
Abstract
Abstract
Introduction
G
Case
A 16-year-old schoolgirl was referred to the gynecological clinic of the Woman's Health Center at Assiut University, in Assiut, Egypt, presented with a 4-month history of severe metrorrhagia with foul-smelling vaginal discharge and intermittent lower abdominal pain radiating to the lower back. She began menarche at age 12, and her menstrual flow was regular for 6 days with no menorrhagia or metrorrhagia. There was no history of urinary, gastrointestinal tract, or cardiorespiratory symptoms. She was misdiagnosed by ultrasound (US) as having an ovarian mass 1 month prior, she was counseled for abdominal exploration in another hospital, and she accepted. Abdominal exploration performed; however, this procedure revealed no pathology.
Her current clinical findings were pallor, fever (temperature of 38.6°C), and tachycardia. Her hemoglobin was 6 g/dL, and her urinalysis, blood chemistry, and liver function tests all yielded normal results. Her abdominal examination was normal. Pelvic examination revealed by inspection purulent vaginal discharge. Rectal US revealed a huge mass that was 10×5 cm filling the vagina. In view of this finding, vaginoscopic examination after written consent was necessary for the patient. The consent was provided and diagnostic vaginoscopy was performed under general anesthesia. A description of this procedure follows.
For a patient of this age, a parent accompanies the young patient into the operating theater until administration of anesthesia. Patients are positioned in a supine position with the thighs and knees flexed and the thighs abducted. A 3 mm-hysteroscope is used with a continuous normal saline flow. The hysteroscope is inserted gently through the vaginal orifice with one hand while the other hand is used to squeeze the vulval tissues gently around the hysteroscope to prevent fluid reflux. Care is taken to prevent damage to the hymen.
In this patient, this diagnostic procedure lasted <3 minutes. It confirmed the presence of a giant cervical polyp filling the whole cavity of the patient's vagina. The patient was counseled on the need for correction of anemia and subsequent surgery. Her anemia was corrected with five units of red blood cells. Broad-spectrum antibiotics were also administered. Abdominal exploration under general anesthesia through a Pfannenstiel incision revealed a normal uterus and adnexa. The bladder was dissected downward and the anterior vaginal wall was opened vertically. A giant, pedunculated cervical polyp, ∼ 10 cm, was confirmed. It originated from the entire anterior cervix (Fig. 1). An abdominal polypectomy was performed (Fig. 2). The patient's estimated blood loss was ∼ 300 mL. She was given 1 unit of whole blood intraoperatively. The anterior vaginal wall was sutured continuously with Vicryl No. 1 on a rounded needle (Fig. 3).
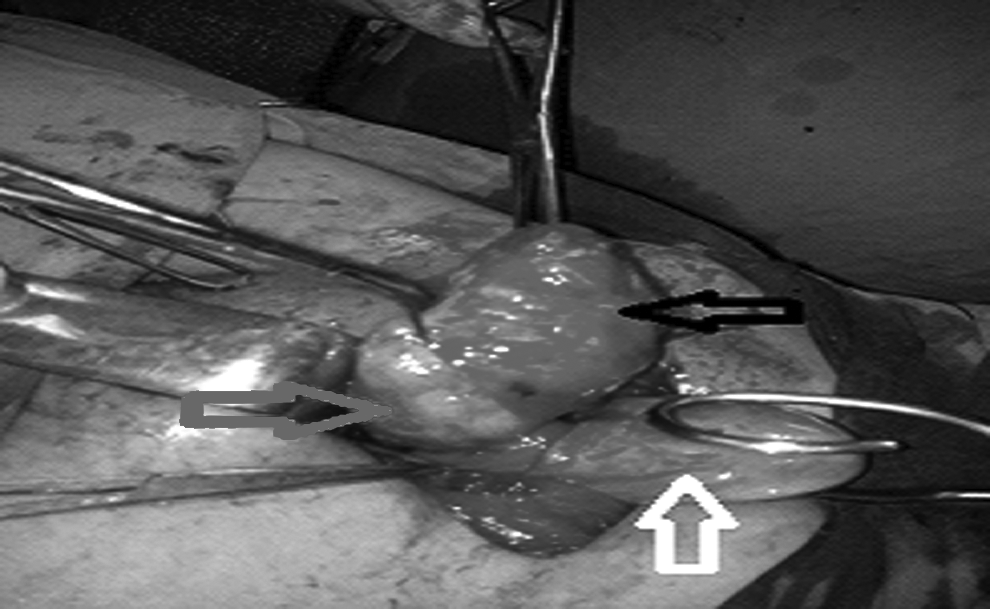
Normal-size uterus (white arrow), giant cervical polyp (black arrow), and opened anterior vaginal wall (gray arrow).

