
Abstract
Abstract
Introduction
A preoperative diagnosis of ovarian pregnancy is not always possible, although some cases have been diagnosed by high resolution ultrasounds, used early to diagnose pregnancy following ART. Only 2 cases of ovarian pregnancy with the use of clomiphene citrate have been reported in the literature. A case of ovarian pregnancy in a PCOS patient who underwent ovulation induction with clomiphene citrate is reported here, because of its rarity.
Case
A 24 year old woman, married for 2 years, consulted a physician for primary infertility. She had attained menarche at 13, and her cycles had been irregular since that age, with her flow lasting for 3–5 days during every 40–50 day cycle. On general examination, this patient was found to be slender with a body mass index (BMI) of 22. She was hirsute and had acne but and no acanthosis nigricans. The systemic examination was normal, a gynecologic examination revealed a normal-sized uterus, and her fornices were free. Semen analysis of her husband was within normal limits. A transvaginal ultrasound showed polycystic ovaries. A hormonal profile performed on the third day of her cycle revealed a follicle-stimulating hormone (FSH) level of 5, a luteinizing hormone (LH) level of 3.1 international units (IU)/mL, and a normal serum prolactin level. Her serum testosterone level was 57.21 and her estradiol level was 37.5 pg/mL. Her thyroid profile and glucose tolerance test results were normal. She was treated with tabKrimson 35 (estradiol and cypropterone acetate) for three cycles. Subsequently, ovulation induction was started with clomiphene citrate at 50 mg from day 2 to day 6 of her cycle, and 500 mg of metformin, used off-label for PCOS, thrice daily throughout the cycle. She could not come to the medical facility for follicular monitoring, because she would have had to travel a long distance. She was advised to engage in coitus during her the fertile period. After her second cycle, she presented with painless bleeding of 2 days' duration, after 50 days of amenorrhea, simulating her normal periods. A transabdominal ultrasound did not reveal any gestational sac.
She was sent home with the advice to come for follicular monitoring during her next cycle, but she then presented to the emergency room (ER) the next day with pain in her lower abdomen, and a transabdominal ultrasound revealed an adnexal mass with minimal free fluid in the pouch of Douglas. Her serum β-hCG was 1000 IU/mL. A transvaginal ultrasound revealed an extrauterine gestational sac of 2.5×3 cm with a yolk sac (Fig. 1) and free fluid in her pelvis. Medical management was deferred, and an emergency laparotomy was performed because of the lack of facilities for emergency laparoscopic surgery in the ER.
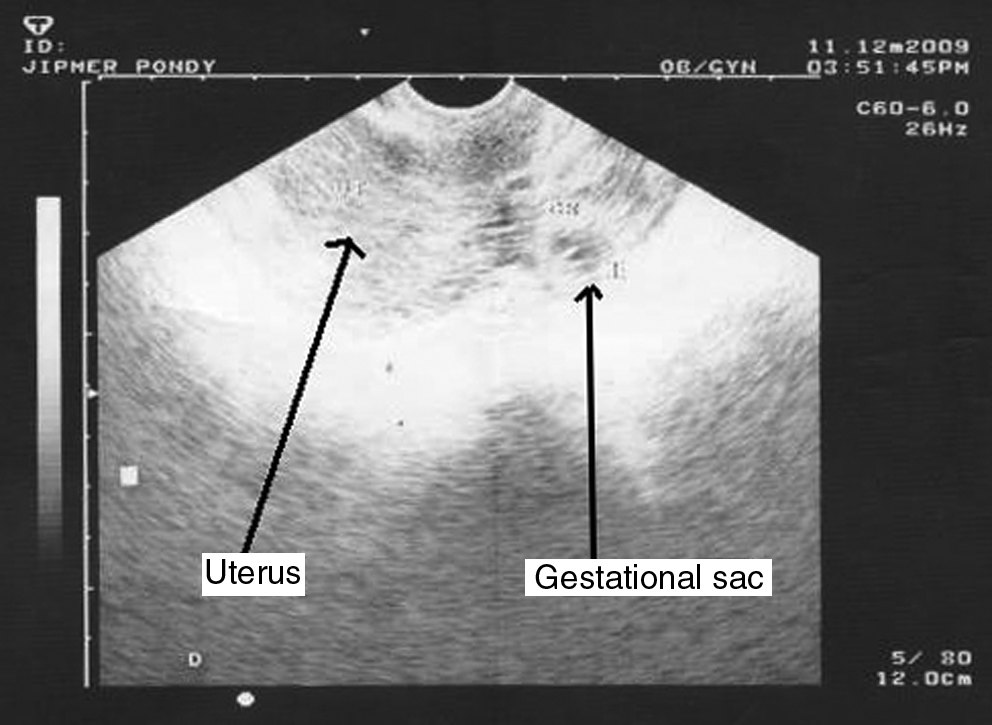
Transvaginal ultrasonographic picture shows extrauterine gestational sac.
