
Abstract
Abstract
Introduction
In addition to the potential for anatomic failure, the surgical correction of POP can precipitate stress urinary incontinence (SUI) in previously continent women as a result of “unkinking” of the urethra and/or overelevation of the bladder base. The ideal method for repair of POP and addressing cases of recognized and “occult” incontinence is a subject of debate. Abdominal sacrocolpopexy (ASCP) has been considered the “gold standard” surgical procedure for repair of level I pelvic support defects. The Colpopexy and Urinary Reduction Efforts (CARE) trial demonstrated that a prophylactic Burch procedure reduced occult SUI rates from 44.1% to 23.8%, therefore indicating that an anti-incontinence procedure should be performed in women undergoing ASCP regardless of preoperative urodynamic testing results. 4 The 2-year follow-up data of the CARE trial showed a slightly lesser impact, with a 32% rate of SUI in the Burch group versus a 45.2% rate in the non-Burch group (p=0.026). 5 More recently, Elser et al. 6 reported ASCP with concomitant incontinence procedure (Burch or midurethral sling) based on urodynamic evidence of SUI (USI) during prolapse reduction. At a mean follow-up of 46.6 weeks, the overall rate of incontinence was low, and similar between groups (13.4% versus 13.3%). These authors concluded that urodynamic evaluation was useful in determining the need for incontinence surgery at the time of ASCP and, based on significantly lower rates of SUI in the midurethral sling versus the Burch group, slings may be superior in preventing postoperative SUI in patients undergoing ASCP.
Robotic sacrocolpopexy (RSCP) has become an appealing alternative to ASCP because of its association with less blood loss and a shorter hospital stay. 7 To date, there are no published data on rates of persistent and de novo SUI in women undergoing RSCP. Because there is a lack of haptic feedback with robotics, there is potential for overcorrection of the vaginal apex when assessing the tension of the mesh, with loss of a normal posterior urethrovesical angle.
The primary aim of this study, therefore, was to compare the rates of postoperative SUI in women undergoing RSCP with and without a concomitant midurethral sling. when the decision to perform an incontinence procedure was based on the presence of USI or positive results of a cough-stress test. In addition, the study was designed to compare the prevalence of overactive bladder (OAB) symptoms in each group.
Materials and Methods
Institutional review board approval was obtained at the University of North Carolina at Chapel Hill (UNC) and at Virginia Commonwealth University Medical Center (VCU). A retrospective chart review of all women who underwent RSCP between November 2007 and January 2010 at both institutions was performed. The following preoperative data were collected: age; parity; race; body mass index (BMI); stage of POP (graded by Pelvic Organ Prolapse Quantification system [POP-Q]); maximum urethral closure pressure (MUCP); presence or absence of stress incontinence during urodynamic investigation; any urge symptoms; and presence or absence of detrusor overactivity (DO). All subjects completed a series of validated questionnaires including the Urinary Distress Inventory Short-form (UDI-6) subscale of the Pelvic Floor Distress Inventory Short-form (PFDI-20) at baseline and 3 or 6 months postoperatively. SUI was defined as a response of “Yes” to question 3 on the UDI-6: “Do you usually experience urine leakage related to coughing, sneezing, or laughing.” Severe SUI was defined as a response of “moderately” or “quite a bit” bothersome to question 3. Urinary frequency was defined as an answer of “Yes” to question 1: “Do you usually experience frequent urination.” Urge urinary incontinence was defined as an answer of “Yes” to question 2: “Do you usually experience urine leakage associated with a feeling of urgency.” OAB symptoms were defined as an answer of “Yes” to either question 1 or question 2.
Statistical analysis
For statistical analysis, the subjects were divided into two groups: those who underwent an RSCP with concomitant midurethral sling placement (Group 1) and those who underwent an RSCP only (Group 2). The primary outcome was the rate of persistent and de novo SUI at 3–6 months postoperatively, as measured by the UDI-6. Secondary outcomes included an assessment of SUI severity between the two groups and the prevalence of OAB symptoms (urinary urgency, frequency, and urge leakage). Statistical analyses were performed with SPSS, version 16.0 (Chicago, IL.) including Pearson's χ2 and Fisher's exact test for categorical data, Student's t-test for continuous data, and Mann–Whitney U test for ordinal data. Relative risk (RR) ratios and confidence intervals (CIs) were determined.
Results
Preoperative data were available for 82 subjects: 49 from UNC and 33 from VCU. Baseline demographics were similar between groups (Table 1). The majority of subjects had stage III apical prolapse prior to surgery. Group 1 included 43 subjects who underwent RSCP with sling and Group 2 included 39 subjects who underwent RSCP alone. In Group 1, 76% of the women had documented preoperative USI. The remainder of the patients had documented SUI based on a positive supine cough stress test or a positive pyridium pad test. When comparing urodynamic parameters between those who had USI and those who did not, there was no difference in preoperative MUCP (59.8 versus 53.7 cm of water, p=0.368). Irritative voiding symptoms were similar in both groups. Overall, at baseline, 56% of subjects reported preoperative urinary urgency and 11% of subjects were found to have preoperative detrusor overactivity by urodynamics. There was no difference between the two groups.
