
Abstract
Abstract
Introduction
Leiomyomata are often asymptomatic, as only a third of the women have symptoms such as menorrhagia, dysmenorrhea, abdominal swelling and mass, pelvic pressure or pain, and infertility. Symptomatic leiomyomata are the primary indications for ∼ 30% of all hysterectomies and for ∼40 % of hysterectomies (or 150,00–200,000 hysterectomies) annually for benign conditions in the United States. At least 34,000 myomectomies are performed annually in the United States. 4 Risk factors include: increasing age; black race; early menarche; low parity or nulliparity; tamoxifen use; obesity; high-fat diet; polycystic ovary syndrome; diabetes; hypertension, and genetic predisposition.5,6 Age and race are the most significant risk factors for fibroids. African-American women have their fibroids diagnosed earlier than their white counterparts, with the highest incidence rate of diagnosis occurring between ages 35 and 40, versus between ages 40 and 44 for whites. 7 The mean age of diagnosis is 37.5±7.9 years for African-American versus 41.6±6.6 years for white women. 8
Case
A 22-year-old black nulligravida with amenorrhea of 6 months' duration, and a history of progressive abdominal enlargement of 9 months' duration, came to the prenatal clinic for an initial prenatal care visit thinking that she was 9 months pregnant. She had received treatment for abdominal pain in the emergency department 2 days prior and a urine pregnancy test was found to be negative. She was asked to follow up with the gynecologic clinic. However, she was not convinced about the negative pregnancy test at the emergency department and came to the obstetric clinic for prenatal care. She was a new visitor in the United States; she had arrived from Haiti 3 weeks prior, where she had lived all of her life, and had also received initial treatment for this condition there. She claimed to have been told by a clinic in Florida 2 weeks prior that she was pregnant, but this information could not be substantiated. She also gave a positive history of associated vague abdominal pain, weight loss, dyspepsia, occasional nausea and vomiting, shortness of breath, and weakness. However, she denied a history of chest pain, orthopnea, leg swelling, paroxysmal nocturnal dyspnea, easy fatigability, genitourinary symptoms, or other gastrointestinal symptoms.
She denied any past medical and surgical history. She had attained menarche at age 14 years, with regular menstrual cycles, with a flow for 3–5 days in a 30-day cycle. She denied a history of menorrhagia, dyspareunia, or dysmenorrhea, or sexually transmitted diseases and she had never had a Papanicolaou smear. She had been married for 18 months and had never been pregnant. She was the last of 5 children (3 females and 2 males). Her family history was significant for ovarian cancer in her grandmother at age 66 and leiomyoma in 2 elder sisters at ages 36 and 39, respectively. The patient denied a family history of diabetes mellitus, hypertension, coronary heart disease, cerebrovascular accidents, or sudden death. She was a housewife and denied abuse of tobacco, alcohol, or illicit drugs. She was taking prenatal vitamins and denied a history of drug allergy.
Her vital signs at presentation were: blood pressure (BP), 129/85 mm Hg; heart rate (HR), 93 beats/minute; RR, 24/minutes, temperature, 98.6oF, and SaO2, 98% on room air. Her preoperative weight was 163 lbs (74.3 kg). She was tachypneic with mild respiratory distress caused by obvious gross distension of her abdomen. Her lung fields were clear bilaterally, with no crackles, wheezing, or rhonchi, and the heart sounds S1 and S2 only were heard and were normal with no murmurs. Her abdomen was grossly distended, tense, and nontender, with abdominal gird at the level of the umbilicus of 139 cm. There were visible superficial inferior epigastric vessels but there were no striae, spider nevi, or caput medusae. There was an ill-defined palpable abdominopelvic mass with a smooth surface that was fixed, firm in consistency, nontender, and extending up to the xiphisternum. There was no demonstrable ascites, and the bowel sounds were distant but with normal frequency. A vaginal examination revealed a normal vulva and vagina, but her cervix was flush with the vagina wall and her uterus was difficult to delineate from the mass.
