
Abstract
Abstract
Introduction
P
Materials and Methods
Procedures
This study was performed from January 2007 to August 2010. The technique 11 and protocol of the study design was approved by the institutional ethical committee and informed consent was obtained from the patients before the intervention. The study involved 180 women who had POP (POP-Q stage 2 or higher) with or without coughing or a Valsalva maneuver. The patients were allocated into two groups following a computer-generated random number table. The surgical technique, as described by Hardiman and Drutz, 14 was followed. A double-ply, number 1 polyglactin-910 suture (Vicryl, J359H, Johnson & Johnson™) was used to fix the vault with the sacrospinous ligament in group 1 and a double ply, number 1, polydioxanone suture (PDS II, Z359T, Johnson & Johnson™) was used for group 2. All surgeries were performed by two senior gynecologists in both groups to exclude interobserver bias. The dissection to the ischial spine was done through an incision in the midline posterior vaginal wall, and the pararectal space was dissected bluntly to the lateral pelvic wall. Each suture was loaded in a Deschamps ligature carrier and passed 2 cm medial through the right sacrospinous liagment. Stitches were then passed through the vault, and closure of the colpoperineorrhaphy was performed. Finally, the fixation sutures were firmly tied without leaving any suture bridge.
The patients were followed-up after 1 month, 3 months, 12 months, and 24 months postoperatively (Fig. 1). During each follow-up visit, patients were asked if they had any urinary and bowel complaints, pain, or abnormal vaginal bleeding. Patients who did not attend the follow-up clinic visits for at least 24 months postoperatively were excluded from the study.

Study profile. PDS II is a type of suture. POP-Q, pelvic organ prolapse quantification, SSF, sacrospinous fixation; USG, ultrasound (gynecologic).
Outcome measures
The primary outcome measure was success rate (i.e., recurrence in the form of symptomatic or asymptomatic prolapse stage 2 or more [leading part of the prolapse is ≥−1cm to the level of the hymen) in the middle compartment (Point C/distal edge of the cervix or vaginal cuff/apex in cases of hysterectomy] and/or need for reoperation within 2 years of follow-up. Each patient's clinical parameters were evaluated during each postoperative check-up.
Secondary outcome measures were immediate and late complications, hospital stays, postoperative recovery, subjective outcome, and improvement in general and disease-specific QoL.
Statistical analysis
Sample size was calculated for the primary outcome measure (i.e., the success rate of the procedure). A minimum of 90 subjects in each group was calculated, assuming a power of 0.8 (β=80% and α=0.05) at a 95% significance level (p-value 0.05), to detect a difference of 15% in the success rate between the two groups, assuming at least an average success rate of 80%8–10 and a dropout rate of 15%.
Characteristics of the patients were summarized, using descriptive statistics for continuous variables (mean, median, and standard deviation as appropriate) and compared using Student's t-tests. Categorical data were summarized as count and in-frequency distribution and evaluated using McNemar's exact test. Data were analyzed using the statistical package Epi Info Statcalc, version 6 (Centers for Disease Control and Prevention, Atlanta, GA). The p-value was established at ≤0.05 as statistically significant.
Results
Ten cases in group 1 and 8 cases in group 2 were excluded from the study, as these subjects did not return for follow-up during the stipulated time period of 24 months (Figs. 1 and 2). Both the groups were comparable in terms of demographic and preoperative variables (Table 1). Seventy-three women in group 1 and 70 in group 2 were postmenopausal. Seven cases in group 1 and 8 cases in group 2 (including a total of 11 cases of symptomatic vault prolapse to or beyond the hymenal level) had prior histories of surgery (abdominal/vaginal hysterectomy with/without repair of pelvic floor; Table 1).