Giant cervical polyp after excision.
Suturing of anterior vaginal wall after polypectomy.
Results
The patient had an excellent postoperative course and was discharged on the fifth postoperative day with a hemoglobin level of 10 g/dL. Histopathologic examination of specimens revealed that she had a cervical fibroid polyp.
Discussion
A cervical polyp is a common benign polyp or tumor originating from the cervix. Cervical polyps constitute 4%–10% of all cervical lesions 5 ; these polyps are usually pedunculated, measuring between 2 mm and 30 mm. More than 60% of women presenting with cervical polyps are between ages 40 and 65, and 45% of these women are postmenopausal. 6 Ectocervical polyps are uncommon. Cervical polyps can reach a large size and protrude from the vulva, but giant polyps are rare. 7 Chronic cervicitis, foreign bodies, and unopposed estrogen secretion are the most common etiologic factors causing the development of cervical polyps. Polyps tend to be asymptomatic but may also present as abnormal bleeding, such as during intercourse, heavy menstrual periods, between menstrual periods, or after menopause. Occasionally, these polyps may grow large enough to obstruct the external os and cause infertility. 7 A giant cervical polyp may be associated with uterine prolapse, although this occurrence is rare, especially in menopausal women. Management of patients with cervical polyps may include different approaches, such as simple removal of the polyp, surgical dilatation and curettage, electrosurgical excision, hysteroscopic polypectomy, and, in few cases, abdominal exploration should be done to remove the polyp. Histologic examination of all cervical polyps is recommended because clinical assessment alone is not sufficient to exclude malignancy. The potential malignancy of giant cervical polyps is uncertain because of their rarity. 8
The gynecologic resectoscope is commonly used in gynecologic practice to resect or remove intracavitary pathology. A wire loop with a monopolar or bipolar resectoscope is most commonly hysteroscopic resection. Most gynecologists are familiar with this technique, and the equipment is cost-effective and widely available. As an adjunct to this technique, hysteroscopic scissors can be used to remove small pedunculated fibroid growths or fragments that remain attached to the uterine wall that are thus not easily removed with the loop. However, during use of a resectoscope, heavy perioperative bleeding may occur. An hysteroscopic morcellator (intra uterine morcellator) has a rotary blade for resection and suction to remove tissue fragments. 9 The disadvantage of hysteroscopic morcellators is that they cannot be used to cauterize bleeding vessels. The hysteroscopic morcellator is also not designed to reach deeper myomas.
There are many interesting points with respect to the case described in this article. First, to the current authors' knowledge, giant or huge cervical polyps are usually found in perimenopausal women; however, the current case involved a 16-year-old virgin. Second, the patient complained of severe metrorrhagia, and this was complicated by severe anemia. This was an interesting presentation a case that is commonly presented only by mild bleeding. Third, vaginal polypectomy is the treatment of choice for most cervical polyps; but in this case, the polypectomy was via abdominal approach because of the virginity of the patient. Fourth, histopathologic examination of specimens in this case revealed that the patient had a cervical fibroid polyp, which is rare in patients of such young age.
Conclusions
Although giant cervical fibroids are rare, this possibility should be considered, regardless of a patient's age. Proper evaluation is needed to make an accurate diagnosis. Vaginal polypectomy is the treatment of choice for most cervical polyps. Histologic examination for all cervical polyps is recommended to exclude malignancy.
Footnotes
Disclosure Statement
No competing financial conflicts exist.