
Abstract
Abstract
Introduction
Case
A 27-year-old woman P1A1 presented to our outpatient department with complaints of abdomen pain for the previous 9 months. She had a history of two laparotomies for ovarian cysts in past 5 years, the details of which were not available. Her general physical examination was unremarkable. On abdominal examination, a mass of about 12 cm×8 cm size was found in the right iliac region. The mass was cystic in consistency, non-tender, and had restricted mobility. The lower margin of the mass was palpable. Her routine laboratory investigations were within normal limits. Sonography done at another hospital showed a multiseptate lesion 11.5×8 cm in size with some solid component in the right adnexa, giving the impression of an ovarian tumor. There was no such cyst in the spleen, liver, or any other abdominal organ. Her CA125 level was 5.8 mIU/mL. However, a repeat sonography at our tertiary center revealed well-defined fluid collection in a honeycomb pattern with multiple septa representing walls of daughter cysts (cysts within cyst) with hyperechogenic internal echo pattern and posterior acoustic enhancement (hydatid sand) pathognomonic of hydatid cyst. A computed tomography (CT) scan revealed a demarcated multiloculated low-density mass of fluid attenuation with high attenuation wall at unenhanced CT. Daughter vesicles appeared as round structures located peripherally within the mother cyst (Fig 1). The patient was taken up for laparotomy. In surgery, there was a large 15×10 cm retroperitoneal cystic mass with multiple small daughter cysts lateral to the right psoas muscle, which was enucleated. Dissection was meticulous to keep the mass intact and to avoid spillage. The patient's recovery was uneventful, and she was discharged from hospital and advised to take 400 mg albendazole daily for 3 months. The patient was followed up regularly, and, to date, there has been no recurrence.
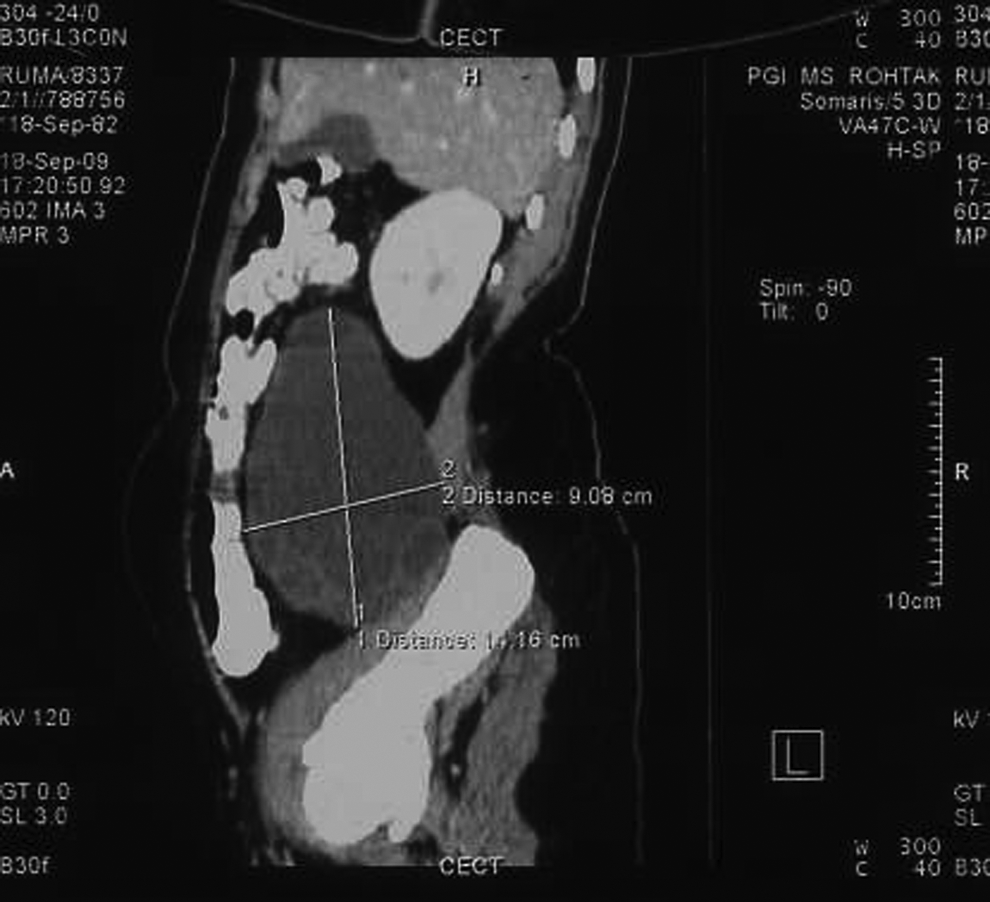
Computed tomography film showing an hydatid cyst.
