
Abstract
Abstract
Introduction
Case
A 40-year-old woman presented with a 1 year history of a progressively enlarging abdominal mass on right side associated with abdominal pain. Her menstrual history was unremarkable. Physical examination showed a pelvic mass. Abdominal ultrasound showed a hyperechoic solid cystic mass in the right ovary measuring 12×7.5 cm. Contrast-enhanced computed tomography (CECT) of the abdomen showed a large ill-defined solid cystic mass in the right ovary measuring 12×7cm, and massive ascitis (Fig. 1). The left ovary was unremarkable. Results of routine hematologic and biochemistry investigations were all within the normal range. Initial investigation of tumor markers before surgery showed markedly elevated serum CA-125 (2142 U/mL; reference range 0–30 U/mL); but other markers including carcinoembryonic antigen (CEA) and CA 19-9 were all within the reference range. The patient underwent a staging operation including total abdominal hysterectomy with bilateral salpingo-oopherectomy (TAH-BSO), infragastric omentectomy, and pelvic lymph node dissection. A large amount of ascitis (∼2000 mL) in the pelvic cavity was found intraoperatively, and sent for cytologic examination. Postoperatively, serum CA-125 levels were reduced (98 U/mL). Microscopic examination showed TCC of the right ovary. Parametrium and pelvic lymph nodes were free of tumor, and cytology of ascitic fluid was also negative for malignant cells. A final diagnosis of TCC of the right ovary, high grade, stage Ic was made. After recovering from surgery, the patient received postoperative chemotherapy with carboplatin (300 mg/m2) and paclitaxel (160 mg/m2), every 3 weeks for six cycles. CA-125 levels returned to normal (11.5 U/mL) after completion of chemotherapy. The patient is being regularly followed up and has been disease free for 5 months.

Computed tomographic (CT) scanof the abdomen showing a solid cystic mass in the right ovary.
Pathologic Examination
