
Abstract
Abstract
Introduction
Case Reports
Case 1
A 25-year-old woman, gravida 2, abortus 1, who had had amenorrhea for 7 weeks presented with complaints of lower abdominal pain, nausea, dizziness, and difficulty in passing urine of 1 day's duration. She had no history of bleeding per vaginum. She had been married for 3 years. Eight months previously, the patient had had one spontaneous first trimester abortion. She had regular menses and was not using any contraceptive methods. There were no risk factors for extrauterine pregnancy in her gynecologic history.
On physical examination, the patient was pale with a pulse rate of 120/min and blood pressure of 90/60 mm Hg. On abdominal examination, soft distention was present with tenderness in the lower abdomen. On vaginal examination, cervical motion tenderness was present and a tender mass of 4×4 cm was palpated in the right adnexa. Beta human chorionic gonadotropin (β-hCG) level was 17,650 international units (IU)/L. Culdocentesis was positive. Laparotomy was performed immediately through a transverse abdominal incision, and revealed intraperitoneal hemorrhage of ∼1000 mL. Two units of blood were transfused. The right tube appeared normal but the right ovary showed a gestational sac with hemorrhage. The left tube and ovary were normal. Wedge resection of the right ovary was performed. The tissue extracted was suspected to be either ovarian ectopic pregnancy or hemorrhagic corpus luteum. Histopathology examination confirmed the diagnosis of ovarian ectopic pregnancy.
Case 2
A 30-year-old patient, gravida 4 para 0, abortus 3, who had had amenorrhea for 53 days was admitted with complaints of lower abdominal pain of 2 days' duration, and one episode of vomiting. She had been married for 13 years. She was sexually active and using no form of contraception. She had previously had three pregnancy losses and two laparotomies. The first laparotomy had been performed by a private practitioner 7 years earlier and perioperative findings had been suggestive of a left tubal abortion. The second laparotomy had been performed 2 years earlier for ectopic pregnancy, and a left-sided salpingectomy was performed. In between the two laparotomies patient had one spontaneous abortion. There was no history of ovulation induction or assisted reproductive technologis (ART).
On examination, the patient was pale with pulse rate of 100/min and blood pressure of 100/60 mm Hg. Her lower abdomen was tender. Vaginal examination revealed tenderness and fullness in the pouch of Douglas. Ultrasonography revealed an empty uterus with thickened endometrium and a hyperechoic lesion of 3×4 cm was seen in the right ovary caused by hemorrhage in the ovarian ectopic pregnancy. Free fluid in the cul-de-sac with internal echoes was seen, and the left ovary was normal. β-hCG) level was 14,690 IU/L. Culdocentesis was positive. The laparotomy was performed in view of a clinical diagnosis of ectopic pregnancy. On laparotomy, 500 cc. of hemoperitoneum was present in peritoneal cavity. The right tube was normal. A mass of 4×3 cm was present in the right ovary with a breach in continuity of the tunica albugenia. The mass was resected with some ovarian tissue, and the ovary was reconstructed. The left ovary was normal. Histopathologic examination confirmed the diagnosis of ovarian pregnancy (Fig. 1). The postoperative period was uneventful.