Data=mean±standard deviation, n (%) or median (25–75th percentile).
Student's t-test.
Mann-Whitney U test.
Pearson's chi-square test.
Fisher's exact test.
RSCP, robotic sacrocolpopexy; BMI, body mass index.
The overall rate of postoperative SUI was 31.7%. A concomitant sling was placed in 30.8% of these subjects. Of the slings placed, there were 34 retropubic slings (79%) and 9 transobturator slings (21%). For the primary outcome, it was found that the rate of postoperative SUI was lower in women who underwent RSCP with concomitant sling placement, compared with those who underwent RSCP alone. Women who underwent sling placement were 60% less likely to have postoperative SUI, compared with those who did not receive a concomitant sling (RR 0.4, 95% CI 0.2–0.8) (Fig. 1).
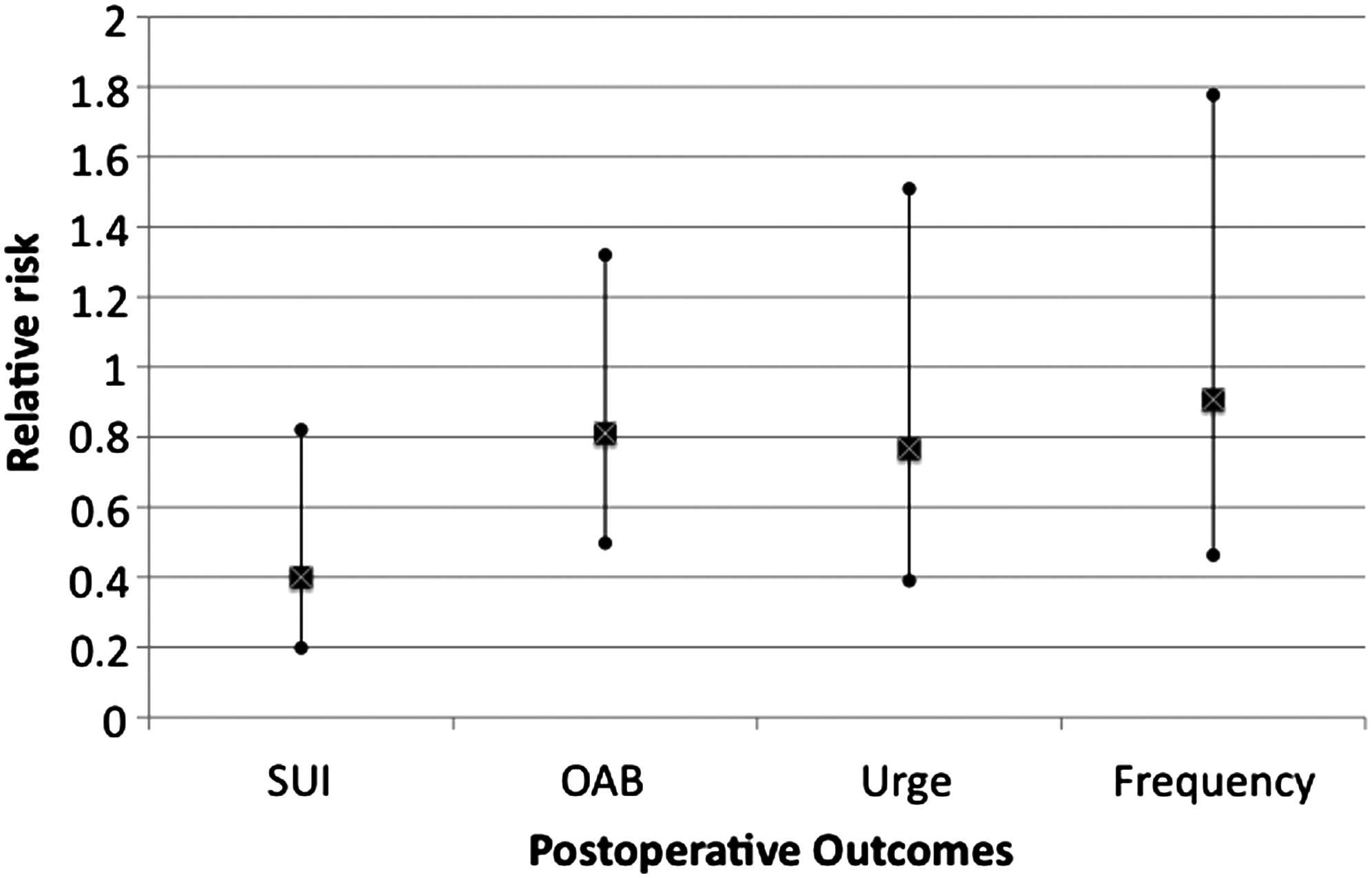
The relative risk and 95% confidence interval for primary and secondary outcomes.
