
Abstract
Background:
Interleukin-10 (IL-10) is an anti-inflammatory cytokine whose levels are elevated in patients with severe COVID-19. IL-10 polymorphisms may play a role in increasing IL-10 levels and the severity of COVID-19. This study aimed to investigate the relationship between IL-10 single nucleotide polymorphisms (SNPs) (rs1800896 [−1082 C < T], rs1800871 [−819 A > G], and rs1800872 [−592 T > G]) and the severity of COVID-19 in patients from Kermanshah Province, Iran.
Methods:
A total of 150 patients with mild COVID-19 (84 men and 66 women aged 40.1 ± 12.44 years) and 143 patients with severe COVID-19 (76 men and 67 women aged 61.04 ± 15.65 years) participated in this study. Blood samples were collected from the patients, DNA was extracted, and the genotype of each SNPs was determined using the polymerase chain reaction-restriction fragment length polymorphism method.
Result:
The results of this study did not show a significant relationship between the genotypes of the three studied SNPs and the severity of COVID-19 (p > 0.05).
Conclusion:
According to our findings, these SNPs were not associated with COVID-19 severity in patients in Kermanshah.
Introduction
The global pandemic of coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), originated in the Chinese city of Wuhan and spread rapidly around the world (Chams et al., 2020). COVID-19 is associated with increased production of inflammatory cytokines such as interleukin-6 (IL-6), IL-1, IL-4, IL-18, IL-33, interferon-γ (IFN-γ), tumor necrosis factor-alpha (TNF-α), and the inhibitory cytokine IL-10 (Falahi et al., 2022; Rezaei, 2021).
IL-10 plays an important role in inhibiting inflammatory responses (Saraiva et al., 2019). It is produced by almost all immune cells, such as dendritic cells, macrophages, B cells, T cell subsets, neutrophils, and nonimmune cells, including keratinocytes and epithelial cells, in response to infection or tissue injury (Iyer and Cheng, 2012). The increase in IL-10 levels in COVID-19 is caused by different mechanisms. Given that COVID-19 is associated with a severe inflammatory response, it is believed that increased IL-10 levels are a form of negative feedback mechanism that reduces inflammation. A high IL-10 level indicates poor prognosis. The data also revealed that levels of IL-10 increased earlier than IL-6 in patients with COVID-19 (Lu et al., 2021). Like other proteins, cytokine production is regulated by genes and genetic factors. Differences in the gene sequences, including the promoter and control regions, cause differences in the expression of the corresponding proteins. Single nucleotide polymorphisms (SNPs) are the most common types of genetic variation among individuals. Studies have shown that SNPs are associated with the susceptibility to viral respiratory infections. They are also important for host resistance to diseases and disease severity (Adli et al., 2022; Karcioglu Batur and Hekim, 2021). Studies have shown that polymorphisms in the IL-10 gene promoter in rs1800896 (−1082 C < T), rs1800871 (−819 A > G), and rs1800872 (−592 T > G) affect IL-10 serum levels and the occurrence and development of various diseases, including systemic lupus erythematosus, pemphigus vulgaris, nephropathy, and breast cancer (Gao et al., 2017; Javor et al., 2010; Li et al., 2022; Mohammadi et al., 2019).
This research aimed to investigate the potential relationship between IL-10 SNPs (rs1800896 [−1082 C < T], rs1800871 [−819 A > G], and rs1800872 [−592 G > A]) and the severity of COVID-19 disease among patients in Kermanshah, one of the Kurdish cities of Iran.
Materials and Methods
Study design
This study included 143 patients with severe COVID-19 and 150 patients with mild COVID-19. All patients had a positive reverse transcription-polymerase chain reaction test for SARS-COV-2 infection in nasopharyngeal samples. Patients were classified into mild and severe groups based on the severity of their clinical symptoms, level of pulmonary involvement, and blood oxygen saturation (SpO2). Patients with mild symptoms of fever, fatigue, gastrointestinal symptoms, loss of sense of smell and taste, mild respiratory symptoms, and SpO2 >90% were considered to have mild COVID-19, and patients with respiratory rate (RR) ≥30, SpO2 <90, and lung involvement of >50% on CT scans were considered to have severe COVID-19. Mild patients were referred to the Clinic of Samen Al-A’meh of Kermanshah, and severely ill patients were admitted to Imam Reza Hospital in Kermanshah.
