
Abstract
Abstract
Introduction
The women's fear of having a malignant disease and their shame concerning the communication of menstrual problems and pain, as well as the hormonal suppression of possibly symptomatic endometriosis by oral contraceptive pill use, lead to a significant diagnostic delay. 1
There is a significant delay of 7 to 12 years (Brazil/Norway 7 years, United Kingdom 8 years, Australia 9 years, and United States 12 years) from the first occurrence of symptoms to the final diagnosis.1,6–10 Apart from relief of symptoms through successful treatment, the final diagnosis has striking psychologic benefits. These benefits include that the patient receives the confirmation that she has pain caused by physical disease, thereby excluding somatization disorders. In addition to this, women often obtain much more social support after being diagnosed with endometriosis.1,9,11
As mentioned previously, endometriosis not only creates physical symptoms, but it also causes mental disorders such as depression, anxiety, or social dysfunction. 12 The study from Lorençatto et al. using the Beck Depression Inventory (BDI), 13 illustrates that 86% of women having endometriosis and chronic pain and 38% of women having endometriosis without pain, suffer from depression. This indicates that there is a significant connection between pain and affective disorders. 14
Endometriosis-associated discomforts can not only threaten the patient's life but also diminish the patient's QoL. When medical treatment is ineffective, distress and anxiety may result, and a further increase in psychologic discomfort can be observed. Over time, women react with negative emotions such as hopelessness, resignation, depressive symptoms, and/or social isolation as a consequence of the disease. The adverse conditions caused by prevailing pelvic pain have an impact on these young women's education and set limitations to their productivity.
Because of the foregoing, it is not unusual for women with endometriosis not to pursue their desired profession, because of their discomfort; also, patients are pressured and suffer guilty feelings, based on their frequent absence from work (average 17.8 days/year).15,16 The actual Global Study of Women's Health (GSWH) by Nnoaham et al. shows that women with endometriosis have a significantly lower productivity of 38% (11 hours/week) compared with women without this disease. 17 The reasons for diminished efficiency are not just the intensely felt pain that the patients suffer. This diminished efficiency can also be caused by an adverse reaction to analgesic medication. Furthermore, a negative body image was observed in these patients, which increases in cases of an infertility or hysterectomy. Accordingly, feelings of loss of control over one's own body, loneliness, and mental overload resulting from a (failed) medical treatment, have a negative effect on these women's self-esteem. 15
Beyond factors that have already been mentioned, endometriosis-associated complaints often lead to problems with partners or social contacts. Various reasons for that are lack of coping stategies, lack of support/understanding from the surrounding milieu, or avoidance of sexual intercourse. Infertile women in particular have feelings of guilt toward their partners and believe themselves to be unsuitable for them.15,16,18,19
Deep infiltrating (peritoneal invasion of >5 mm) bowel endometriosis (DIE) is less common than peritoneal/ovarian endometriosis. The estimated occurrence is between 5 and 12%; the major locations are the rectum and the rectosigmoid junction, and can extend up to 93% of all intestinal endometriotic lesions.20–23 Despite other endometriosis-associated symptoms, typical complaints are bowel dysfunctions dependent on menstruation, constipation/diarrhea, flatulence, passage of mucus in the stool, pain during bowel movements, and rectal pressure. 24
Indications of colorectal resection for endometriosis are controversial, given the risk of substantial complications. 21 In the past, several studies tried to evaluate the effectiveness of a surgical treatment in cases of DIE on QoL and physical symptoms. Garry et al., 25 for example, showed via pre- and a 4-month postoperative comparison, that after a radical laparoscopic resection of DIE, QoL (measured by EuroQOL/EQ-5D™) 26 and sexual activity (measured by the sexual activity questionnaire) 27 improved significantly. Symptoms such as dysmenorrhea, dyspareunia, and rectal pain decreased significantly and were reduced to normal frequency. However, the effects of the surgical treatment did not have as much influence on improving the psychologic well-being of patients to a level considered normal in the United States female population. 25 Abbot et al. demonstrated the effectiveness of laparoscopic resection in a 2–5 year follow-up research study: Pain scores improved, and sexual activity (habit, pleasure, discomfort) and QoL increased significantly; QoL seemed to have improved postoperatively during this 5-year follow-up period, athough it did not reach a level considered “normal” in the general population. 28
Long-term data on the effects of endometriosis on psychologic well-being are rare, therefore the results of this study are of particular importance. The aim of the present study is to evaluate the change in psychologic well-being and QoL after a laparoscopic radical resection of bowel endometriosis.
