
Abstract
Abstract
Introduction
Minilaparotomy (defined as an incision of ≤6 cm) for hysterectomy is a feasible and efficient approach. 2 Moreover, laparoscopy is expensive and has a long learning curve. 3 Minilaparotomy using an elastic self-retaining retractor, which gives better exposure during surgery, can be used instead of laparoscopy and at a lower cost. 4 It has been shown to be a good alternative to laparoscopic hysterectomy and can be used when there is a lack of expensive equipment or gynecologists who lack the expertise in laparoscopic techniques. 5 The use of minilaparotomy with elastic self-retaining retractor (Mobius, Apple Medical, Marlborough, MA) for both adnexal masses and large uteri is described.
Cases
Case 1
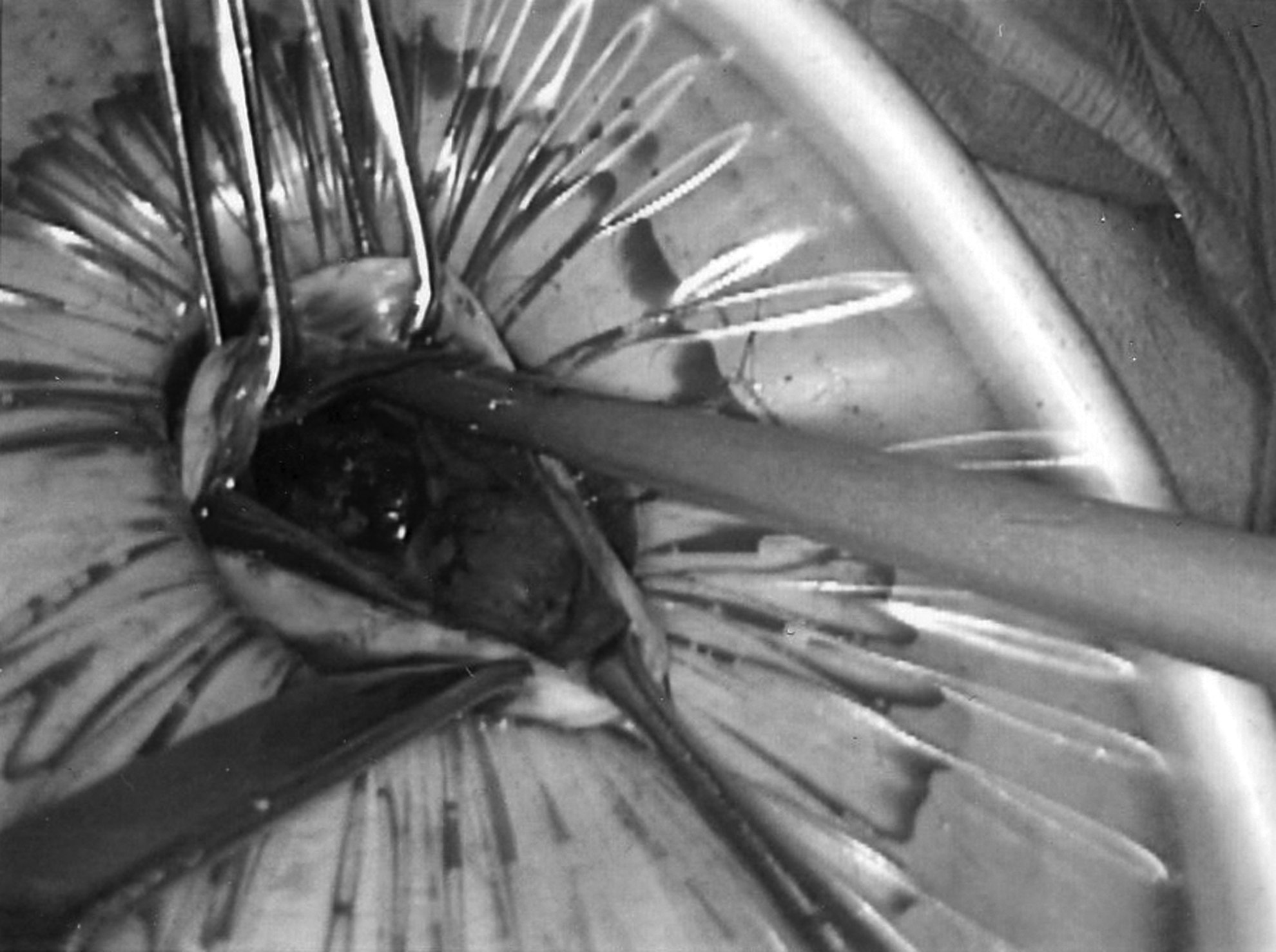
A 19-year-old nulliparous woman was referred for a pelvic mass. Ultrasound and computed tomography (CT) scan revealed a 28×19×12 cm unilocular cystic mass with a nonenhancing thin wall, likely arising from the right ovary. The patient had no medical problems and CA-125 was within normal limits. On clinical examination, a cyst was seen to be extending from the pelvis to the ribcage. A 4 cm subumbilical midline incision was made. The abdomen was opened in layers and an elastic self-retaining retractor was placed. The cyst was found to be smooth walled. A view of the cyst with the self-retaining retractor is shown in Figure 1. The cyst was drained with a needle attached to the suction. The cyst was then pulled out through the incision. It was noted to be a paratubal cyst with complete destruction of the distal tube. The fimbrial end could not be visualized, and a right salpingectomy was then completed. The left tube and both ovaries were completely normal. Estimated blood loss for the procedure was 30 cc, operative time was 48 minutes. The patient was discharged home the next day. Final pathology showed a paratubal cyst and segment of unremarkable fallopian tube.