All patients were from Kermanshah, one of the Kurdish cities in western Iran. All patients signed the informed consent form. This study was approved by the Ethics Committee of the Kermanshah University of Medical Sciences with reference code: IR.KUMS.REC.1401.123 in June 2010.
Sample collection
Five milliliters of blood was taken from each patient, and DNA was extracted using the salting-out method. Polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) was used to genotype three SNPs in the IL-10 gene promoter region. The primers used in the PCR-RFLP for IL-10 SNP genotyping are listed in Table 1.
PCR and RFLP Conditions for IL-10 Polymorphism Identifications
IL, interleukin; PCR, polymerase chain reaction; RFLP, restriction fragment length polymorphism.
Polymerase chain reaction reaction-restriction fragment length polymorphism
To perform PCR-RFLP, extracted DNA containing the IL-10 promoter was amplified by PCR. PCR was performed in a volume of 15 μL of the reaction mixture, including 5.5 μL of purified water, 1 μL of forward and reverse primers, 0.5 μL of DNA, and 7 μL of the master mix (Sinacloon, Tehran, Iran). PCR steps included 3 min at 95°C for initial denaturation, 34 cycles of denaturation for 45 s at 94°C, 30 s at 58°C for annealing for all SNPs, and a final extension step at 72°C for 2 min, using an iCycler C1000 machine (Bio-Rad Life Sciences, Hercules, CA, USA). The PCR product lengths for rs1800871, rs1800872, and rs1800896 were 606 bp, 309 bp, and 160 bp, respectively. The PCR products were subjected to enzymatic digestion using a restriction enzyme specific to each SNP, and the resulting product was electrophoresed on a 2% agarose gel.
Electrophoresis on agarose gel
The 606 bp PCR product for rs1800871 (−819 A > G) was digested with MSlI (Rsel) restriction enzyme for 16 h at 37°C, and the digested product was electrophoresed on an agarose gel. The PCR product containing the G allele was cut by the Rsel enzyme into two fragments of 371 bp and 235 bp, but the product containing the A allele was not sensitive to the restriction enzyme, leaving the 606 bp fragment intact. If a PCR product formed two bands of 371 bp and 235 bp after enzymatic digestion, it was classified as GG homozygous. However, if it formed three bands at 371 bp, 235 bp, and 606 bp, it was classified as heterozygous AG, and if it formed only one band at 606 bp, it was classified as homozygous AA (Fig. 1).

Restriction digestion (Rsel) products of the IL-10 rs1800871 A > G polymorphism in the promoter region on a 2% agarose gel. Homozygous wild-type AA genotype (606 bp); heterozygous AG genotype (606 bp + 371 bp + 235 bp); and homozygous mutant GG genotype (371 bp + 235 bp).
The 309 bp PCR product for rs1800872 (−592 T > G) was digested with the restriction enzyme Rsal for 16 h at 37°C, and the digested product was electrophoresed on an agarose gel. The PCR product containing the T allele was cut by the Rsal enzyme and broken into two fragments of 122 and 187 bp. However, the product containing the G allele was not sensitive to the restriction enzyme and, as a result, the 309 fragment remained intact. If the PCR product formed two bands of 122 bp and 187 bp after enzymatic digestion, it was classified as TT homozygous. However, if three bands of 122, 187, and 309 bp were formed, they were classified as GT heterozygous; if only one band of 309 bp was formed, they were classified as GG homozygous (Fig. 2).