A specimen from the TAH-BSO in addition to specimens containing omentum, aortic and paraaortic lymph nodes, right and left external iliac lymph nodes, and right pelvic lymph nodes were received. The hysterectomy specimen showed a right ovarian mass measuring 12×7×6 cm. A cut section showed a gray-white solid cystic tumor having hemorrhagic and necrotic areas (Fig. 2). Areas of capsular breech were also identified. The left-sided adnexa and the right- sided fallopian tube were unremarkable. The received omentum and excised lymph nodes were also grossly unremarkable.

Panhysterectomy specimen showing solid cystic mass in the right ovary.
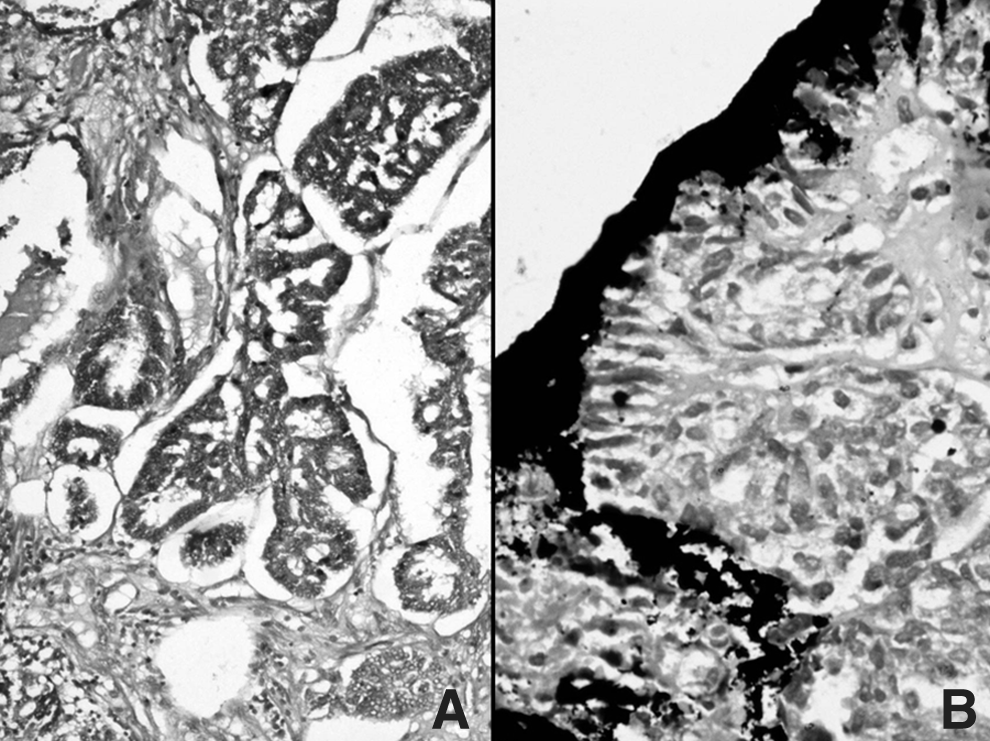
Hematoxylin and eosin stained sections revealed a malignant surface epithelial neoplasm in the right ovary, with the majority of areas showing morphology of TCC. No areas of benign or atypical proliferative Brenner component were identified. The majority of areas showed thick, blunt papillary projections with fibrovascular core lined by transitional type epithelium (Fig. 3). Most of papillary folds arose from cystic spaces and showed infiltrative growth of epithelium into the cyst wall. At places, solid sheets having scant fibrovascular support (Fig. 4) in addition to areas of desmoplastic stroma were identified. Foci of glandular differentiation, thin papillae of serous papillary carcinoma (Fig. 5A), stromal inflammation, and areas of necrosis were also seen. Cytologically, cells lining the papillae were round-to-oval with vesicular chromatin, conspicuous nucleoli, and nuclear grooving at places with prominent mitotic activity. The tumor was infiltrating the ovarian capsule at places (Fig. 5B).
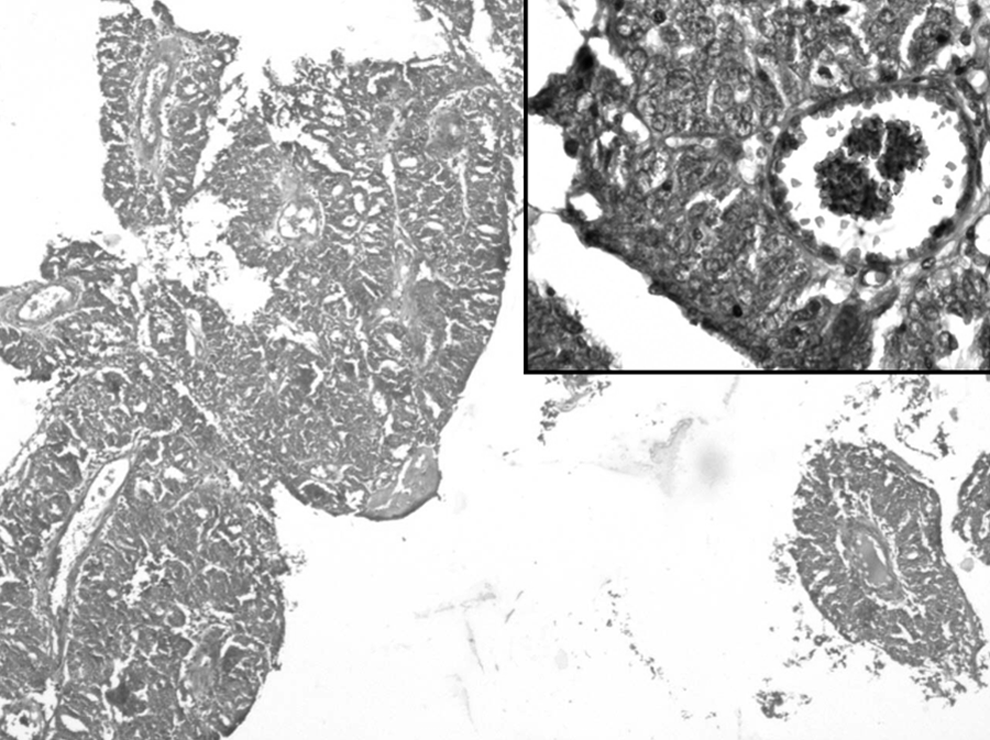
Photomicrograph depicting multilayered papillary architecture of tumor (hematoxylin and eosin [H&E]×10) and inset showing high power view of true papillae lined by transitional type epithelium having nuclear atypia (H&E×40).

