
Abstract
Abstract
Introduction
The overall incidence of splenectomy during surgery for advanced ovarian cancer is not known; however, it is thought to be increasing with the trend toward more aggressive cytoreduction. One recent series of 194 patients with advanced disease utilized splenectomy in 6% of cases. 3 Splenic involvement in ovarian cancer has been reported to be as high as 20% either via extensive abdominal carcinomatosis or solitary metastasis. 4 The known complications of a splenectomy include pleural effusions, pneumonia, thrombocytosis with thromboembolism, pancreatic injury, and postoperative sepsis. A recent series of 112 patients who underwent splenectomy during primary or secondary cytoreductive surgery for ovarian cancer revealed short-term complications including wound infection, pneumonia, thromboembolic events and sepsis, and a perioperative mortality rate of 5%. 5
Recent studies, including Gynecological Oncology Group (GOG) 172, have shown a significant survival advantage for those patients who undergo intraperitoneal (IP) chemotherapy with a platinum agent and Taxol (paclitaxel) versus those who undergo intravenous (IV) chemotherapy. A 15.9-month OS advantage was noted in GOG 172 (p = 0.03) and these results are consistent with two previous GOG trials.6–8 Additionally, a 5-month increase in progression-free interval was noted for those patients undergoing IP chemotherapy versus those who received IV therapy. 6 Concurrent with the publication of GOG-172, the National Cancer Institute issued a clinical announcement supporting the use of IP chemotherapy in patients with advanced ovarian cancer who had undergone optimal cytoreductive surgery.9–11
While IP chemotherapy has demonstrated an improvement in OS and progression-free survival (PFS), it has also been associated with an increased rate of toxic side-effects. Only 42% of the IP patients in GOG 172 were able to complete six cycles and only 48% completed three or four cycles. While patient quality of life 1 year after completion of therapy was comparable between the groups, there was a significantly increased rate of short-term toxicities in the IP group. Patients randomized to receive IP therapy experienced increased pain, fatigue, leukopenia, infection, thrombocytopenia, gastrointestinal, metabolic, and neurologic toxicities compared to those randomized to IV therapy. 6
A review of the patients from GOG 172 examined those surgical procedures required to achieve optimal cytoreduction and the subsequent ability of the patients to initiate or tolerate IP chemotherapy. The procedures examined were hysterectomy, appendectomy, right colon resection, left colon or rectosigmoid resection, colostomy, and small bowel resection. The only surgery that was associated with a decreased ability of patients to initiate or tolerate IP chemotherapy was left colon or rectosigmoid resection. 12 Another earlier review of 227 patients undergoing IP chemotherapy found an increased (though not statistically significant) rate of catheter related infections and IP chemotherapy-related toxicity in those patients who had undergone gastrointestinal surgery at the time of cytoreduction. 13
While there have been studies examining the ability of patients to tolerate IP chemotherapy after undergoing cytoreductive surgery including multiple bowel resections, there has been no investigation into the ability of patients to tolerate IP chemotherapy after surgery including splenectomy. Splenectomy is associated with increased rates of short-term morbidity, is a marker of upper abdomen disease, and may result in decreased levels of immunocompetence. These factors, theoretically, may make a course of IP chemotherapy more difficult to tolerate. The aim of this study is to determine the ability of patients to tolerate IP chemotherapy after optimal cytoreductive surgery that includes splenectomy.
Study Design
All patients from January 1, 2005 to December 31, 2007 with primary or recurrent high-grade stage III ovarian cancer who had undergone optimal cytoreductive surgery to <1 cm of residual disease and subsequently underwent IP chemotherapy with a platinum agent and paclitaxel at our institution were identified from a tumor registry database. Individual subject data were collected retrospectively from inpatient and ambulatory medical records. Surgical and pathology reports from primary or secondary surgeries were reviewed in all cases. The following information was abstracted from a database that had been previously approved by the Johns Hopkins Hospital Institutional Review Board: Patient age and date of diagnosis, International Federation of Gynecology and Obstetrics stage of disease, number of cycles of IP chemotherapy, type of chemotherapy, number and type of bowel resection, pelvic or abdominal peritoneum stripping, liver resection, lymph node dissection, GOG score, and cytoreduction status. Surveillance information included the date of last follow-up and disease status or date of death. Thirty (30)-day morbidity was also calculated and included these events occurring within 30 days of surgery: Pulmonary embolus, deep vein thrombosis, intraabdominal or pelvic abscess, pneumonia, wound infection, bacteremia, or urosepsis.
Unpaired t-tests and Fisher's exact test were used to compare patient characteristics. Kaplan-Meier survival analysis and unpaired t-tests were then used to calculate and compare PFS, 30-day morbidity from the date of surgery, and completion of a full six cycles of IP chemotherapy. All confidence intervals are at the 95% level and all p-values are two sided with a value ≤0.05 considered significant. MedCalc software was used for all calculations.
Results
A total of 41 patients who met study inclusion criteria were identified. Thirteen (13) patients underwent splenectomy (33.3%) and 28 (66.6%) did not have a splenectomy performed during optimal cytoreductive surgery (OCRS). The average age of patients who underwent a splenectomy was 58 years and the average age of patients who did not undergo splenectomy with OCRS was 62 years, and this difference was not statistically significant (p = 0.15). The average GOG score for patients undergoing splenectomy was 0.47 and for those not undergoing splenectomy was 0.35 (p = 0.75). The patients were well matched in terms of stage, grade, and histology. Thirty-eight percent (38%) of patients who underwent splenectomy did so in the setting of recurrent disease, while 18% of the patients in the control group had recurrent disease (p = 0.24) (Table 1).
GOG, Gynecological Oncology Group.