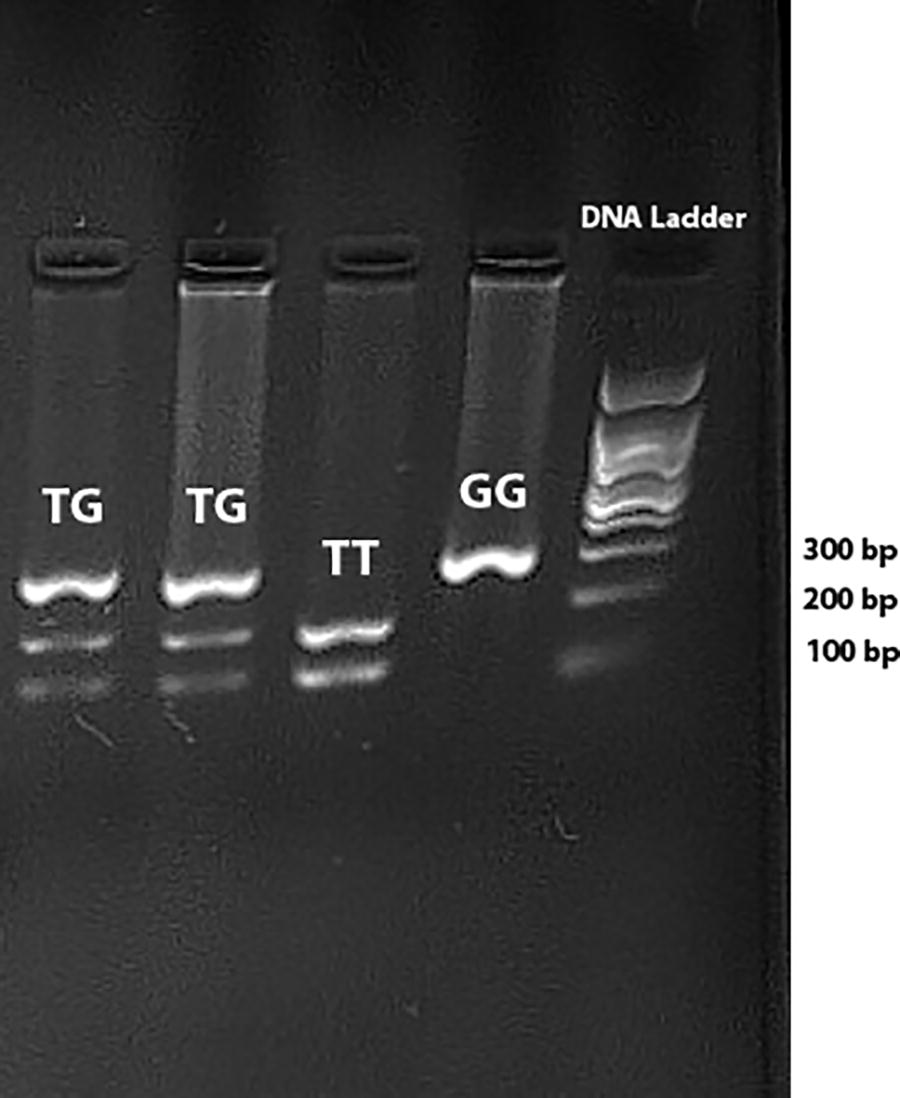
Restriction digestion (Rsal) products of the IL-10 rs1800872 T > G polymorphism in the promoter region on a 2% agarose gel. Homozygous wild-type TT genotype (122 bp + 187 bp); heterozygous TG genotype (309 bp + 122 bp + 187 bp); and homozygous mutant GG genotype (309 bp).
The 160 bp PCR product for rs1800896 (−1082 C < T) was digested by BSRBI enzyme for 16 h at 37°C, and the digested product was electrophoresed on an agarose gel. The PCR product containing the C allele was cleaved by the BSRBI enzyme into two fragments of 28 bp and 132 bp, but the product containing the T allele was resistant to the enzyme, leaving the 160 bp fragment intact. Due to the small size of the 28 bp fragment, it was removed from the gel by separating the two bands at 160 and 132 bp. Therefore, if the PCR product after enzymatic digestion led to the formation of a 132 bp band, it was classified as CC homozygous. However, if it led to the formation of 132 and 160 bp bands, it was classified as heterozygous CT; if it led to the formation of only one 160 bp band, it was classified as homozygous TT (Fig. 3).

Restriction digestion (BSRBI) products of the IL-10 rs1800896 T > C polymorphism in the promoter region on a 2% agarose gel. Homozygous wild-type TT genotype (160 bp); heterozygous CT genotype (160 bp + 132 bp); and homozygous mutant CC genotype (132 bp). Due to the small size of the 28 bp fragment, it was removed from the gel by separating the two bands at 160 and 132 bp.
Statistical analysis
IBM SPSS software package version 22 and Excel 2019 were used to analyze the data and draw graphs. A chi-square test was performed to compare the genotypes and allelic frequencies of SNPs between patients with severe and mild forms of COVID-19. The chi-square test was also used to evaluate the Hardy-Weinberg equilibrium (HWE) for all three SNPs in the patients with severe and mild COVID-19. To determine the consequences of these changes, odds ratio and 95% confidence intervals (CIs) were calculated using logistic regression. Statistical significance was set at p ≤ 0.05.
