
Abstract
Abstract
Introduction
Absence of a functional vagina can, less frequently, be a consequence of radiation, trauma, surgery, or chemical treatments. 2
There are several treatments for creating a neovagina, and there is no consensus about the best option. However, it is agreed that the treatment should only be offered when the patients are ready to start sexual activity. Moreover, both medical and psychological assistance to the patient and her family are necessary before and throughout the treatment.3,4
The first option to create a neovagina is a nonsurgical procedure – progressive vaginal dilation – as described by Frank. 5 Both retrospective 6 and prospective studies 7 have demonstrated highly successful rates for this procedure, although the use of the dilators can be uncomfortable and unpleasant, 8 and the whole process can last several months.
When surgical treatment is indicated, the options currently used are the Vecchietti procedure, the Davydov technique, the intestinal vaginoplasty, and the Abbe–Mcindoe vaginoplasty. Studies have reported good results with both the Vecchietti and the Davydov techniques, which can be performed laparoscopically. But as is the case with intestinal vaginoplasty, these techniques require abdominal surgery. On the other hand, the Abbe–McIndoe vaginoplasty has the advantage of being a perineal procedure in which, recently, other materials have been used as an alternative to skin graft for lining the vaginal mold, thus modifying the original technique. 3
In 1984, Dhall described the use of the amniotic membrane to generate prompt and proper epithelization and metaplasia in the vaginal mucosa. 9 The inconvenience of this technique is that it requires the selection, acquisition, and preservation of the amniotic membrane. Another issue is the risk of transmission of diseases such as hepatitis and other virus infections through the graft. Seeking to minimize these complications, alternative materials to re-cover the neovagina were sought. 10
In 1994, Jackson and Rosenblatt described for the first time the use of the Interceed® in the lining of the vagina in 4 patients. 10 The authors had decided to use the material because the amniotic membrane that was prepared for the surgery was accidentally contaminated.
Interceed is a biodegradable fabric made of oxidized regenerated cellulose, and it is designed to reduce the formation of postsurgical adhesions. It has been used in pelvic surgeries, effectively reducing the incidence and extension of adhesions.11,12 In neovaginoplasty, the membrane is placed on the injured area, and it appears to form a gelatinous layer that provides mechanical protection during the process of epithelization. These factors were a motivation to explore further uses for the oxidized cellulose membrane. 13
In 2003, Motoyama et al. described the use of Interceed in 10 patients with vaginal agenesis. There were no operative complications, and the coverage of the entire vaginal cavity by a vaginal epithelium was observed after 2 postoperative months. 14
Later on, Sharma et al. and Dadhwal et al. published their results using Surgicel®, which is another oxidized cellulose membrane.15,16 Ten patients were evaluated in each study and both authors obtained good success rates.
In the current study, the morphologic aspects of the McIndoe neovaginoplasty with the use of the oxidized cellulose membrane (Interceed) to create a neovagina were evaluated.
Methods
We prospectively evaluated 10 patients at the Division of Urogynecology of the Federal University of Sao Paulo, following protocol previously approved by the Ethics Committee of the University. All patients gave their informed consent before the surgical intervention.
The group included 7 patients diagnosed with vaginal agenesis (70%) and 3 patients presenting vaginal atresia and functional uterus (30%). The patients with congenital defects ranged from 12 to 26 years of age (average 18.9 years of age). The main complaints by the patients were amenorrhea (45.4%), dyspareunia characterized by difficulty of penetration during sexual intercourse (36.2%), cyclic abdominal pain (9.2%), and association of dyspareunia and cyclic abdominal pain (9.2%). All patients with congenital defect of the vagina received karyotype, magnetic resonance imaging (MRI) of the pelvis, and urography (Table 1).