There were 2 patients in Group 2 who had USI but did not receive a sling: 1 had a urethral injury at the time of sling attempt and the other elected to not have a sling. Of those women reporting any postoperative SUI, 26.9% reported it to be “severe.” Severe SUI was significantly more common in the group that did not have a concomitant sling (15.8% versus 2.4%, p=0.049). The number of slings needed to prevent case of postoperative SUI was 3.6. Among women with postoperative SUI (18.6%), there was no difference based on type of sling—retropubic 6/8 (75%) versus transobturator 2/8 (25%; p=0.99).
In terms of irritating voiding symptoms, there were no differences between the two groups in postoperative urinary frequency, urge urinary incontinence, or OAB symptoms (Table 2). Preoperative OAB symptoms were not predictive of persistent or de novo postoperative OAB symptoms (42.2% versus 45.5%, p=0.776).
Data=n (%).
Pearson's chi-square test.
Fisher's exact test.
RSCP, robotic sacrocolpopexy; OAB, overactive bladder.
Discussion
In women undergoing RSCP, there was a high rate of postoperative de novo SUI that urodynamic studies were not able to accurately predict. Urodynamic testing has conventionally been used to assist in directing the need for an incontinence procedure at the time of surgical correction of advanced POP. The potential benefit of these investigations is a reduction in unnecessary anti-incontinence procedures that may cause additional surgical morbidity, increase cost, and increase the chance of postoperative irritating voiding symptoms. In this study, in which the decision to perform an incontinence procedure was predominantly made on the basis of evidence of urodynamic stress incontinence, the cure rate was 81% for those who had a concomitant sling placed. In those women without evidence of USI, however, almost half reported the new onset of SUI 3–6 months after undergoing RSCP. In addition, those with de novo SUI after RSCP alone had more severe SUI, compared to those with persistent SUI after a concomitant sling placement.
The current authors' reported rate of de novo SUI (46.2%) is similar to the CARE trial data 4 (44.1%) but higher than rates reported in retrospective cohort studies by Elser et al. 6 (13.3%) and Misrai et al. 8 (13%) who reported on ASCP and laparoscopic sacral colpopexy, respectively.4,6,8 This variability may be related to measurement techniques. The current authors used a strict definition as a response of “yes” to any episode of postoperative SUI on the UDI-6. In this study, the 15.8% rate of severe SUI is similar to that of Elser et al. 6 (13.3%) and Misrai et al. 8 (13%) when the use of nonvalidated questionnaires may have captured only the more significant cases.
The potential for de novo SUI in women undergoing RSCP is real. While operating remotely at the surgical console, it is difficult to assess tension of the mesh on the vaginal apex and the degree of correction of the anterior vaginal wall. The surgeon could either leave the console to evaluate the vaginal anatomy or have a bedside assistant perform the assessment. The current authors' estimate of the tension placed on the mesh is based on the visual appearance of “adequate” support by the console surgeon and the bedside assistant who can perform a vaginal examination. Based on the observed rate of de novo SUI in women undergoing robotic surgery in this study, it seems clear that regardless of urodynamic results, the risk of postoperative SUI is high. These findings corroborate the conclusions of others that preoperative USI with prolapse reduction does not predict postoperative SUI accurately. 9
In this study, it was determined that placement of 3.6 slings would be necessary to prevent 1 case of postoperative SUI in women undergoing RSCP. These findings support the argument that a prophylactic sling probably prevents a higher rate of SUI as well as more severe postoperative SUI. This information is useful for clinicians in directing preoperative counseling.
The principal limitations of this study are the retrospective design, its relatively small sample size, and the lack of a more objective measure for SUI postoperatively, such as a standing stress test. Selection and reporting bias, inherently present in retrospective reviews, may have affected the observed rates of SUI. However, the use of a standardized questionnaire that was collected prospectively may help decrease any reporting bias. In addition, the current authors' protocol for placement of a concomitant sling to address incontinence in the presence of any USI was not strictly adhered to. Several women declined sling placement, based on mild symptoms, whereas others accepted sling placement, based on a confirmatory test. Using these less-strict criteria, it is possible that the predictability of preoperative urodynamics was underestimated. The strengths of the study include the use of validated questionnaires that were collected prospectively, the use of a strict definition of SUI, and the inclusion of two study sites, which could improve the generalizability of the results.
Conclusions
Women undergoing RSCP have a high rate of postoperative SUI. The rate and severity of this SUI is decreased when a concomitant midurethral sling is used. Based on findings of this study and the observed inability to predict de novo SUI on urodynamic testing, it is recommended that surgeons consider placement of a concomitant sling at the time of robotic prolapse reconstruction.
Footnotes
Disclosure Statement
Catherine Matthews, MD, is a consultant for Intuitive Surgical and American Medical Systems. The other 3 authors have no competing financial interests.