
Abstract
Abstract
Introduction
Case
A 28-year-old primigravida was referred at 16 weeks of gestation, not responding to induction of abortion with misoprostol (400 μg, two doses). On admission, she was hemodynamically stable. Abdominal examination revealed uterine height corresponding to 16 weeks of gestation. Ultrasonography showed an intrauterine dead fetus (16 weeks size). The patient was considered for extra-amniotic ethacridine lactate instillation for induction of abortion. After insertion of the 22 Fr Foley catheter, the procedure was abandoned because of the difficulty of instillation of the drug beyond 20 mL. In view of the aforementioned difficulty, an extrauterine pregnancy was suspected. Repeat ultrasound scan showed pregnancy in the right horn without any identifiable link to the cervix. There was suggestion of an empty left uterine horn having continuity with the cervical canal. As magnetic resonance imaging (MRI) or computer tomography (CT) scans were not readily available for further investigation to confirm the diagnosis, sonohysterography was performed. Examination revealed a single vagina and cervix. A 16 Fr Foley catheter was inserted into cervix and balloon inflated with 10 mL of normal saline. Under ultrasonography, Foley catheter was seen in the cavity of the left horn of uterus, which was outlined by instilling 25 mL of saline through the Foley catheter. This confirmed the diagnosis of pregnancy in the right rudimentary horn (Fig. 1). Both kidneys were normal on ultrasonography.
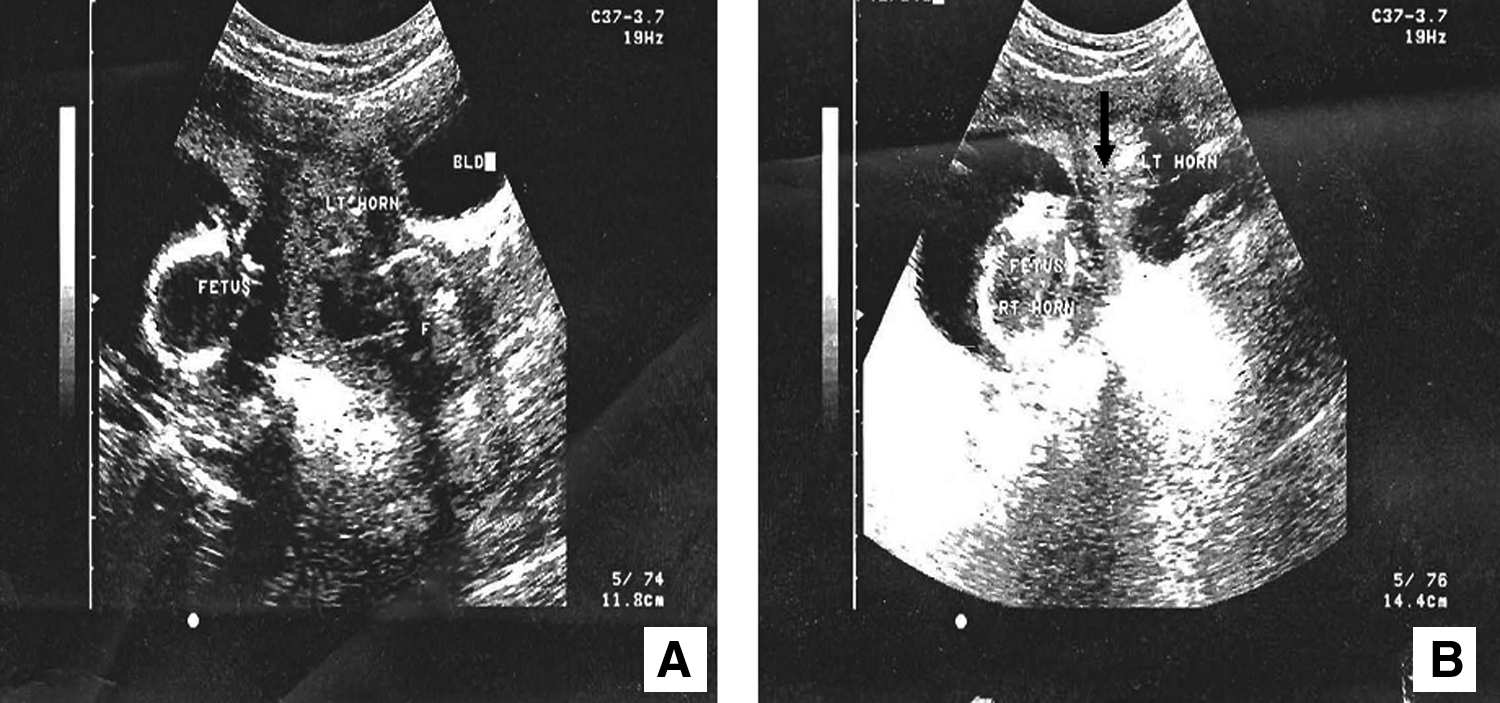
Sonohysterographic findings of women with pregnancy in right rudimentary horn