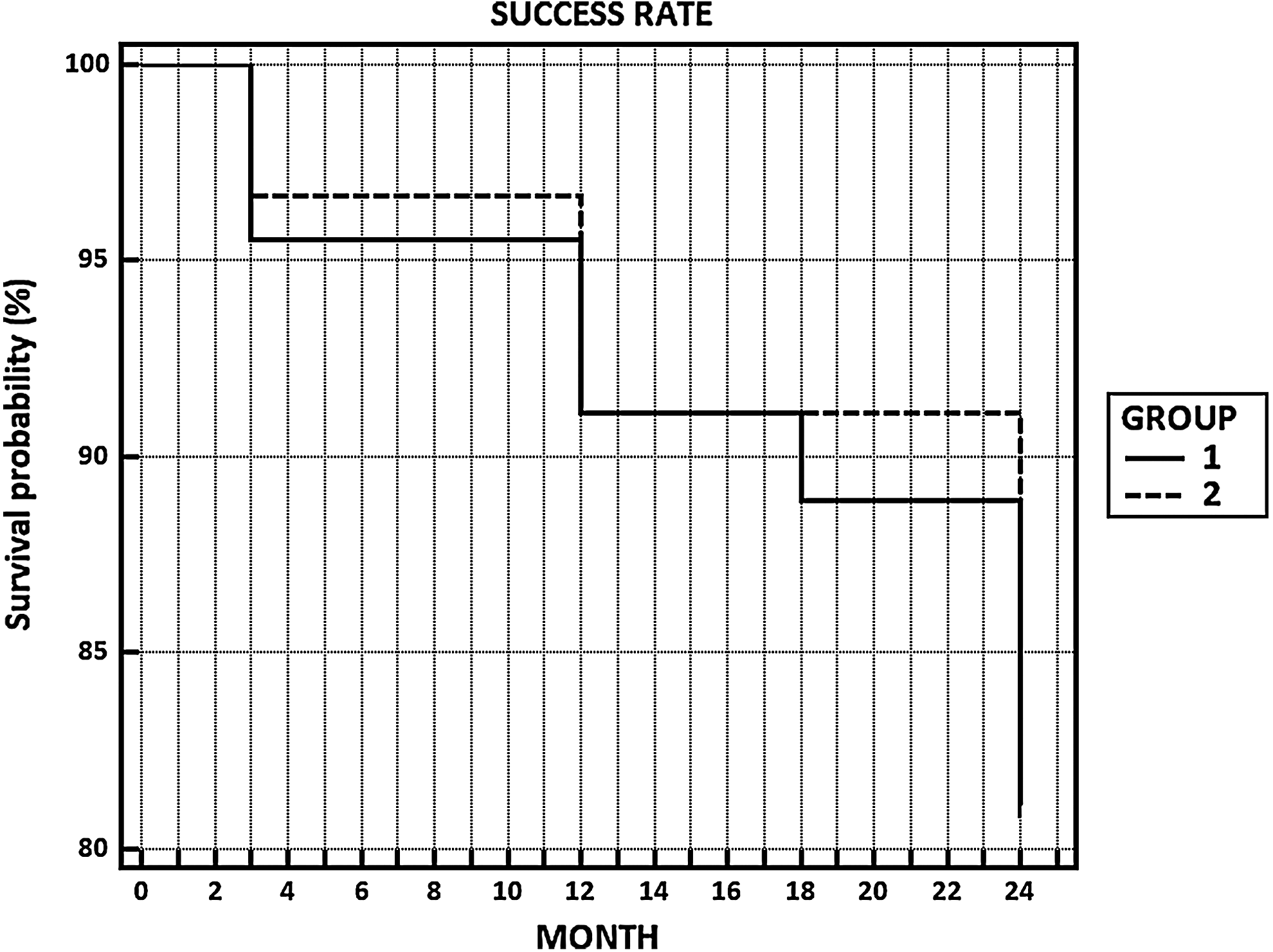
Time-dependent survival probability for Group 1 and Group 2 in terms of success rate.
BMI, body mass index; SD, standard deviation; TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; VH, vaginal hysterectomy; PFR, pelvic-floor repair.