Materials and Methods
Patient data
The survey was designed as a retrospective study of women with DIE who underwent radical resection of DIE with segmental resection of the rectosigmoidal bowel at the General Hospital of Villach between October 2004 and October 2008. Diagnosis of endometriosis was based on visualization and radical resection of all tissues exhibiting endometriotic involvement, followed by histologic confirmation defined as the presence of ectopic endometrial tissue, that is, glandular and stromal structures and/or the presence of muscular hyperplasia (in 48 out of 75 cases), and fibrosis on light microscopy.29,30 Infiltration of the rectosigmoid was confirmed by histology in all women included in the present analysis. The study was approved by the local institutional review board. Women either self-referred to the clinic or were referred by general practitioners/ gynecologic consultants. Patients who had a diagnosis of a psychologic disorder such as depression, schizophrenia, borderline disorder, or phobia were excluded from the study as were patients with histories of cancer. Women receiving pre- and or postoperative hormonal treatment were also excluded. Within the study population, surgery was performed either to reduce symptoms associated with DIE such as dysmenorrhea, dyspareunia, and chronic pelvic pain, or because of a history of primary infertility.
Women with confirmed bowel endometriosis were invited to answer a telephone survey. A 10-item questionnaire with a 4-point Likert scale (from 0=strongly disagree to 3=strongly agree) was presented. The measuring tool was developed on the basis of standardized questionnaires such as the SF-36 Health Status 31 for physical and mental health. It evaluated the following scales pre- and postoperatively: feelings of physical exhaustion and lack of motivation, personal satisfaction, lack of acceptance of the own body, the sensation of a depressed mood, loss of body control, general anxiety, lack of understanding, loss of life- motivation, feelings concerning female identity, and, finally, QoL. In addition to the psychologic questionnaire data were also requested about sociodemographic criteria; gynecologic, obstetric, and medical history; and surgical outcome.
Statistical analysis
Because of the asymmetrical distribution of the data, a nonparametric procedure, the Wilcoxon matched pairs signed ranks test, was used for comparison of two (pre/post) dependent groups.
All data were calculated with the Statistical Package for the Social Science (SPSS) 15. The level of significance was set at p<0.05.
Results
Demographics
The average age of the patients at the time of surgery was 34 years (range 23–47). Fifty-five percent of the women were married, 29% were single, and 16% were divorced. Thirty-two percent made use of the psychologic counselling offered at the hospital. The counsellors were two psychologists with specific knowledge of the clinical and psychologic impact of endometriosis. Eight percent had psychologic counselling at a private practice and 12% attended an endometriosis support group.
The median time between surgery and the survey was 38 months (range 13–69).
Previous therapy and surgical findings
At the point of laparoscopic resection, 80% of the patients had undergone previous surgeries not involving the treatment of bowel endometriosis: 37% had had one, 28% had had two, 8% had had three, 3% had had four and five, respectively, and 1% had had six previous procedures. Altogether, 69% of the women had some form of surgical treatment previously. None of the patients received any hormone therapy for endometriosis before surgery.
The uterosacral ligaments were involved in 61%, the bladder in 30%, and the rectosigmoid in 100% of the examined cases. There was an involvement of the pouch of Douglas in 49%, of the ovaries in 25%, of the vagina in 16%, and of the rectovaginal space in 11%; 84% had additional sites (see Table 1).
Presenting bodily symptoms
Before surgery, dysmenorrhea (94%) and chronic pelvic pain (93%) were the main complaints for the women. In addition, 69% of patients reported dyschezia, 75% dyspareunia, and 19% dysuria.
