
Abstract
Abstract
Introduction
Four more cases were reported;15,16 however, as the authors could not be contacted, their articles are not included in this table.
Pr. infertility, primary infertility; Diagn, diagnosed; L/S, laparoscopy; L/T, laparotomy, MOS, months.
Cases
Case 1
A 32-year-old nulliparous patient was referred for infertility to the Department of Obstetrics and Gynecology, Samsun Education and Research Hospital 1 year after her only pregnancy resulted with abortion at the 6th gestational week. Her menstrual cycles had been regular (within 27–30 day intervals). In 2008, she had surgery to repair an atrial septal defect, but had had no abdominal surgery. She was not taking any medications. She did not have any history of acute or severe abdominal pain. Findings from a pelvic examination were normal. The right ovary and uterus were normally visualized on transvaginal ultrasound, but the left ovary was not seen. Day 3 hormonal profile was normal. Hysterosalpingography demonstrated a normal uterine cavity and right Fallopian tube, but the left Fallopian tube could not be visualized beyond the isthmic portion. During diagnostic laparoscopy, the right ovary and right Fallopian tube were seen to be anatomically normal, and chromopertubation test was positive. However, the left Fallopian tube was absent beyond the isthmic level, as was the left ovary. Other intra-abdominal and pelvic structures were normal. On computed tomography, both kidneys and the urinary tract appeared normal.
Case 2
A 19-year-old patient was referred to the Department of Obstetrics and Gynecology, Samsun Education and Research Hospital suspected of being pregnant. At laboratory evaluation, β-human chorionic gonadotropin was 2134 milli-international units (mIU)/mL and progesterone was 2.17 ng/mL. The patient's first pregnancy had resulted in abortion at the 6th gestational week 2 months earlier. Her menstrual cycles had been regular (within 30 day intervals). She had no history of abdominal surgery or severe pelvic pain. On transvaginal ultrasound, the uterus was antevert, and the endometrium was 15 mm thick. The right ovary could not be visualized, but the left ovary was normal. As the patient had had sudden onset abdominal pain and vaginal bleeding, and the transvaginal ultrasound demonstrated intra-abdominal fluid, it was decided to perform laparoscopy, with a pre-diagnosis of ectopic pregnancy. At laparoscopy, there were fine adhesions between the uterus and the intestines, and some blood in the pelvis. Ruptured ectopic pregnancy focus was seen in left Fallopian tube's ampullary region. Salpingostomy was performed, the gestational sac was removed, and the bleeding was controlled. The chromopertubation test was positive in the left Fallopian tube but it was negative in the right Fallopian tube. The right Fallopian tube could not be visualized beyond the isthmic level, and the right ovary was also absent (Fig. 1). Other intra-abdominal structures were normal.
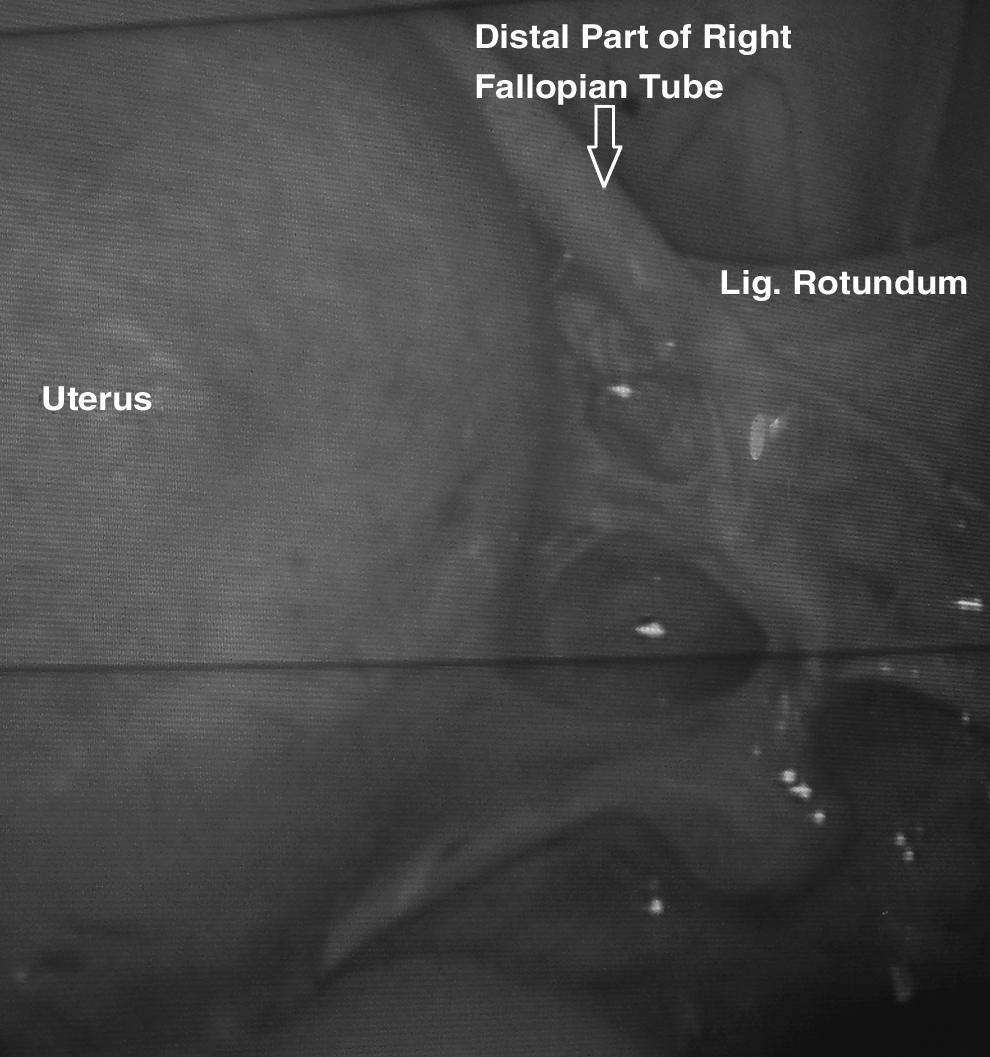
Absence of right Fallopian tube and ovary in case 2.