Discussion
The majority of cases of hydatid disease come from rural areas. Months or years may pass before an individual exhibits any signs or symptoms of infection from the cystic larval stages.
The natural progression of an untreated cyst may include calcification and death of the cyst. However, more frequently, the cyst gradually enlarges. Cystic ecchinococcosis is rarely fatal. Occasionally, deaths occur because of anaphylactic shock or cardiac tamponade in the case of heart echinococcosis.
Although the liver (75%) is the most common site of involvement, followed by the lungs (15%), no site in the body is completely immune from the disease, and hydatid disease should therefore be considered in the differential diagnosis of cystic masses. 2 The atypical and rare presentation of this disease may be seen in the kidneys (3%), spleen (4%), cerebrum (2%), and heart (0.02%), most commonly in the left chamber. 3 Rare sites of cysts (muscles, bare brain, orbit) can cause dramatic and disabling symptoms (blindness and paralysis). A retroperitoneal hydatid cyst is very rare. Most cases are the result of traumatic or surgical ruptures of a hepatic, splenic, mesentric cyst or any other abdominal hydatid cyst. Our case is unique in that the retroperitoneal cyst was primary, since no cyst was found in any other organ. At the same time, the history of previous two laparotomies for ovarian cysts is important. It appears that either no procedure had been done, as both the ovaries were found to be normal on laparotomy, or surgery performed was incomplete.
Hydatid cysts may be solitary or multiple. Most patients (as many as 80%) have single organ involvement and harbor a solitary cyst. Ultrasonography is the first-line screening for abdominal hydatosis, and it is especially useful for the detection of cystic membrane, septae. and hydatid sand. A CT scan best demonstrates cyst wall clacification, cyst infection, and peritoneal seedlings. A typical honeycomb pattern may be seen in multivesicular cysts. The septae represent the walls of the daughter cysts housed within the mother cyst. A “wheel-spoke” pattern can be observed when the daughter cysts are separated by hydatid matrix. 4
Various serological tests like immunoelectrophoresis, enzyme-linked immunosorbent essay (ELISA), and the latex agglutination sand indirect hemagglutination (IHA) test can be carried out for diagnosis, screening, and follow-up of patients with hydatid disease. The diagnosis is easier if the lesion has multiple locations involving different organs or when daughter cysts, germinal membrane detachment, and calcification are present. The World Health Organization has outlined the treatment guidelines for hydatid cysts. 5 Surgery is the mainstay of treatment for large symptomatic cysts. The goals of surgery are to remove the cyst and prevent spillage. If peritoneal spillage occurs during surgery, antihelminthic drugs should be administered. The other alternatives are chemotherapy with albendazole or mebendazole and PAIR therapy (puncture, aspiration, injection, and reaspiration). Indications are (1) large multiple cysts of the liver, spleen, kidney, and bones; (2) inoperable cysts; and (3) relapse after surgery.
Conclusions
In conclusion, the possibility of an hydatid cyst should always be kept in mind when a septated mass is found in the pelvis, and should be treated appropriately.
Footnotes
Disclosure Statement
No competing financial interests exist.