
Abstract
Abstract
Introduction
AT is a benign tumor of mesothelial origin. It is rare and is preferentially found in the genital tracts of both males and females. 7
This case report describes a leiomyo-adenomatoid tumor of the uterus of a 24-year-old woman. The findings are similar to a case report by Amérigo et al. 1
Case
A 24-year-old woman (gravida 1, para 0) was referred from her general practitioner for gynecologic evaluation. She had been using second-generation contraception (ethinylestradiol and norgestimate) for several years. She presented with diminishing menstruation, increased vaginal discharge, a sense of cervical descent, and occasional dyspareunia. On physical examination, her vulva, vagina, and cervix were found to be normal but a plump area was palpated around the cervix. Transvaginal ultrasonography revealed a 22×20–mm myoma on the anterior cervico-corporal junction. Follow-up was arranged 6 months later, at which time the myoma was found to be unchanged in size. At a second follow-up, 1 year after the first contact, she complained about increasing dyspareunia and pollakiuria. The size of the myoma had increased to 26×23 mm. She was offered laparoscopic myomectomy and accepted the protocol. Five months later, the operation was performed without complications. Postoperatively, there were no reports on reappearance of symptoms, but a cervical smear previously taken revealed the presence of a low-grade squamous intraepithelial lesion.
Grossly 3.5×3.5×2 cm of shredded material was available for examination. It consisted partly of white cylindrical tissue fragments with a white-to-yellow surface and a whorled texture. A few minor hemorrhages were seen on the sectioned surface.
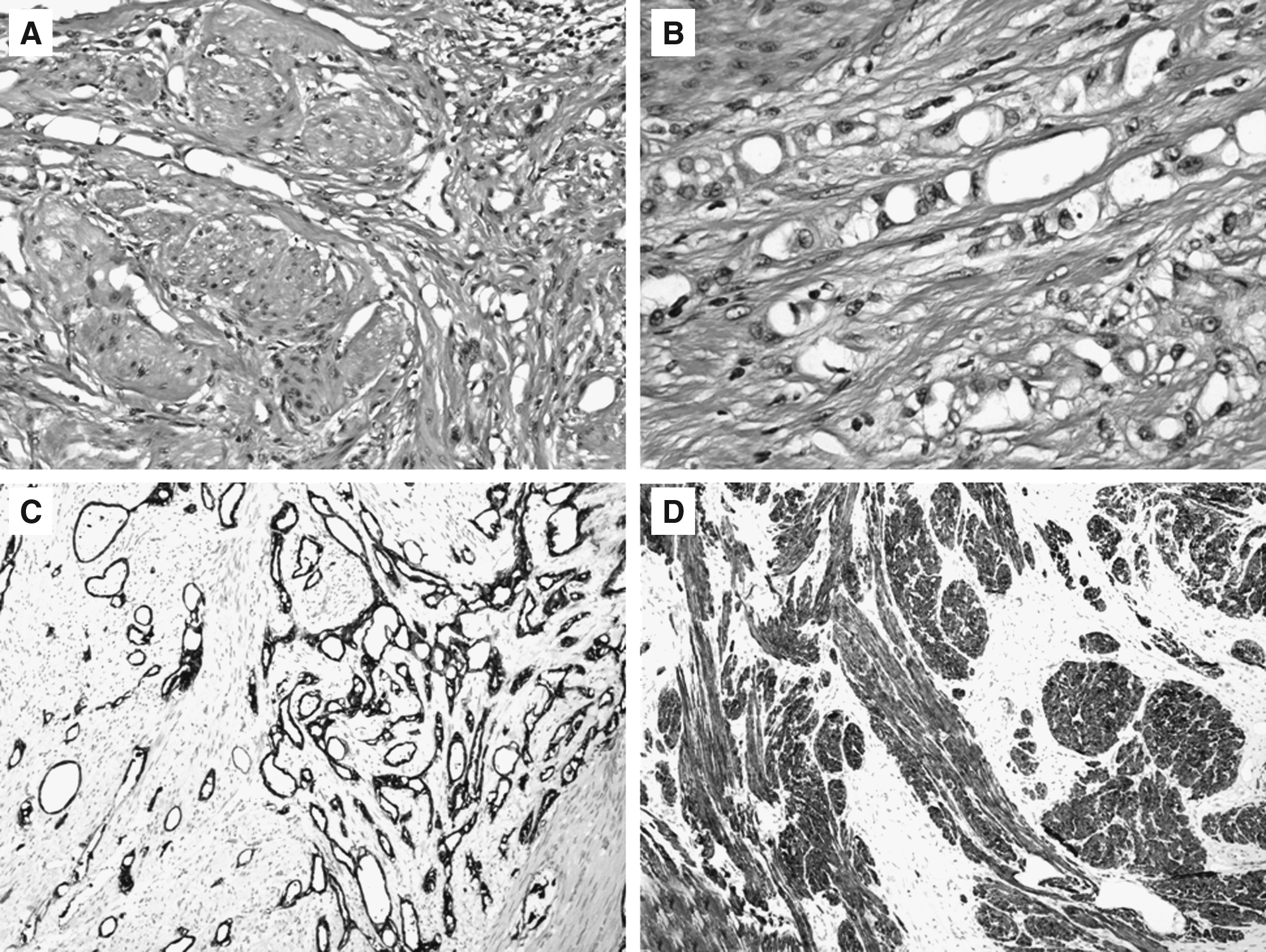
On microscopic examination the material showed uniform, fusiform smooth-muscle cells portrayed in a typical whorled pattern as in leiomyomas. Intermingled between the smooth-muscle fascicles. groups of vacuolated cells, slit-like structures, and tubules lined by flattened-to-cuboidal cells with small and uniform nuclei, some with an apical brush border, were observed. In some of the tubules and slitlike structures, very thin crossing strands were observed.
The adenomatoid-like tumor cells had positive immunostaining for the mesothelial antigen (HMBE-1), vimentin, calretinin, wide-spectrum cytokeratins (KL1) and low–molecular-weight cytokeratins (CK7 and CK8 LMW), and a negative reaction to endothelial antigens CD31 and CD34. The smooth-muscle cells had positive immunostaining for α-smooth-muscle actin and desmin. (Fig. 1). Immunohistochemical labeling for Ki-67 revealed a low proliferative index (<1%) in both the adenomatoid components and in the smooth-muscle tissue.
Results
The pathologic changes represented a leiomyo-adenomatoid tumor of the uterus. Postoperatively, her symptoms were resolved.
Discussion
Amérigo et al. discuss and favor the hypothesis that leiomyo-adenomatoid tumor should be considered a subtype of AT with distinctive morphologic features. The researchers base this on the presence of the adenomatoid component intermixed with the smooth-muscle proliferation and the fact that their case had a well-demarcated lesion as opposed to the previously reported cases of leiomyo-adenomatoid tumors. 1
In a collision tumor, which is the differential diagnosis for leiomyo-adenomatoid tumor, one would expect a transition from the leiomyo-adenomatoid component to an adenomatoid and a leiomyomatoid component, respectively. In the current case there was a balanced distribution of the adenomatoid component intermingled between the smooth-muscle cells throughout the entire tumor.
Conclusions
This case report is an additional contribution to support the hypothesis that leiomyo-adenomatoid tumor is a specific subtype of AT.
Disclosure Statement
No financial conflicts exist.