Photomicrograph showing fused papillary configuration (hematoxylin and eosin [H&E]×10).
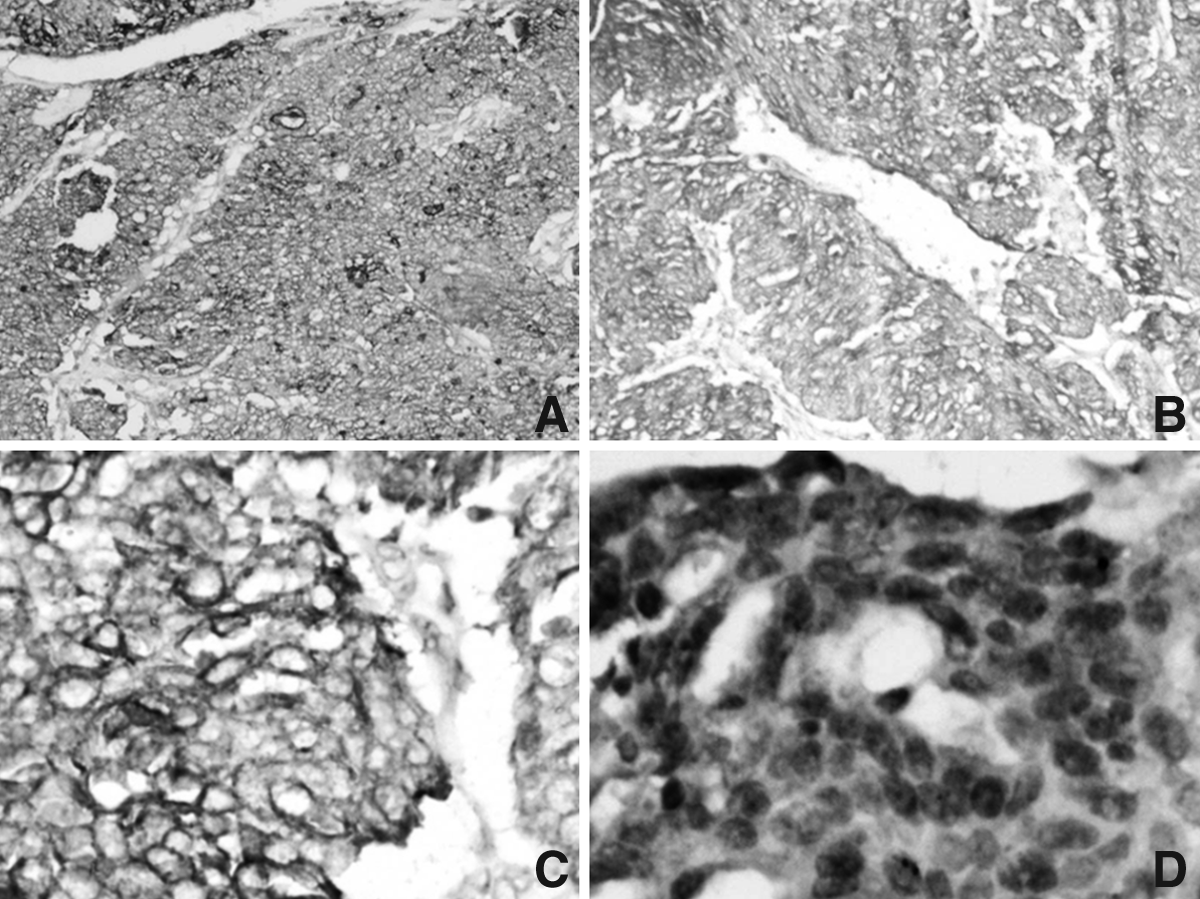
A panel of immunostains composed of cytokeratin (CK)7, CK20, CA-125, estrogen receptor (ER), human epithelial growth factor (HER)2neu and vimentin were applied to rule out metastatic urothelial malignancy in the ovary. Tumor cells marked positive for CK7, CA-125, ER, Her2neu and negative for CK20, thus indicating primary TCC of the ovary (Fig. 6A–D).
