficient in screening for CRC in patients of different ages and pathological stages.
In conclusion, the multigene detection of Septin9, SDC2, IKZF1, and KCNQ5 demonstrates a high diagnostic positivity rate in patients with CRC and those with colorectal polyps, making it a promising indicator for CRC and precancerous lesion screening in clinical practice. This approach may ultimately lead to improved patient outcomes and more effective treatment strategies. However, our study also has some limitations such as (1) the small sample size, (2) the single sample source, and (3) the inability to distinguish between polyps and malignancy. However, if polyps can be detected and resected endoscopically earlier, the trauma and high cost of surgery can be avoided. Therefore, compared with detecting CRC through peripheral blood multigene methylation testing, timely detection of precancerous lesions is more useful and clinically valuable.
Multigene methylation detection involves the extraction and purification of peripheral blood cell-free DNA and uses fluorescence quantitative PCR for detection. This method is simple to operate, cost-effective, does not require special equipment, and is not influenced by factors such as tumor location, age, and tumor type. Once rolled out on a large scale, the cost will be significantly reduced. While multigene methylation detection can overcome the limitations of single-gene detection’s poor sensitivity, there are challenges in its future applications: (1) preclinical studies need to be conducted in various regions to further validate preferred genes; (2) community-based multigene methylation testing has not been performed yet, and traditional screening will persist until substantial evidence from the general population is available; and (3) further exploration is needed to combine it with other molecular detection methods to address the limitations of multigene methylation detection. To draw more convincing conclusions, increasing the sample size, maintaining follow-up, and conducting multicenter comparative studies are essential. Only in this way we can effectively demonstrate the clinical significance of the multigene detection of Septin9, SDC2, IKZF1, and KCNQ5 in CRC screening.
Footnotes
Acknowledgment
This work was supported by Kodia Biotechnology Ltd.
Authors’ Contributions
Y.X.: Conceptualization, methodology, and writing original draft. A.T.: Data curation, visualization, investigation, and writing—reviewing and editing. R.L. and H.Q.: Visualization and investigation; X.L.: Software and validation. Z.W.: Supervision. All authors have contributed significantly and are in agreement with the content of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants from the Tianjin Natural Science Foundation (Grant No.