Results
The relationship between age and disease severity
A total of 143 patients with severe form (76 men, 67 women, aged 61.04 ± 15.65 years) and 150 patients with mild form of COVID-19 (84 men, 66 women, aged 40.1 ± 12.44 years) participated in this study. There was no significant difference between the two groups in terms of sex distribution (p = 0.62), but the average age of patients with the severe form of COVID-19 was higher than that of patients with the mild form of COVID-19, and this difference was statistically significant (p > 0.0001).
Correlation of IL-10 gene polymorphisms with the severity of COVID-19
In this study, three different polymorphic regions, rs1800896 (−1082 C < T), rs1800871 (−819 A > G), and rs1800872 (−592 T > G), were selected from the IL-10 promoter and their relationship with the severity of COVID-19 were investigated. Table 2 displays the spread of genotypes, frequencies of alleles, and various genetic models (dominant, additive, and recessive) among individuals affected by severe and mild cases of COVID-19. Examination of SNPs in terms of HWE showed that except for rs1800896, the others did not show detectable deviation from HWE.
Distribution of Allele and Genotype Frequencies of IL-10 Gene Polymorphisms in Patients with Severe and Mild COVID-19 and Controls
CI, confidence interval; HWE, Hardy-Weinberg equilibrium; OR, odds ratio; SNP, single nucleotide polymorphism.
The results of this study showed that there was no statistically significant difference between patients with severe COVID-19 and those with mild COVID-19 in terms of allele and genotype distribution of all three studied SNPs or in terms of different genetic models (dominant, additive, and recessive).
Discussion
IL-10 is an inhibitory cytokine whose serum levels have been shown to increase in proportion to the severity of COVID-19. Single nucleotide polymorphisms (SNPs), especially in cytokine gene regulatory regions, are associated with differences in cytokine production (Haukim et al., 2002). In this study, we investigated the relationship between three SNPs in the IL-10 promoter (rs1800896 [−1082 C < T], rs1800871 [−819 A > G], and rs1800872 [−592 T > G]) and the severity of COVID-19 in people with COVID-19 in Kermanshah, Iran. The results of this study showed that there was no statistically significant difference in the distribution of genotypes and the frequency of IL-10 SNP alleles (rs1800896 [−1082 C < T], rs1800871 [−819 A > G], and rs1800872 [−592 T > G]) between patients with mild COVID-19 and patients with severe COVID-19.
IL-10, also known as human cytokine synthesis inhibitory factor (Vojgani, 2020), is produced by various cells, such as CD8+ and CD4+ T cells, regulatory T cells, natural killer (NK) cells, NK T cells, B cells, dendritic cells, eosinophils, mast cells, monocytes, and macrophages (Laurent and Shapiro, 2006). It reduces the production of Th1 cytokines and expression of MHC class II and co-stimulatory molecules in macrophages. It can also inhibit NF-κB activation but improves B cell survival and antibody production (Abbas et al., 2021). IL-10, when produced in response to or in combination with inflammatory cytokines, such as IL-6, IL-8, IL-4, and TNF-α, can trigger a cytokine storm (Barrett, 2019; Niedźwiedzka-Rystwej et al., 2022). Although the inflammatory response protects the body against harmful stimuli in its severe form, as seen in cytokine storm syndrome, it can cause severe organ damage and even death (Mangalmurti and Hunter, 2020). Cytokine storm and lymphopenia are hallmarks of immunopathology in viral infections, such as SARS-CoV, MERS-CoV, and SARS-CoV-2 (Channappanavar and Perlman, 2017; Gupta et al., 2019; Yang et al., 2020). Studies have shown that the serum level of IL-10 increases in people with severe COVID-19, and this cytokine is considered a predictor of the severity of the disease (Han et al., 2020, Soltani-Zangbar et al., 2022).
In this study, we did not find a significant relationship between any of the three studied SNPs and the severity of COVID-19. Consistent with our findings, in a recent study by Rizvi et al., no association was found between the rs1800872 variant (−592T > G) and the severity of COVID-19. However, they found a significant association between rs1800896 (−1082C < T) and the severity of COVID-19. In addition, while the frequencies of the TT and CC genotypes were higher in the severe group than in the mild group (65.3% vs. 52.9% and 4% vs. 2.4%, respectively), the frequency of the CT genotype was lower in the severe group than in the mild group (30.7% vs. 44.7%) (Rizvi et al., 2022). In contrast to the current study, Abood and colleagues (Abbood et al., 2023) found associations between specific IL-10 SNPs (rs1800896 [−1082C < T], rs1800871 [−819A > G], and rs1800872 [−592T > G]) and COVID-19 mortality in various virus variants among some Iranian population. It is important to note that their study examined recovered and deceased patient groups, differentiating it from the current study in terms of the study population.