Blood loss was proportional to the duration and nature of surgery, and there was no significant difference the groups (Table 2). The majority (87.5% in group 1 versus 86.5% in group 2) of the patients underwent vaginal hysterectomy, anterior colporrhaphy, and posterior colpoperineorrhaphy along with SSF. SSF was combined with anterior and posterior repair in 5 cases in both groups, as the patients were young and did not opt for hysterectomy.
SSF, sacrospinous fixation; VH, vaginal hysterectomy; AC, anterior colporrhaphy; PC, posterior colpoperineorrhaphy; CI, confidence interval; min, minutes, SD, standard deviation.
The perioperative complication (Table 3) most commonly encountered was hemorrhage (7.5% of group 1 versus 6.09% of group 2), which was managed by blood transfusion and pressure packing of the vagina immediately after the operation in the patients in both groups. Mild-to-moderate gluteal pain (5% versus 3.65%) responded well to analgesics for 3–7 days and resolved within 3 months. Persistent gluteal pain for more than a year was encountered in 3 cases in group 2 and in 1 case in group 1. Sutures were not detectable at this stage of follow-up. Persistent vaginal bleeding was noted in a total of 9 cases (5% in group 1 versus 6.09% in group 2). In 5 cases, granulation tissue had to be managed with silver-nitrate application. Others resolved spontaneously over time. Five patients in group 1 and 4 patients in group 2 developed postoperative cystocoeles (grade 2), which were mostly asymptomatic. The incidence of enterocoele was 2 in each group. Recurrence either in the anterior or posterior compartment did not require reoperation within the follow-up period. Postoperative urinary complaints of either stress or urge incontinence were comparable in both groups.
BT, blood transfusion; CI, confidence interval.
The length of postoperative follow-up was at least 24 months. There was significant improvement of general and disease-specific QoL in 93.75% (77/80 in group 1 versus 75/82 in group 2) of the subjects. Five patients were not satisfied at the end of stipulated follow-up period (2 years)—2 because of persistent gluteal pain and the other 3 because of menopausal symptoms unrelated to the surgery—although the anatomical outcome was satisfactory in both cases (Fig. 2). The success rate in group 1 was 91.25% and was 92.68% in group 2.
Although 18 cases were excluded from this study, it is worth mentioning that, among these cases, 9 patients were followed for 12 months, 7 patients for 3 months, and the rest of the patients for 18 months. Almost all of these patients were symptom-free; 1 patient had urge incontinence at 3 months and the other had a grade 1 cystocoele at 12 months.
Discussion
As women live longer and healthier lives, pelvic-floor disorder continues as an important health and social issue. Management of pelvic-organ prolapse can be difficult because of the coexistence of different support defects. Various types of surgical approaches have been studied to address this bothersome condition. Although the true incidence of vault prolapse is unknown, some literature has estimated its incidence as 0.2%–1.0%.
9
Nichols
15
studied sacrospinous fixation for vault support in the late 1980s and found it to be an excellent procedure without jeopardizing vaginal length. Subsequently, SSF was used as a procedure for vaginal-vault prolapse only.
10
Cruikshank and Cox
16
stated that this procedure can also be used as a prophylaxis against posthysterectomy vault prolapse, especially in patients having loss of uterosacral–cardinal ligament complex noted at the time of hysterectomy. However Colombo and Milani
17
did not recommend this procedure as a prophylactic measure with vaginal hysterectomy for prevention of vault prolapse, owing to increased blood loss in an SSF group. Compared to some other studies,2,18,19 average blood loss was higher owing to the fact that vaginal hysterectomy was done in the majority (85.41%) of the cases along with pelvic-floor repair, requiring longer operative time. Injury to the vessels may occur from overzealous dissection or passage of a needle through the neurovascular bundle in the sacrospinous ligament. Pressure may work well for control of this type of hemorrhage.