Summarized comparison of pre-and postoperative psychologic well-being
All psychologic variables improved significantly with a median follow-up of 38 months.
Detailed data concerning pre- and post-laparoscopic resection of DIE are given in Table 2 and Figure 1a and b. As shown in Figure 1a, the scales feelings of physical exhaustion and lack of motivation, lack of acceptance of one's own body, sensations of a depressed mood, and loss of body control postoperatively decreased to a significant extent. A significant reduction of general anxiety, lack of understanding, and loss of motivation for life were also observable after treatment.
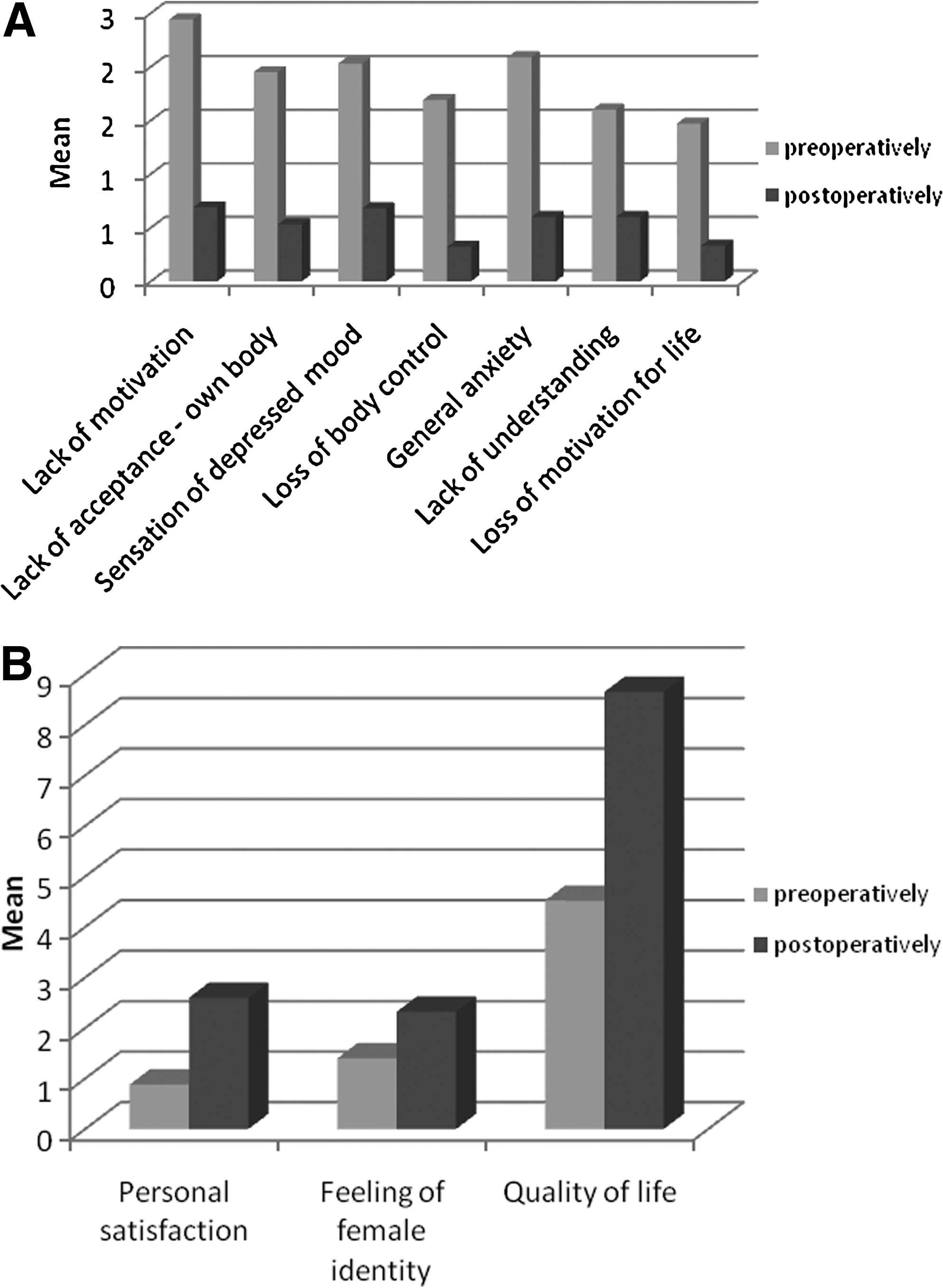
p<0.001; Wilcoxon test (2-tailed).