Imaging studies
The abdomen and pelvic sonogram showed a mass with a >35 cm craniocaudal dimension with irregular septations and irregular soft-tissue components. There was no significant free fluid in the abdomen and pelvis. These results may have represented an ovarian process such as a cystic ovarian neoplasm. A computed tomography scan of the abdomen and pelvis showed a large cystic mass with enhancing prominent lobulated soft-tissue components and a few thin enhancing septae. The mass occupied most of the intra-abdominal space, measuring ∼ 30×20×47 cm. The uterus appeared normal in size and enhancement; therefore, it was more likely that the large mass originated from adnexa. Results from testing were as follows: white blood–cell count, 4830 cells/mL; hemoglobin, 14.1 g/dL; hematocrit, 43.4%; platelet counts, 207, 000 cells/mL; urine pregnancy test, negative; purified protein derivative (PPD), negative; CA-125, 19.2 U/mL (normal: <34 U/mL); α-fetoprotein (AFP), 3.0 μg/L (normal: <10.0 μg/mL); carcinoembryonic antigen (CEA), 0.32 ng/mL (normal: <2.5 ng/mL); human chorionic gonadotropin (hCG), <1.20 mIU/mL; and estradiol; 356 pg/mL (normal: 30 – 400 pg/mL). See Figures 1–4 for imaging, gross picture, and histopathology.

Computed tomography scan of the abdomen and pelvis at the supraumbilical region showing the large intra-abdominal tumor.
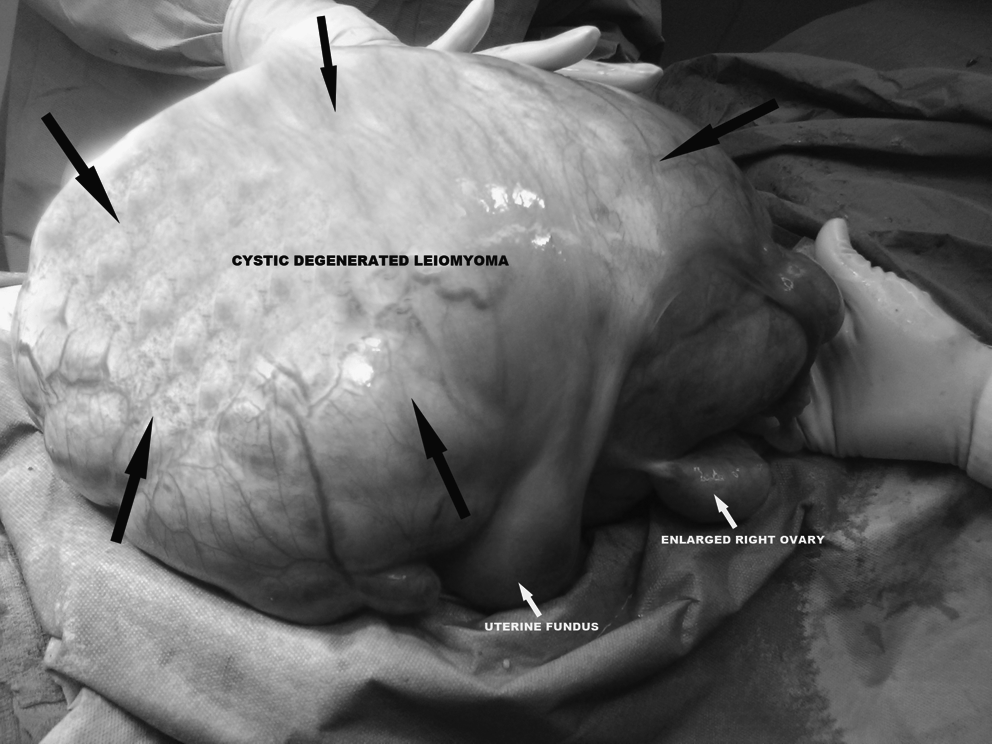
Gross picture of the entire tumor attaching to the uterus, ovaries, and fallopian tubes after exteriorization during surgery.