20
Most of the intraoperative bleeding in the current study was managed by pressure packing. In the current study, the incidence of hemorrhage requiring blood transfusion was comparable to other studies.2,19 SSF has been used over the years as an effective method for suspension of the vaginal vault, a but paucity of data exists regarding the ideal suture material for this widely practiced procedure. Historically, various types of sutures (permanent or delayed absorbable) have been used for this procedure (e.g., nylon, prolene, silk, polydiaxanone, or TiCron
Concern regarding a higher incidence of postoperative cystocoele caused by damage of the pudendal nerve has been reported in some studies. 18 Some researchers argue in favor of iliococcygeus fixation, showing a higher success rate and a lower incidence of cystocoele formation.27,28 However, iliococcygeus fixation might contribute to stress in the anterior vaginal wall, as it this procedure is usually performed bilaterally. SSF has a comparable success rate to iliococcygeus suspension, but patients' satisfaction is higher after SSF. 18 According to Morgan et al., failure rates after SSF are, in part, accounted for by differences in how anatomical outcomes are evaluated and which compartment of vaginal support is being considered. 5 Failure rate after SSF is highest in the anterior compartment. 5 Nine cases of asymptomatic cystocoele (5 in group 1 versus 4 in group 2) were recorded in the current study, which is comparable to the studies related to iliococcygeus fixation.27,28 A study by Smilen et al. 29 concluded that SSF did not increase the risk of postoperative cystocoele formation independently, compared with other vaginal reconstructive procedures performed without SSF. In addition, in the current study, 4 cases of enterocoeles were detected during follow-up.
Severe postoperative gluteal pain that runs down the posterior surface of the right thigh may result from pudendal-nerve injury or entrapment. Some researchers suggest that muscular ischemia contributes to this type of buttock pain. 18 In the current study, in patients presenting with late-onset vaginal bleeding, granulation tissue was found in 8 (3 in group1 versus 5 in group2). Immediate removal of the suture has been suggested by several researchers who did studies in which where permanent sutures were used.11,21 Sutures were not visible at this stage of follow-up, and 5 cases resolved with application of silver nitrate. Patients may have transient, moderate-to-severe buttock pain on the side of the sacrospinous ligament suspension (10%–15%). 20 This is usually self-limiting and resolves within 2–3 months postoperatively as was also noted in the current study. Although there were 4 cases (1 in group 1 versus 3 in group 2) of persistent gluteal pain, this was not related to pudendal-nerve entrapment, thus, neither kinds of suture had to be removed. Complications such as ureteral entrapment23,30 have also been reported in some studies but this was not seen in the current study's series.
Restoration of the vaginal apex remains the primary goal of this surgery. SSF is used to suspend the vagina to the sacrospinous ligament and brings the upper vagina over the levator plate. This procedure is generally done unilaterally, although bilateral performance of it has been described. The right sacrospinous ligament is commonly chosen, based on the hand dominance of the surgeon. 20 The overall results from sacrospinous ligament fixation has been good. Sze and Karman reviewed 1137 patients with 83% cure rate. 31 In the current study, the cure rate in group 1 was 90% and was 91.89% in group 2.
Abdominal sacrocolpopexy can be performed as an alternative to SSF. The former procedure is associated with a better long-term result (a lower rate of recurrent vault prolapse and dyspareunia) but requires longer a hospital stay with potentially more postoperative morbidity and a longer learning curve for the surgeon, compared to SSF.11,32 The trend toward a lower reoperation rate for prolapse following abdominal sacrocolpopexy was not statistically significant, compared to vaginal SSF. 11 However, vaginal SSF is quicker and less expensive to perform and provides patients with earlier return to daily activities. 11
Conclusions
Various surgical techniques have been used to suspend the vaginal vault. The experience—and, consequently, the bias of surgeons—have historically dictated the approaches and the types of suture material used during surgery. Techniques and approaches for SSF has changed over time, a but paucity of data exists regarding which suture material will yield a lower rate of complications. The current authors suggest that absorbable sutures, such as polyglactin 910 or PDS II, have comparable success profiles and fewer complications.
Footnotes
Disclosure Statement
The authors report no conflict of interest. The authors alone are responsible for the content and writing of this article.