All patients underwent a colon preparation the day before the procedure. Under spinal anesthesia with sedation, the patients were placed in the gynecologic position and a urethral catheter was inserted. A neovaginoplasty by a modified McIndoe technique using Interceed was then performed. A cruciform incision was made in the vaginal vestibule and a vaginal cavity was created by opening the rectovesical plane by blunt dissection after local infiltration of adrenaline solution 1:20,000 concentration. A cavity size of 10 cm in length and 4–5 cm in diameter was achieved (Fig. 1). A cylindrical mold coated with Interceed was introduced after a rigorous hemostasis. Measuring 9.5 cm in length and 3.5 cm in diameter, this mold was inflatable and malleable, with a drainage system (Silimed®) (Fig. 2). Finally, the new vagina was closed approaching the labia majora with two polyglactin number 0 sutures (Fig. 1). The average time of the surgery was 77.5 minutes.

Neovaginoplasty by McIndoe technique.

Cylindrical mold coated with Interceed.®
Within the group of patients with vaginal atresia and a functioning uterus, although 1 patient was subjected to hysterectomy, it was possible to preserve the uterus communicating to the new vagina in the other 2 cases.
The hospital stay was 7 days, during which the patients remained on bed rest receiving a light fiber-free diet and antibiotic therapy with metronidazole and cephalosporin. In addition, deep venous thrombosis prophylaxis with elastic compression stockings and passive movement of the lower limbs were prescribed. On the 7th postoperative day, both the sutures and the mold were removed, and the cavity was washed and examined. Patients were given instructions and were advised to use the mold continuously, except during defecation. They were discharged 24 hours after the removal of the sutures and examination.
Follow-up visits occurred weekly during the first postoperative month and monthly thereafter. The evaluation consisted of interviews to find out about complaints related to abnormal discharge, bleeding, and pain as well as examination of the neovagina. For those patients with sexual partners, vaginal intercourse was allowed 3 months after the procedure and the quality of their sexual life was also assessed.
For the first 3 months, fragments of the vaginal mucosa, preferably from the upper third portion of the canal formation, were collected once a month. Fragments were collected again 9 months after the surgery. The material was preserved in buffered formalin 10% and sent to the Department of Histology for laboratory analysis.
The material was conveniently dehydrated in ethanol, then cleaned by xylene and impregnated with liquid paraffin, and, finally, put in an oven at 59°C, according to Masson's method (1956). In the third paraffin bath, the material was then included.
The blocks were cut in microtome type Minot (American Optical brand, model 820), adjusted to 5 μm. The sections were placed on slides previously coated with Mayer's albumin and kept in the oven at 37°C for 24 hours for drying and gluing. Sections were then stained with hematoxylin and eosin for morphologic description.
Results
The first biopsy 1 month after the procedure revealed the presence of granulated tissue rich in blood capillaries, fibroblasts, lymphocytes, plasma cells, neutrophils, and some macrophages on the samples. The presence of isolated or grouped cells of epithelial type was also observed on the free surface, thus suggesting the formation of vaginal epithelial tissue (Fig. 3). Two months after the surgery, the presence of granulated tissue remained, and on the free surface, numerous epithelioid cells, forming islets or grouped as a layer, were observed. In the 3rd month, a granulated tissue of epithelial type cells forming layers of well-defined stratified epithelial tissue on the free surface could be identified. After 9 months, the biopsy showed typical vaginal mucosa or stratified vaginal epithelium and lamina propria consisting of connective tissue rich in blood vessels (Fig. 4). A typical vaginal epithelium containing well-differentiated epithelial layers (superficial, intermediate, and basal) was observed. The reaction for an identification of glycogen (PAS) was positive, thus indicating that a typical vaginal epithelium had been formed.

Photomicrograph of a fragment of the vaginal wall, 1 month after the neovaginoplasty with oxidized cellulose. Observe lamina propria rich in blood vessels and epithelioid cells. Hematoxylin and eosin (HE) 113×84mm.