The surgical procedures required to achieve optimal cytoreduction included hysterectomy, lymph node dissection (pelvic and/or periaortic), liver wedge resection, diaphragm stripping or resection, large bowel resection, small bowel resection, and stripping of the peritoneum of the pelvis or abdomen, in addition to splenectomy. The patients were well matched with no significant differences noted in the use of any of the surgical procedures for those patients who underwent splenectomy compared to those who did not undergo splenectomy (Table 2).
Fifty-four percent (54%) of the splenectomy patients had an episode of perioperative morbidity (defined as an event that occurred within 30 days of surgery including thrombolic event, intraabdominal abscess, pneumonia, wound infection, bacteremia, and urosepsis). Fourteen percent (14%) of the control group had such an event. This was a statistically significant difference (p = 0.02) (Table 3).
All patients underwent IP chemotherapy with a platinum agent and paclitaxel in a dosing regimen consistent with GOG 172. Sixty-nine percent (69%) of patients who underwent splenectomy were able to complete a full six cycles of IP chemotherapy. Seventy-one percent (71%) of those patients who did not undergo splenectomy were able to complete six cycles of IP chemotherapy. The difference was not statistically significant (p = 0.33). The mean number of IP cycles completed by patients after splenectomy was 4.7 and the mean number following surgery without splenectomy was 5.4 (p = 0.21) and was not statistically different. The median PFS for patients who underwent splenectomy was 9 months versus 16 months for patients who did not (p = 0.13). Median survival had not been reached at the time of analysis (Table 4).
PFS, progression-free survival.
Discussion
This study is the first one to examine the ability of patients with advanced ovarian cancer to tolerate IP chemotherapy after cytoreductive surgery involving a splenectomy. Our data suggest that patients who undergo splenectomy at the time of OCRS are just as able as those who did not have a splenectomy to complete a full course of IP chemotherapy (Table 4).
The patients were well matched in terms of age, stage, grade, histology, GOG score, bowel resections, and extent of surgery (Tables 1 and 2). These may all be factors that play a role in a patient's ability to tolerate the increased toxicity of IP chemotherapy. With these variables accounted for, it becomes possible to evaluate the effect that splenectomy will have. It is well established that splenectomy is associated with increased perioperative and postoperative morbidity. Overwhelming postsplenectomy infection (OPSI) is a rare but catastrophic event associated with splenectomy. The incidence of infection after splenectomy has been estimated to be 3.2% with a mortality rate of 1.3%. 14 In the setting of an OPSI, the mortality rate jumps to greater than 50%. 15
There are several limitations of the current study that must be considered when interpreting the data. First and foremost is the retrospective methodology, which introduces the potential for selection bias. In order to minimize the potential for bias, consecutive cases were collected, including patients with recurrent disease, so as to generate as complete a picture as possible of the potential impact of splenectomy on patients undergoing IP chemotherapy. Another potential source of bias is the selection of patients undergoing IP versus IV chemotherapy after cytoreductive surgery including a splenectomy. During the time frame of this study, a splenectomy was performed 29 times for primary or recurrent ovarian cancer at Johns Hopkins Hospital. Thirteen (13) of these patients met inclusion criteria for this study. Of the 16 patients who were not included, 7 received their chemotherapy from a medical oncologist (at an outside institution) who recommended IV chemotherapy or were lost to follow-up. Additionally, the small sample size is a confounding factor.
Conclusions
Ovarian cancer often presents with bulky upper abdominal disease. The accepted treatment paradigm for these patients is resection of disease and adjuvant chemotherapy. IP chemotherapy has become an integral part of treatment for advanced ovarian cancer once optimal cytoreduction has been achieved. Additionally, much of the current literature suggests that increasingly aggressive surgical cytoreduction results in improved patient outcomes. 2 However, it is unclear how those patients who are undergoing such radical surgical procedures in order to achieve maximal cytoreduction are able to tolerate the rigors of IP chemotherapy. In order to achieve maximal cytoreduction, a number of surgical procedures may be required, including splenectomy. While our data show a statistically significant increase in perioperative morbidity for patients undergoing splenectomy, they also demonstrate no difference in number of cycles of IP chemotherapy or percent of patients undergoing the recommended six cycles (Tables 3 and 4). Although there is an increased rate of events within the first 30 days of surgery that may require supportive care for patients after splenectomy, this does not appear to impair their ability to tolerate IP chemotherapy. Additionally, the median PFS is comparable in the two groups (Fig. 1). This is encouraging to gynecologic oncologists to continue on the course of maximal cytoreductive surgery and adjuvant (IP) chemotherapy and to perform a splenectomy if it will result in OCRS.
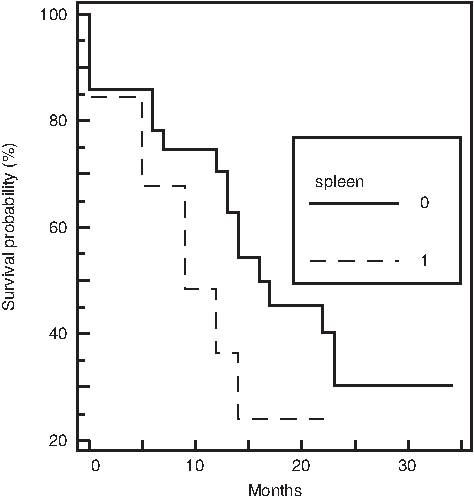
Splenectomy progression-free survival (PFS). Kaplan-Meier curve comparing median PFS of patients who underwent splenectomy versus those who did not. Median PFS was 9 months in the splenectomy group and 16 months in the control group (p = 0.13).
Footnotes
Disclosure Statement
No competing financial interests exist.