Laparotomy performed with the patient under general anesthesia confirmed pregnancy in right rudimentary horn, which was attached to the whole length of the body of the left normal uterine horn, both tubes and ovaries being normal (Fig. 2). However, there was no communication demonstrable between the rudimentary horn and the normal horn. The right uterine artery, which was supplying the rudimentary horn, was ligated and excision of the rudimentary right horn with right salpingectomy was performed. The defect on the uterus was repaired in three layers. The postoperative recovery was uneventful. The patient was counseled on contraception, the need for antenatal care, and elective cesarean delivery for any future pregnancy. She was discharged on the 7th postoperative day.
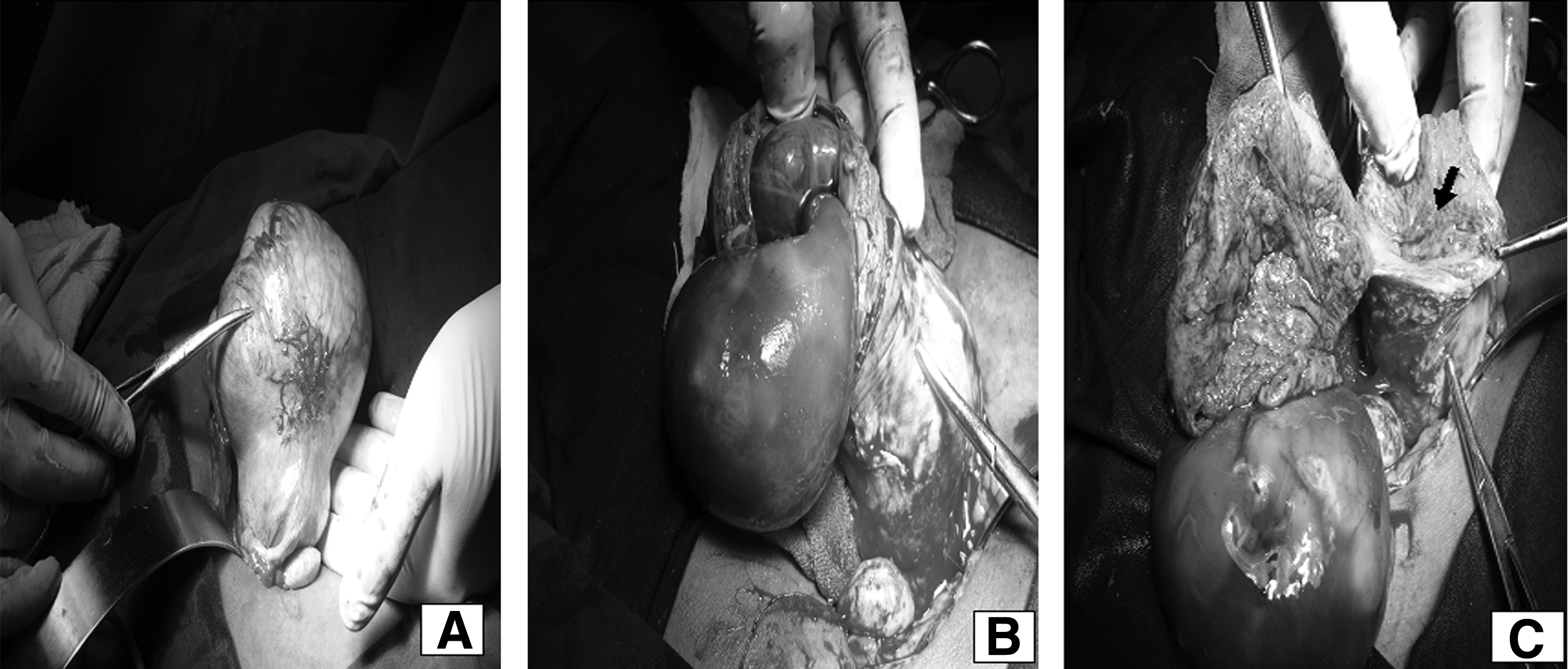
Findings at laparotomy.
Discussion
Müllerian duct malformations represent a variety of congenital anomalies resulting from arrested development, abnormal formation, or incomplete fusion of the paramesonephric ducts. Unicornuate uterus with rudimentary horn is a rare Müllerian anomaly. Approximately 90% of rudimentary horns are noncommunicating, and pregnancy is possible by transperitoneal migration of either sperm or fertilized ovum. 3
Clinically, pregnancy in the rudimentary horn might present with failure of induction of medical abortion as in this case; which may be caused by the myometrial layers having different strengths because there is less structural differentiation of oxytocin receptors. They usually present with uterine rupture; 80%–90 % in the middle trimester, remaining in the third trimester, and having only 2 % fetal salvage rate. 3
Because of the high risk of morbidity, early diagnosis is very important. Even with the advances of imaging, pre-rupture diagnosis is remarkably low. The clinical examination may provide a clue to the diagnosis early in the first trimester when the uterus and the rudimentary horn are still in the pelvis. 4 There are small case series and reports that highlight the usefulness of ultrasonography and MRI in the pre-rupture diagnosis of this condition.3–6