Discussion
TCC-O is a rare, recently recognized subtype of ovarian surface epithelial neoplasm, which was first defined by Austin and Norris. 1 It has been described as primary ovarian carcinoma in which definite urothelial features are present, but no benign, metaplastic and/or proliferative Brenner tumor can be identified. 2 In addition, pure TCC also lacks prominent stromal calcification, which is commonly seen in malignant Brenner tumor. 3
The true incidence of pure TCC-O remains unknown. The histologic pattern of TCC is often mixed with other types of carcinomas, the most common being papillary serous carcinoma.4,5 More than 50% of tumor should display a pattern of TCC for a diagnosis of TCC-O. TCC-O has close morphologic similarities to TCC of the bladder, and it behaves more aggressively than malignant Brenner tumor. Austin and Norris, therefore, concluded that TCC-O arises directly from pluripotent surface epithelium of the ovary and from cells with urothelial potential, rather than benign or proliferative Brenner tumor precursor.1,3
When TCC-O is encountered, the main differential diagnosis is metastasis from the urinary tract and malignant Brenner tumor.3–6 The site of origin of the tumor can be decided by the pattern of distribution of disease and immunohistochemical (IHC) staining.7–9 TCC-O is negative for CK20, thrombomodulin (TM) and uroplakin III in comparison with bladder TCC, which is usually positive for CK20 or sometimes positive for TM and uroplakin III.2,7,8 TCC-O is also often positive for CA-125, Her2neu and Wilms' tumor protein (WT1). 2 Croft et al. 10 concluded that almost all TCC-O are strongly positive for ER, a characteristic that helps to differentiate TCC-O from papillary urothelial carcinoma metastasis to the ovary. The tumor in this case was also positive for CK7, CA-125, ER, and Her2neu and negative for CK20, thus confirming diagnosis of primary TCC-O. The IHC staining pattern thus indicates that morphologic similarities between TCC-O and TCC of the bladder does not indicate any histogenic similarities, and TCC-O is a morphologic variant in the spectrum of surface epithelial ovarian carcinomas.7,11
TCC-O is subtype of ovarian surface carcinoma and appears to be more aggressive than other non-TCC ovarian carcinomas. 12 The treatment is composed of TAH-BSO and postoperative chemotherapy. Although TCC-O is clinically aggressive, it seems to respond well to chemotherapy, and patient outcomes after chemotherapy are better than for other types of common epithelial ovarian carcinomas.13–15
Conclusions
To conclude, TCC-O is a rare subtype of epithelial ovarian carcinoma. The histopatholgist should keep in mind this rare entity while reporting ovarian surface carcinomas with urothelial morphology. The immunophenotype of TCC-O is similar to that of other surface carcinomas of the ovary, but different from that of TCC of the bladder, therefore making it possible to differentiate from bladder metastases. Surgical resection is the primary therapeutic approach, and patient outcome after chemotherapy is better than that for other types of ovarian cancer.
Footnotes
Disclosure Statement
No competing financial conflicts exist.