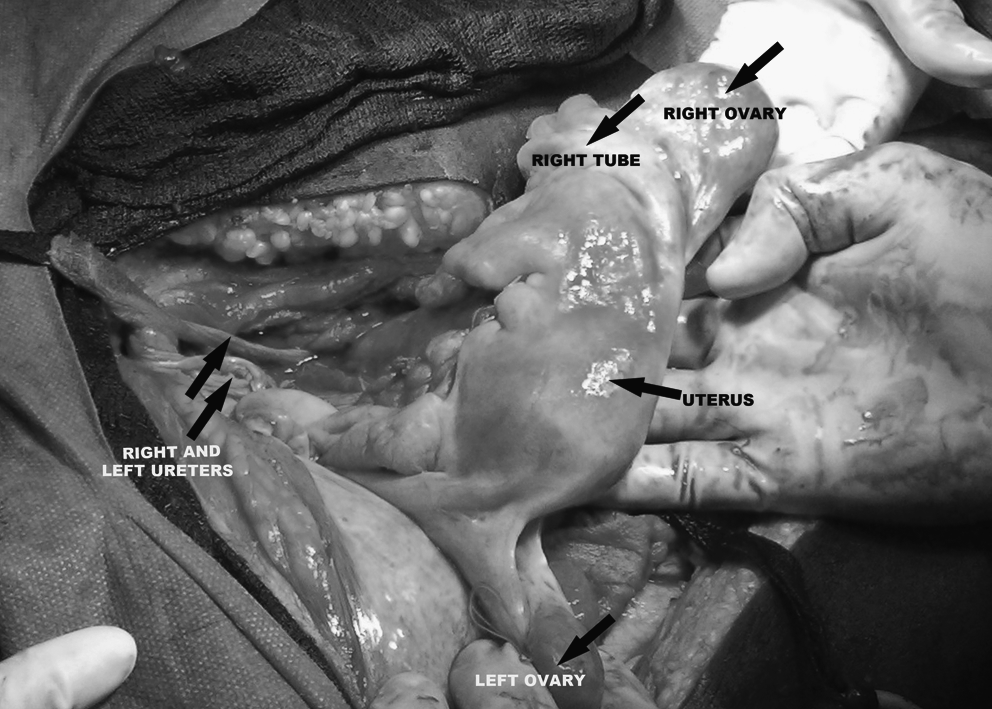
Internal genital organs. The uterus, ovaries, and fallopian tubes, and the ureters and major blood vessels after debulking the tumor.
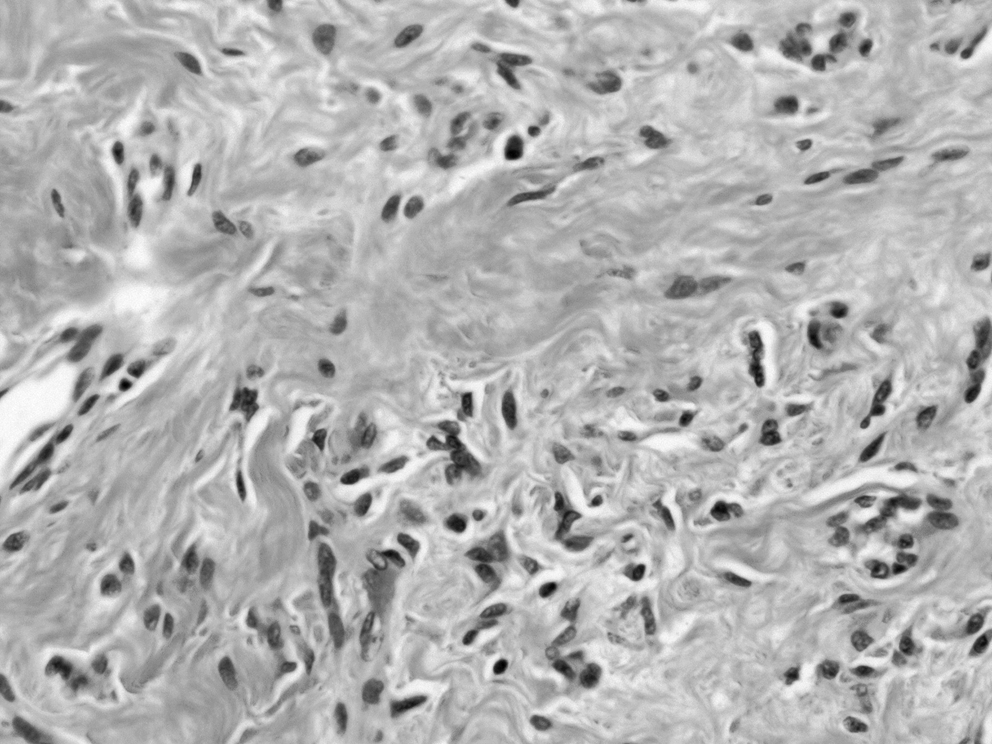
Histopathology of the tumor. It shows bundles of spindle-shaped smooth-muscle cells separated with hyaline and hydropic degeneration. There are no nuclear atypia, abnormal mitosis, or coagulative necrosis.
Diagnosis and treatment
Based on the clinical presentation and imaging studies, a clinical diagnosis of an intra-abdominal and pelvic tumor was made. The patient underwent exploratory laparotomy with a midline vertical incision with supraumbilical extension, and a large tumor arising from the anterior wall of a slightly overstretched enlarge uterus, which was pushed to the left adnexa, was found. The mass had a sessile attachment to the uterus from the isthmus to the fundus and occupied the entire pelvic and abdominal cavities, measuring 67×45×39 cm. There were huge vascular attachments posterior to this mass. Complete assessment and debulking of this tumor was difficult. Hence, a small purse-string suture was made on the anterior portion of the mass and a stab wound was made within the purse-string to allow a pull-suction tube to be passed without spillage of its content. Eleven liters of serous fluid was drained before extensive dissections were done to remove the mass that had attachments to the hepatic capsule, stomach, spleen, transverse colon, small bowels, sigmoid colon, and anterior and posterior uterine walls. The uterus, the fallopian tubes, and the ovaries were dissected off from the mass and were preserved.
Results
Excellent hemostasis was obtained and estimated blood loss was 1100 mL. No intraoperative blood transfusion was given, but the patient was transfused with 2 U of packed red blood cells immediately postoperatively. The rest of the postoperative course was unremarkable, and the patient was discharged on the fourth postoperative day. She was subsequently seen in the gynecologic clinic for follow-up three times with no significant abnormalities found. Her postoperative weight was 127 lbs (57.6 kg), with a differential weight change of 36 lbs (16.3 kg) immediately after the surgery.
Discussion
MEDLINE® and PubMed databases were searched from January 1, 1990 to December 31, 2009, crossreferencing the index terms
TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; SCH: supracervical hysterectomy.