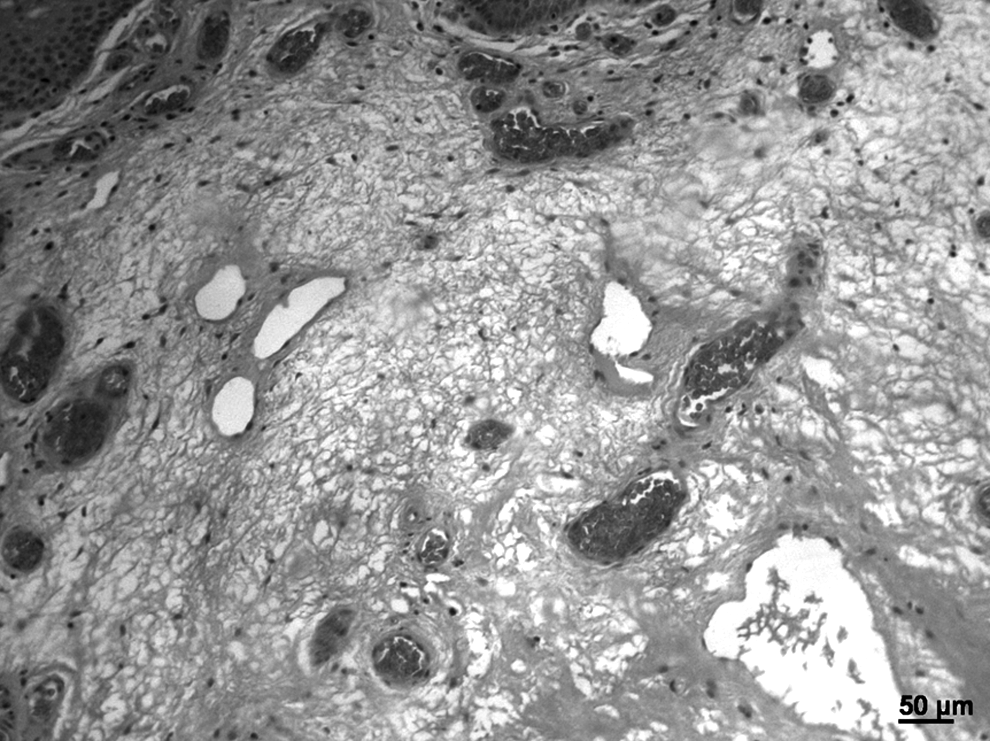
Photomicrograph showing fragment of the vaginal wall after 9 months of neovaginoplasty with oxidized cellulose. Observe lamina propria containing connective tissue. Hematoxylin and eosin (HE) 146×109mm.
Discussion
Although nonsurgical treatment should be the first option in the management of vaginal agenesis, it requires motivation and persistence, and it takes time. Therefore, surgery often becomes the solution for obtaining a functional vagina.
There are many reported techniques, and there is no consensus about the best option. The ability and experience of the surgeon in the specific technique remain crucial to the choice.
The Abbe–McIndoe vaginoplasty has been performed at the Division of Urogynecology of the Federal University of Sao Paulo as the treatment for vaginal agenesis. Compared with techniques that use the peritoneum and intestine, this procedure has advantages such as shorter hospital stay and absence of abdominal incision. Moreover, the use of alternative materials, instead of skin graft, to coat the mold, avoids unaesthetic scars, thus making the procedure even more advantageous.
The use of the amniotic membrane, as proposed by Dhall, 9 may result in the transmission of viruses or prions. In the university hospital, the presence of hepatitis C virus was identified by polymerase chain reaction (PCR) test in a donor's amniotic membrane, which had a negative sorologic result. In addition, the increased difficulty in obtaining and preserving the amniotic membrane was a motivation to start using the oxidized cellulose membrane (Interceed).
The histologic evaluation made in this study showed the organization of epithelial tissue, typical of the vagina, 1 month after the surgery, and complete epithelization at 9 months postoperative for 100% of the patients. Similarly to Motoyama et al., Sharma et al., and Dadhwal et al.,14–16 good results were observed in this study, and there were no complications regarding the oxidized cellulose membrane.
Conclusions
Therefore, it can be concluded that the oxidized cellulose membrane is an interesting alternative material to be used in neovaginoplasty. It is a material that is available, and although it has non-stick properties, it also results in excellent postoperative epithelization. Moreover, it does not involve additional surgical procedures and it does not expose the patient to the risk of virus infection from transmission. Nevertheless, congenital vaginal agenesis is a rare condition and as a result, only a small number of cases have been evaluated until now. Further studies on more subjects with longer follow-up analyses are necessary.
Footnotes
Disclosure Statement
No competing financial interests exist.