Results
Case 1
After completion of infertility workup, the patient was scheduled to undergo controlled ovarian hyperstimulation and intrauterine insemination for 3 cycles.
Case 2
A linear salpingostomy was performed and the gestational sac was removed.
Summary
Both patients were informed about their extraordinary situation and its unclear clinical consequences.
Discussion
Unilateral absence of adnexae and the ovary is a very rare condition (only 24 cases were previously reported) with unknown etiology and clinical consequences (Table 1). This situation gains clinical significance especially when the contralateral Fallopian tube and/or the ovary are affected by a pathology such as an ectopic pregnancy, tubal occlusion, or an ovarian disease necessitating oophorectomy. This is difficult to diagnose with radiologic and ultrasonographic imaging techniques; therefore, all patients have been diagnosed at laparotomy or laparoscopy up to until now. Whether this absence underlies the complaints of the patients such as pelvic pain, infertility, and ectopic pregnancy, or whether it coincidentally exists, is debatable. For all these reasons, the true incidence of absence of unilateral adnexa is hard to estimate. It was reported to be 1:11,241. 15
Many different explanations were proposed to explain the underlying etiology; however, the different embryologic origins of these two structures make the situation more interesting, but also make it more difficult to explain. In intrauterine life, Fallopian tubes originate from the paramesonephric (Müllerian) duct system. Ovaries, as undifferentiated gonads at ∼ the fifth gestational week, include mesonephric cells (which will develop into ovarian medulla), coelemic epithelial cells, and primordial germ cells (originating from the ectoderm) in the genital ridge lying above the mesonephros. In cases in which both ductal systems were affected together, other urinary-tract or uterine anomalies were also expected; however, only 4 of 24 reported cases had such anomalies. Nevertheless, a defect in the development of the genital ridge and mesonephros in early embryogenesis cannot be excluded.
Another proposed explanation was maldevelopment secondary to a vascular accident, probably in intrauterine life. The vascular supply of Fallopian tubes also include branches from uterine arteries; therefore, occlusion of the ovarian blood supply would have a minimal effect on Fallopian tube genesis. However, an occlusion of the uterine artery or its branches would affect the uterus and vagina in addition to the Fallopian tubes, rather than the adjacent ovary. In addition, cases with absent ovaries together with aplasic 4 or twisted 1 contralateral tubes were also reported. When all these issues are taken into account, a vascular accident hypothesis seems improbable.
An intrauterine adnexal torsion was also suspected. 15 Separated ovarian and tubal tissue remnants in the abdominal cavity, partial agenesis, or twisting of the tube favor this hypothesis. 1 Although no precise data either to support or to deny this hypothesis exist, it is also believed that this is the most probable explanation.
Timing of the underlying pathology is another subject of debate. Unilateral absence of the ovary associated with a rudimentary left Fallopian tube tightly stretched over the sigmoid colon to the left retroperitoneum was diagnosed incidentally in a 8-month-old female during laparotomy for persistent ovarian cyst. 5 Based on this report, it can be assumed that the underlying event most probably occurs in intrauterine life.
Clinical presentations of previously reported cases differed (Table 1). Some of the previously reported patients presented with pelvic pain,1,10 and some other cases were discovered during infertility workup in Case 1 in this article and others1,8,9 or incidentally.2,14 Only 1 patient with tubal ectopic pregnancy and contralateral tubal and ovarian agenesis (similar to Case 2 in this article) was reported. As a clinical outcome of this absence, function of the existing tube is debatable, despite that its patency is demonstrated with chromopertubation: infertility or ectopic pregnancy arouses suspicion of a functionally abnormal tube, whereas incidentally diagnosed absence in fertile patients opposes this hypothesis. True incidences of such abnormalities in both normal and infertile populations are needed to clarify this point.
Conclusions
Although very rare, unilateral absence of Fallopian tubes and ovaries may compromise fertility, especially if a contralateral tube and/or ovary are affected by a pathologic situation. Therefore, contralateral adnexa should be visualized before any intervention with a Fallopian tube or ovary.
Footnotes
Disclosure Statement
No competing financial interests exist.