Uterine leiomyomata are believed to originate from multiple chromosomal abnormalities. Individual myomata are monoclonal in origin, as they develop from a single progenitor myocyte with the same chromosomal abnormality. The size of the myoma is proportional to the degree of karyotype abnormalities. 28 The chromosomal abnormalities are: translocation between chromosome 12 and 14 in 20% of cases; deletion of chromosome 7 in 17%; and deletion of chromosome 12 in 12 %. The region affected in chromosome 12 and 7 involves a gene that regulates growth-inducing proteins and cytokines, such as transforming growth factor–β (TGF-β), epidermal growth factor (EGF), insulinlike growth factors (IGFs)–1 and −2), and platelet-derived growth factor (PDGF). The key regulators of fibroid growth are ovarian steroids, estrogen and progesterone, growth factors and angiogenesis, and the process of apoptosis. 6 Moreover, a gene that predisposes patients to multiple fibroids, cutaneous leiomyomata, and papillary renal-cell carcinoma has been linked to chromosome 1q42.3 – q43 in some studies.5–7 This gene codes for fumarate hydratase (FH), a mitochondrial enzyme of the tricarboxylic acid cycle. The enzyme acts as a tumor-suppressor gene; a deficiency of this enzyme has been linked to a specific hereditary fibroid-associated syndrome, and tumors begin to form when a woman is between ages 20 and 35. 29
As the myomata enlarge, they may outgrow their blood supply, resulting in various types of degeneration. These degenerative changes are atrophic, hyaline, fatty, cystic, myxoid, red (hemorrhagic infarction), or necrobiotic and calcareous (dystrophic calcifications). 30 Hyaline degeneration is the most common type of degeneration, occurring in up to 60% of cases, and edema is found in ∼ 50% of cases on histopathology. Cystic degeneration is observed in ∼ 4 % of leiomyomata, and may be considered as an extreme sequela of edema. 30 The majority of fibroids with cystic degeneration are pseudocysts derived from liquefaction of hyaline changes. True cysts do exist among fibroids, and these are referred to as lymphangiectasis. Other secondary changes in fibroids include circulatory changes, such as edema and lymphangiectasis, axial rotation leading to congestion, interstitial hemorrhage, necrosis, and detachment. Angiomatous or telangiectatic changes, infective changes leading to inflammation, suppuration (localized abscess), gangrene, and sloughing may occur. Malignant changes include sarcoma (malignant leiomyoma), perithelioma, and endothelioma.
The presence of a large cystic degeneration of leiomyoma may pose a serious diagnostic dilemma and management challenges, especially when it occurs in a young nulliparous patient. The mean age of the reviewed cases of cystic degenerated leiomyoma in this article was 43, and the age range was from 16 to 56. Approximately 58% of the cases were subserous or pedunculated fibroids, and 26% presented with abdominal pain. Approximately 58% were of the multilocular type, and 52% contained serous fluid. Hysterectomy was the mode of treatment in 84% of cases, whereas only 16% had fertility-preserving surgeries.
The most common symptoms of fibroids are heavy menstrual bleeding or prolonged menstrual periods, and a feeling of pelvic pressure. The patient reported in this article had an unusual presentation of amenorrhea and progressive abdominal swelling, which, in a young reproductive-age woman, could be interpreted as pregnancy. It is not surprpising that this patient presented to the Kings County Hospital Center, New York, NY, to seek prenatal care for a presumed 9-month pregnancy. This case presented the largest cystic degenerated leiomyoma reported in the literature to date. Moreover, its occurrence in a young nulliparous patient and its rapid growth posed a serious diagnostic and great surgical dilemma. A successful fertility-preservating surgical procedure and excellent postoperative recovery made it intriguing. This diagnostically and surgically challenging treatment was successful because of the combination of good preoperative preparation, meticulous surgical skill, and intensive postoperative care. The management approach was largely influenced by the patient's age and parity, and the size and extent of the tumor.
Conclusions
Cystic degenerated fibroids represent benign changes in leiomyomata, and they can manifest with varying symptoms depending upon their sizes and locations. Most cystic degenerations are secondary to liquefaction of hyaline degeneration. However, some cystic leiomyomata appear to arise de novo as cysts, which may suggest another pathophysiology of cystic degeneration. The treatment approach is largely influenced by age, parity, desire for future fertility, the presenting symptoms, and the extent of the tumor. The case presented here was a young nulligravida who desired future childbearing. She underwent uncomplicated myomectomy and excision of pelvic mass.
Footnotes
Disclosure Statement
No competing financial conflicts exist.