The sensitivity of ultrasonography is reported to be ∼25% for the diagnosis, which decreases with advancing gestation beyond the first trimester. 3 Different criteria have been proposed for the sonographic diagnosis of pregnancy in the rudimentary horn. If available, MRI can confirm the condition before the patient is subjected to surgical procedure. In resource-poor settings, where a facility for MRI or emergency laparoscopy is not available, sonohsyterography can confirm the diagnosis.
Sonohysterography is very useful and inexpensive and requires less skill and experience to perform than other procedures. There are only a few reports that advocate the usefulness of this procedure in the diagnosis of rudimentary horn, especially when the rudimentary horn is firmly attached to the unicornuate uterus as in this case. 7 In this case, the appearance of an extra uterine gestation surrounded by a very thin layer of myometrium and the inability to demonstrate communication between the single cervix and the gestational sac on sonohysterography suggested the diagnosis of rudimentary horn. As a noncommunicating horn with functional endometrium usually presents early in the adolescent years, with hematometra or severe dysmenorrhea, the absence of symptoms in this case raises the possibility of very thin communication not visible to naked eye between the horns. Excision of the rudimentary horn with ipsilateral salpingectomy is the recommended treatment once the diagnosis is made. 3 The ipsilateral fallopian tube should be removed because of the possibility of an ectopic pregnancy developing later. 2
Conclusions
In conclusion, sonohysterography can be considered as a safe and cost-effective alternative for the diagnosis and confirmation of pregnancy in the rudimentary horn; especially in a low-resource setting.
Footnotes
Disclosure Statement
No competing financial conflicts exist.