Case 1. Visualization of the adnexal cyst through the self-retaining retractor.
Case 2
A 24-year-old woman presented with a pelvic mass. Ultrasound showed a 17×10×16 cm cystic mass obscuring most of the pelvis. CT Scan showed the mass to be 22×15×10 cm. There were no septations and no adenopathy. CA-125 was within normal limits and the patient had no medical problems. On examination, the patient was found to have a 32 weeks-sized mass. A 4.5 cm transverse suprapubic incision was made. An elastic self-retaining retractor was placed. Suction was then performed. Edges of the cyst were opened and held with an Allis Clamp. Multiple loculi were noted and were broken down, and all fluid was suctioned out (Fig. 2). Lap pads were placed around the cyst to avoid any spillage into the peritoneal cavity. The cyst was seen to be arising from the right ovary and no identifiable viable ovarian tissue was noted. Right salpingo-oophorectomy was completed. The uterus and the left tube and ovary were normal. Frozen section and the final pathology confirmed the mass to be a benign mucinous cystadenoma. Estimated blood loss for the procedure was 40 cc, operative time was 45 minutes. The patient was discharged home the next day and recovered well.
Case 2. Drainage of the adnexal cyst through the minilaparotomy incision.
Case 3
A 40-year-old nullipara was referred for a right-sided adnexal mass. Ultrasound and magnetic resonance imaging (MRI) showed a right-sided ovarian cyst measuring 14×12×10 cm. There was no lymphadenopathy and no other abnormal findings. CA-125 was within normal limits. A 4 cm midline subumbilical incision was made. The abdomen was opened in layers and a right ovarian cyst was found. The cyst was then drained and 400 cc of fluid was removed. After decompression, the cyst was completely brought out of the incision. No identifiable ovarian tissue was noted and right salpingo-oophorectomy was completed. The size of the incision after removal of the retractor is shown in Figure 3. Frozen section and final pathology confirmed it to be a benign mucinous cystadenoma. The patient's estimated blood loss was 30 cc, operative time was 1 hour and 2 minutes, and the patient was discharged the next day.

Case 3. Skin incision after removal of the retractor.
Case 4
A 38-year-old woman presented with a large fibroid uterus. Examination revealed a 32 week sized fibroid uterus, which was confirmed by CT scan. The patient had a midline subumbilical incision measuring 6 cm. The abdomen was opened in layers, and a self-retaining elastic retractor was placed (Fig. 4). A round ligament was ligated and transected on either side. The uterus was morcellated with a scalpel to gain further access. The infundibulopelvic and uterine pedicle was ligated and transected on either side. Uterosacral ligaments were ligated and transected and the uterus was removed. Estimated blood loss was 200 cc, operative time was 1 hour and 44 minutes, and the patient was discharged home the next day.

Case 4. Elastic self-retaining retractor placed through the abdominal incision.
Case 5
A 47-year-old nulliparous woman presented with a 34 week sized fibroid uterus. She underwent a minilaparotomy with a 6 cm midline incision. An elastic self-retaining retractor was placed, and hysterectomy was completed in a fashion similar to Case 4. The morcellated uterus is shown in Figure 5. Estimated blood loss was 220 cc, operative time was 1 hour and 35 minutes, and the patient was discharged home the next day.

Case 5. Morcellated uterine specimen (corresponding to 34 weeks of gestation) removed through minilaparotomy incision.
Discussion
Minilaparotomy has been shown to be a useful option in benign gynecologic surgery.4–7 Minilaparotomy for large masses using the elastic self-retaining retractor is described here. The use of this retractor has multiple advantages, as first described by Pelosi and Pelosi. 8 It provides retraction circumferentially in a uniform fashion, thus maximizing exposure. As it can adapt to the thickness of the abdominal wall, it can be used in obese patients with success. In contrast, metal retractors produce asymmetrical traction, which can be excessive, and can cause hematomas and postoperative pain.
All of our patients were discharged on postoperative day 1. Blood loss was minimal in every case and there were no complications. Large uteri were removed with the help of scalpel morcellation. This technique is not only cosmetically more appealing to the patient, but also financially advantageous in comparison with conventional laparotomy.
Minilaparotomy is an excellent alternative to laparoscopy in institutions that do not have the appropriate equipment or if the surgeon does not have expertise in laparoscopy.
A potential concern with this technique is the possibility of spillage of cyst fluid from malignant ovarian cysts. Therefore, careful patient selection is of the utmost importance, and even then, extreme care should be taken to avoid spillage during surgery.
Conclusions
In conclusion, minilaparotomy with a self-retaining elastic retractor is a useful alternative to traditional laparotomy and laparoscopy. It is feasible, safe, and cost effective. The technique described here provides a good alternative to traditional laparotomy and laparoscopy, and patients will benefit from this innovative procedure.
Footnotes
Disclosure Statement
No competing financial conflicts exist.