At the laparotomy, dark-colored thick blood (∼150 mL) was noted in her pelvis. Both tubes were normal. Her left ovary was polycystic, and her right ovary was enlarged with a dark hemorrhagic cystic mass of 3×3 cm (Fig. 2), from which thick blood was oozing. There were no adhesions. The ovary was separated from the fallopian tube and the gestational sac occupied the ovary, which, in turn, was attached to the uterus by the ovarian ligament. A diagnosis of ovarian ectopic pregnancy was made and resection of the ectopic mass was undertaken. The surface of the ovary was felt to be very thick when the excision was undertaken, and bilateral ovarian drilling was also performed. The histopathologic examination (Fig. 3) of the resected specimen was consistent with ovarian pregnancy. The case fulfilled the criteria proposed by Spiegelberg for the diagnosis of primary ovarian pregnancy. 10

Laparotomy picture: shows hemorrhagic mass on the surface of the left ovary.
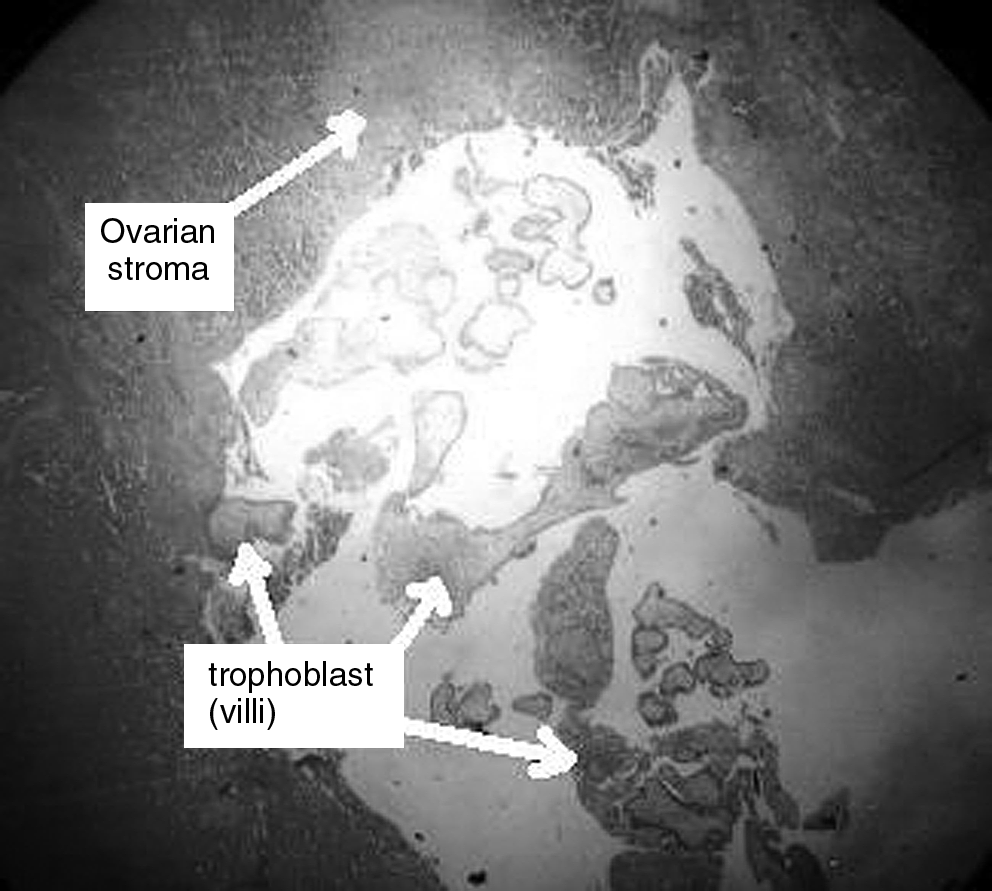
Histopathologic picture showing ovarian tissue and trophoblastic tissue.
