
Abstract
Abstract
Introduction
Case
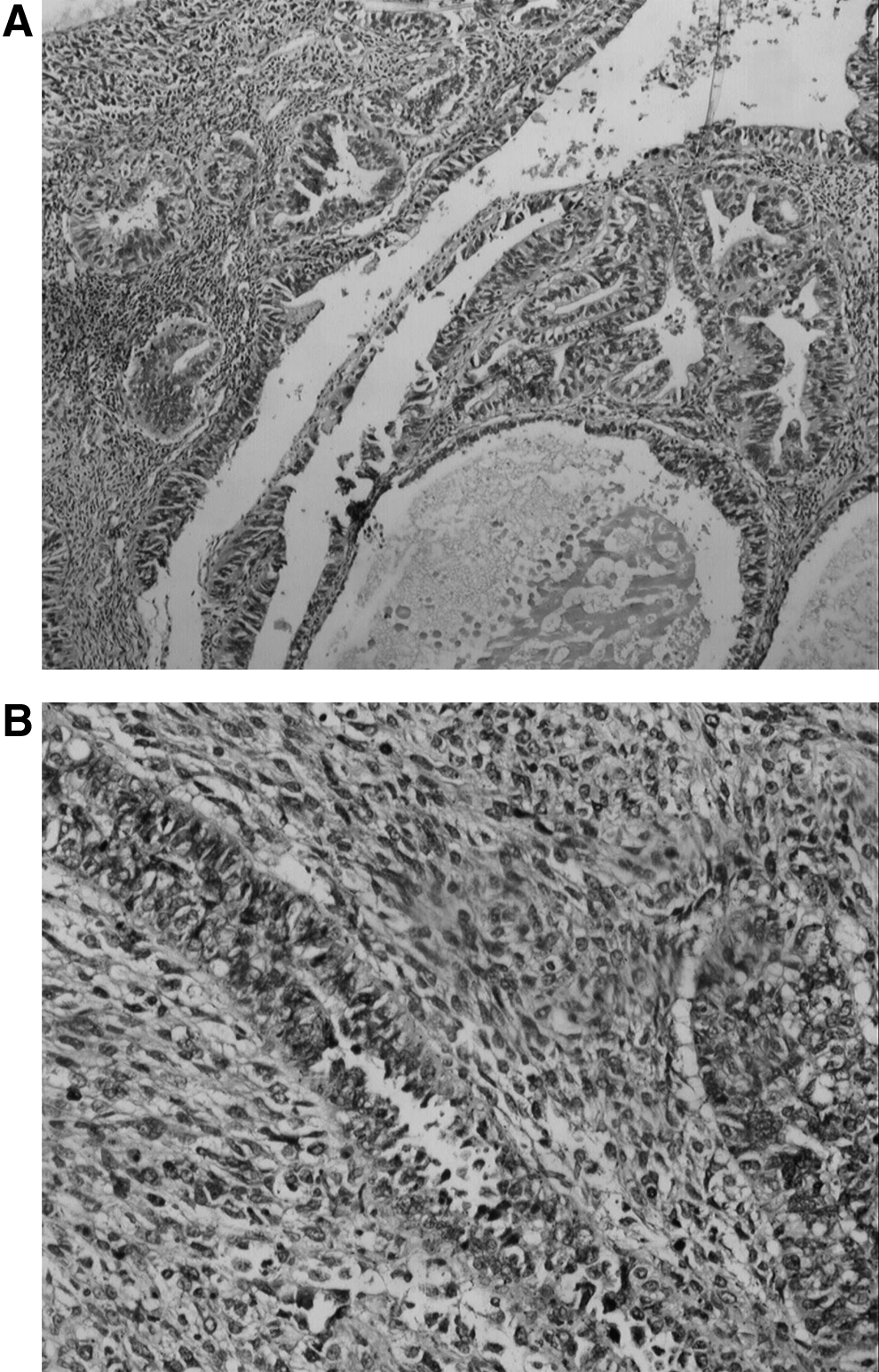
In 2005, a 65-year-old multiparous woman presented with invasive ductal breast cancer. She had been postmenopausal for 17 years. A mastectomy and axillary dissection was performed and the tumor was staged pT4, N1, M0. Immunohistochemical staining of the tumor was positive for estrogen receptor. Postoperative treatment consisted of chemotherapy and radiotherapy. After this treatment, the patient received 20 mg tamoxifen daily. In 2009, the patient presented with postmenopausal bleeding and lower abdominal pain. On pelvic examination, the uterus was slightly enlarged, and on routine ultrasound, a mass was detected in the uterus. Routine hematological, biochemical, and tumor marker determinations revealed no particular abnormalities. Pathologic examination of a curettage biopsy showed the existence of a MMMT arising from the endometrium (Fig. 1). Total abdominal hysterectomy with bilateral salpingooophorectomy and pelvic lymphadenectomy were carried out. Final pathological examination confirmed MMMT of the endometrium with no lymph node metastasis. Histologically, the tumor was 65 mm in size and had infiltrated more than half the myometrial wall of the uterus. There was no venous or lymphatic invasion. Resection margins were free of tumor. The patient received pelvic radiotherapy after surgery. The patient is currently disease free for breast cancer. She has shown no recurrence of the MMMT for more than 12 months.