Furthermore, personal satisfaction and female identity increased significantly. The variable “QoL” measured via 10-point scale, rose had from an average of 4.5 points before intervention to 8.7 points after intervention (Figure 1b), which is a significant change. On the whole it can be stated that a laparoscopic radical resection of DIE leads to a significant improvement of psychologic well-being and QoL.
Discussion
Endometriosis, like many other chronic diseases, has an impact on the psychologic well-being and QoL. Causes for negative effects on psychologic health are, for example, inefficient medical and/or basic surgical interventions. 28 As a result of a wrong treatment, bodily symptoms persist, and QoL/mental health decreases steadily. There are very few long-term studies about the well-being of patients after a radical resection of endometriosis in the case of DIE. In addition to the lack of information on findings, a resection also can cause major complications, which is why opinions differ concerning a resection.20,21,31,32 In spite of all complications and divergent opinions, the results of this study demonstrate a significant increase in psychologic well-being and QoL.
The results of the current study are in line with other studies, which show an improvement in well-being and QoL almost to a normal level21,33,34 after laparoscopic radical resection.21,33,34
This is the first study that demonstrates changes in psychologic well-being using special psychologic parameters on patients with surgically removed DIE of the bowel. In this context, it is very important to point out that none of the women received any pre- and/or postoperative hormone therapy. This fact allows the conclusion that the significant improvement in psychologic well-being and QoL is solely the effect of the surgery. Studies demonstrate that the impaired psychologic well-being affects not only daily life in the same way as would bodily symptoms, but also the personality and self-esteem of these patients. 15 This is clearly noticeable in cases of dyspareunia, combined with a negative body image and bad feelings about female identity. Typical behavior patterns are anxiety, and avoidance or interruption of sexual intercourse because of pain. As a consequence, sex life for both partners is dissatisfying, and communicating the problem often is inhibited because of shame. Furthermore, patients are also less relaxed, and have fewer orgasms and intercourse episodes. 35 Therefore, dyspareunia causes difficulties in relationships, and leads to self-reproach and feelings of being unfeminine.
Demographic data show that although mental problems were present, the majority (68%) of patients in this sample did not make use of the psychologic care offered during their stay in hospital. This fact demonstrates that in the future, patients should be informed about the opportunity for psychosocial care during their stay in the hospital. There should be a focus on psychologic support in the hospital and if necessary, the period of counseling should be extended.
Furthermore, a detailed and thorough informing of patients about their conditions plays a major part in improving psychologic well-being and QoL, as it helps the patient recover the feeling of having control over her own health.
A faithful and solid physician–patient relationship during the whole course of treatment can assist in further improving the recovery of these patients. Additionally the physician should reinforce the empowerment and compliance of the patient regularly and provide psycho-educational interventions.17,36
Conclusions
The present study shows that radical surgery on patients with DIE with bowel involvement leads to an enormous improvement in their QoL and psychologic well-being.
Furthermore the preoperative data on psychologic variables conclude that patients not only need medical support, but rather a multi-professional healthcare system, as the majority of the patients have to cope with physiological symptoms and strongly reduced QoL, as well as psychologic and psychosocial problems before surgery.
Bearing these things in mind, we suggest that gynecologists should address the problem of impaired psychologic well-being during the stages of primary care and refer to a psychologist if required.
Footnotes
Disclosure Statement
No competing financial conflicts exist.