Results
The patient returned for follow-up. She was advised to wait for 6 months for spontaneous conception. After 6 months, she was given clomiphene citrate at the same dose (50 mg for 5 days starting on day 2 of her menstrual cycle), and she conceived during her second cycle. She had an intrauterine pregnancy and her delivery was managed in her home town.
Discussion
Ectopic pregnancy is an important cause of maternal mortality, and its incidence is reported to be increased by fourfold with the use of clomiphene citrate or gonadotropin therapy. 11 Although ovarian pregnancy is one of the least-common ectopic pregnancies, accounting for 0.2% of all ectopic pregnancies, according a source in 2009, its incidence has increased, and was noted as constituting up to 3.2% of all ectopic pregnancies in an earlier 10-year population-based study in 2002. 4 The various risk factors recently reported for ovarian ectopic pregnancy include use of intrauterine contraceptive devices (IUCD),1,3,12 ovarian hyperstimulation, intrauterine insemination,7,13 in vitro fertilization, and embryo transfer.8,9
Ovarian pregnancy concurrent with intrauterine pregnancy following ovulation induction with clomiphene citrate was reported by Phillips in 1979. 14 The present case did not have any risk factors for ovarian pregnancy other than ovulation induction. There were no features of ovarian hyperstimulation observed in the present case, unlike that reported by Einenkel and collegues. 7 PCOS needs to be considered as a risk factor for the development of ovarian ectopic pregnancy, as, in this case, the ovarian capsule was felt to be tough and offered resistance when ovarian drilling was undertaken at the time of the resection of the ovarian ectopic pregnancy. Because of the thick capsule, the ovum would not have been released, and fertilization would have probably taken place on the surface of the ovary, resulting in a primary ovarian pregnancy.
Diagnosis of ovarian pregnancy was possible preoperatively in a few cases by transvaginal ultrasound,4,8,9 and some cases have been diagnosed only by laparoscopy7,13 or laparotomy. 4 In the present case, although an extrauterine gestational sac was seen on a transvaginal ultrasound, the entire ovary could not be visualized. It was interpreted as a ruptured ectopic pregnancy; however, the ovary as the site of the ectopic pregnancy was not considered. Laparoscopic management is the present-day method of choice in ruptured ectopic pregnancies3,7 when a patient is hemodynamically stable. This option could not be chosen in this case, because of a lack of facilities. Resection of an ovarian ectopic pregnancy, rather than an oopherectomy, should be undertaken whenever possible, especially in a patient with infertility, to preserve the ovarian reserve.
Conclusions
The case illustrates the fact that it is easy to miss an ectopic pregnancy if a transvaginal ultrasound is not performed. The clinical presentation of ectopic pregnancy can mimic the menstrual pattern in PCOS. PCOS may be one of the factors predisposing a patient to ovarian ectopic pregnancy because of the thick ovarian surface.
Footnotes
Disclosure Statement
No competing financial conflicts exist.