Discussion
Tamoxifen, a selective estrogen receptor modulator, is a standard endocrine treatment for hormone receptor-positive breast cancer, both in the adjuvant and metastatic settings. Tamoxifen will continue to be an important drug for the treatment of hormone-dependent breast cancer, despite results suggesting that aromatase inhibitors will play an increasing role in the treatment of breast cancer for postmenopausal women.5,6
The clinician must, however, keep in mind that tamoxifen may have serious side effects. Besides thromboembolic events, endometrial proliferation and subsequent endometrial cancer in particular are well-documented risks in long-term tamoxifen users. We are reporting a case of a postmenopausal, multiparous patient who developed a MMMT within 4 years of tamoxifen exposure for breast cancer. Fortunately, the time of detection was short and the surgical intervention was sufficient for the treatment of the MMMT of the uterus. Interestingly, our patient presented none of the known predisposing factors for uterine neoplasms like hypertension, diabetes, or obesity. She had no history of endometrial polyps or mucosal hyperplasia. The only known risk associated with endometrial cancer in this patient was tamoxifen therapy over a period of 4 years. Curtis et al. 4 provided evidence that the use of tamoxifen is associated with an overall fourfold relative risk for MMMT. This risk rises to eightfold if patients take tamoxifen for more than 5 years.
Tamoxifen may cause cellular changes by altering oncogene and growth factor expressions. Tamoxifen is a potent activator of promoters regulated by AP-1 sites independent of estrogen receptors. AP-1 sites are binding sites for oncogenes c-jun and c-fos, so, tamoxifen is an agonist of AP-1 dependent transcription, which is cell-specific. 7 This is observed in uterine cells but not in breast cells lines. 8 It has been shown that tamoxifen induces expression of c-fos and c-jun protooncogenes in the rat uterus, and overexpression persists for 7 days after administration of tamoxifen. 9 Moreover, tamoxifen has been found to increase immunoreactive TGF-beta in the endometrium and is particularly more pronounced in endometrial stroma. It has been hypothesized that TGF-beta isoforms might be an important mediator of both estrogen and tamoxifen-induced proliferative disorders in the uterus. 10 TGF-beta is mitogenic and angiogenic in the endometrium, 11 and it was found to be strongly expressed in uterine MMT developed after tamoxifen therapy in a case report. 12 In addition, tamoxifen has been shown to exert a direct genotoxic effect by DNA adduct formation. DNA adducts were created by the microsomally activated substance metabolite E of tamoxifen. 13 Overexpression of p53 in tamoxifen-associated endometrial cancers, reflecting the mutant status of the gene, might imply increased exposure to DNA-mutating compounds. 14 These findings indicate that several mechanisms may exist in the association between tamoxifen use and endometrial cancer.
Conclusion
It has been established that the benefits of adjuvant tamoxifen therapy outweigh the increased risk of uterine cancer, but it is important that the clinician and patient be aware that the risk of uterine cancer continues for years after tamoxifen is discontinued. These women may be at an increased risk of a poor outcome years after completion of treatment for breast cancer due to the risk of developing an aggressive uterine malignancy. Routine screening in this population with ultrasound and endometrial sampling has been found to be of limited benefit. However, these patients need to be educated on the importance of reporting symptoms and having regular gynecologic examinations even after cessation of tamoxifen in order to try to detect these cancers at an early stage. 15
Footnotes
Disclosure Statement
No competing financial interests exist.