In our study, the frequencies of CT and CC genotypes were higher in the severe group than in the mild group (53.1% vs. 52.7% and 4.2% vs. 3.3%, respectively). However, the frequency of the TT genotype was higher in the mild group than that in the severe group (44% vs. 42.7%). In a study by Felix et al., no significant relationship was found between genotypes and allelic frequencies of rs1800872 (−592T > G) and rs1800871 (−819A > G) in both critical and noncritical groups. Therefore, these two polymorphisms have not been identified as risk factors for death due to COVID-19 (Avendaño-Félix et al., 2021). Batur and Hekim, by reviewing the literature on some cytokine gene polymorphisms associated with the incidence of COVID-19 and mortality in 23 countries, showed that polymorphisms of rs1800896 in IL-10, rs2275913 in IL-17A, and rs763780 in IL-17F may explain variations in the prevalence of COVID-19 and mortality in different countries (Karcioglu Batur and Hekim, 2021). Although the relationship between the rs1800896 genotype and the severity of COVID-19 can be indirectly inferred from the results of this study, one notable weakness is that the researchers examined the mortality and prevalence of COVID-19 on only two specific days (September 7, 2020, and December 6, 2020). In contrast, in a similar study, no association was found between rs1800896 and rs1800871 variants of IL-10 and the prevalence and mortality rate of COVID-19 (Batur and Hekim, 2020).
The association of IL-10 SNPs with other respiratory diseases, such as influenza, acute respiratory distress syndrome (ARDS), and neonatal bronchiolitis, has also been investigated. For example, Gong et al. confirmed the relationship between the IL-10 rs1800896 CC genotype and age and the development of ARDS and showed that in 52-year-old subjects, the CC-1082 genotype was significantly associated with an increased risk of ARDS (odds ratio [OR] = 3.9; 95% CI [1.8-8.6]; p < 0.001) (Gong et al., 2006). In a study by Holster et al., infants with rhinovirus bronchiolitis had a lower proportion of IL-10 rs1800896 CT or CC genotype (27.3%) than controls (65.5%, p = 0.009). However, their study found no association between IL-10 genotypes (rs1800871 and rs1800872 (and viral causes of neonatal bronchiolitis. In contrast, in a study conducted by Rogo in Iran, the GG and TG genotypes of IL-10 (rs1800872) were found to be significantly associated with an increased risk of severe influenza. This suggests that carriers of GG and TG (IL-10 rs1800872) are more likely to develop severe A/H3N2 influenza virus infection (Rogo et al., 2016). In a similar study conducted by Keshavarz et al. in Iran, no correlation was found between the frequency of IL-10 rs1800872 genotypes and influenza A/H1N1 or influenza B disease (Keshavarz et al., 2019). Considering that in both studies, sampling was done from the National Influenza Center of Tehran University of Medical Sciences, probably because of the larger number of samples in the first study, its results are more reliable.
Conclusion
The results of our study did not show a significant association between three SNPs identified in the promoter region of IL-10 (rs1800896 [−1082C < T], rs1800871 [−819A > G], and rs1800872 [−592T > G]) and the severity of COVID-19 in patients of Kermanshah, Iran. This could be due to the ethnic difference of our study population, patients in Kermanshah, with the population studied in other studies, although the role of other factors, such as sample size, cannot be ignored. Future genetic studies should involve a greater number of participants and a wider array of SNPs to elucidate the association between genetic variations in IL-10 and SARS-CoV-2 infection.
Footnotes
Acknowledgment
The authors would like to acknowledge the Deputy of Research and Technology of Kermanshah University of Medical Sciences for financial support.
Authors’ Contributions
A.G.K. took part in the study’s concept and design. The article was written by H.A. All authors contributed to data collection, analysis, and interpretation, and they all approved the final publication.
Author Disclosure Statement
The authors state that they do not have any known competing financial interests or personal ties that could appear to have influenced the work provided in this study.
Funding Information
This study was funded by the Deputy of Research and Technology of the Kermanshah University of Medical Sciences (4010214).