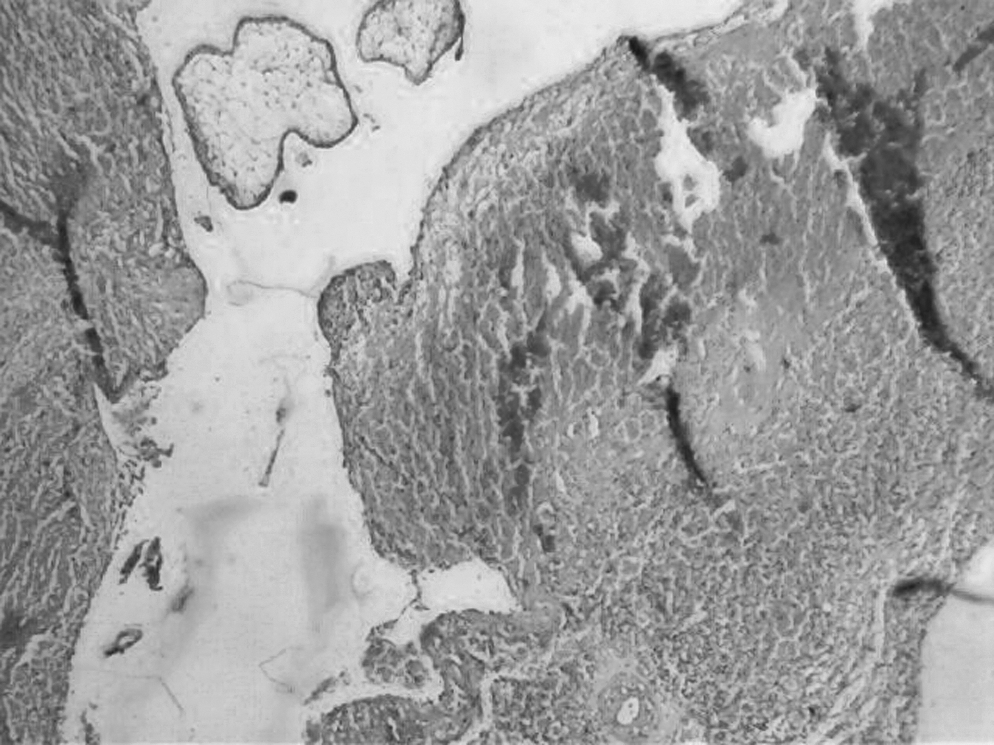
Villi and hemorrhagic stroma.
Results
The first patient has had regular follow-up for a year and, as of this writing was carrying an 8-week intrauterine pregnancy. The second patient was lost to follow-up.
Discussion
Primary ovarian pregnancy is a rare form of ectopic pregnancy that must be demonstrated with Spiegelberg criteria, which are: the fallopian tube, including the fimbria ovarica, is intact and clearly separate from the ovary; the gestational sac definitely occupies the normal position of the ovary; the sac is connected to the uterus by the utero-ovarian ligament; and the ovarian tissue is unquestionably demonstrated in the wall of the sac. Unfortunately, these are the surgical criteria; none of these criteria can be established on ultrasonography. All these criteria were fulfilled in the cases reported here. Differential diagnosis include ruptured hemorrhagic corpus leuteum, chocolate cyst, and ruptured tubal ectopic pregnancy.2,3
In contrast with patients with tubal pregnancies, traditional risk factors such as pelvic inflammatory disease and prior pelvic surgery may not play a significant role in the etiology of primary ovarian pregnancy; ovarian pregnancy is more frequent in ectopic pregnancies associated with the use of contraceptive intrauterine devices.4,5 Neither of our patients, however, was using an intrauterine device. Other hypotheses have suggested interference in the release of ovum from the ruptured follicle, malfunction of tubes, or inflammatory thickening of tunica albugenia. 4 Ovarian hyperstimulation and ART are the other reported etiologies. Borrow concluded that chance is the reasonable explanation for ovarian pregnancy. 3
Primary ovarian ectopic pregnancy in case 1 was probably a random and chance occurrence, but case 2 had had two previous laparotomies for ectopic pregnancy, suggesting inflammatory disease. The signs and symptoms of ovarian pregnancy are similar to those of disturbed tubal gestation.
With the improvement in ultrasonographic skills, and especially with the vaginal probe, ovarian pregnancy has been diagnosed preoperatively.6,7 No case of repeat ovarian pregnancy has been reported in contrast to the ∼15% recurrent tubal pregnancy rate, and 1 case of tubal pregnancy after a previous ovarian pregnancy has been documented. Rupture in first trimester is the usual rule in ovarian ectopic pregnancy, but this pregnancy may occasionally advance to full term. 6 In delaying the diagnosis there is risk of rupture, secondary implantation, and difficulties during surgery. Only a few case reports describe medical management of ovarian pregnancy, using either methotrexate or mifepristone (RU 486) in combination with prostaglandin F2α.8–10 Because it is not possible to diagnose an ovarian pregnancy without performing at least a laparoscopy with collection of a biopsy, it is correct to conclude “If laparoscopy is required for diagnosis, definitive surgical management may be accomplished at the same time.” 9
In the past, ovarian pregnancy had been treated by ipsilateral oophorectomy, but the trend has since shifted toward conservative surgery such as cystectomy or wedge resection performed at either laparotomy or laparoscopy. 11
Conclusions
Awareness of the possibility of ovarian pregnancy and histologic examination of surgical specimen are key factors for diagnosis of ovarian pregnancy.
Footnotes
Disclosure Statement
No competing financial conflicts exist.