
Abstract
Abstract
Introduction

Bicornuate uterus with noncommunicating horn. (Credit to Benson T. Congenital Anomalies of the Female Genital Tract: Atlas of Female Pelvic Medicine and Reconstructive Surgery, 2nd ed. Philadelphia: Springer, 2009.)
Pregnancy in a rudimentary horn of the uterus is a very rare condition (∼1/100,000). 4 Serious maternal morbidity as well as fetal death have been reported for patients with this condition. Miscarriage, ectopic pregnancy, rudimentary horn uterine rupture, preterm labor, malpresentation, and placenta accreta are among the complications. 5 However, there are numerous cases of full-term birth reported of pregnancy in a rudimentary horn.6,7
In a literature review by Nahum, newborn survival range was from 0% to 13%, which increased over time, compared with prior decades. Fifty percent of pregnant uterine horns ruptured, and the majority of these events (80%) occurred prior to reaching to third trimester. Maternal mortality has decreased significantly, compared with decades ago, when diagnostic imaging was not available. 8
Case
A 20-year-old gravida 2, para 1001, female presented to the emergency department complaining of mild periumbilical pain. She denied having any vaginal bleeding. Her past medical history was significant for a prior full-term uncomplicated vaginal delivery. She reported being ∼7 weeks pregnant, according to the date of her last menstrual period. The emergency department personnel performed a bedside ultrasound to confirm the pregnancy. An intrauterine gestation was not identified. Her β–human chorionic gonadotropin (βhCG) level was 92,927 milli-international units (mlU)/mL. Transvaginal ultrasound showed a uterus with a thickened endometrium and no evidence of an intrauterine pregnancy. The adnexa and ovaries on both sides were visualized. Adjacent to the right ovary, a large gestational sac containing a yolk sac and a fetal pole with a fetal heartbeat was noted. The size of this mass was 3 cm, and a pregnancy at 7 weeks by crown rump length (CRL) of gestation was confirmed. The patient was taken to the operating room for a diagnostic laparoscopy with the presumptive diagnosis of ectopic pregnancy. Intraoperatively, a bicornuate uterus with a right rudimentary horn was noted (Figs. 2 and 3). There was no evidence of ectopic or abdominal pregnancy.

Pregnancy in a rudimentary uterine horn seen during laparoscopy.
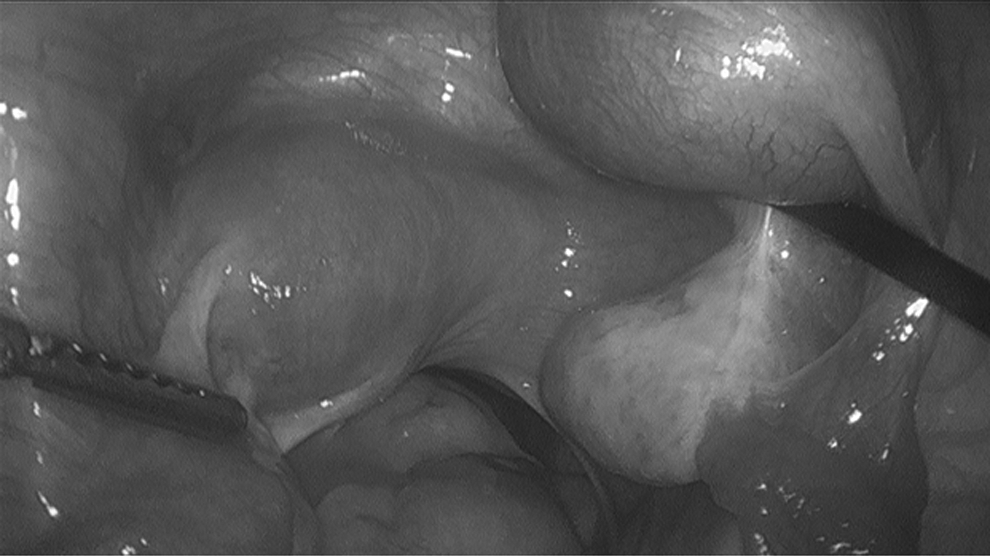
Pregnancy in a rudimentary uterine horn and its relationship to the right ovary and Fallopian tube.
Upon examination, one normal-appearing cervix was noted. This was a desired pregnancy, and as there was potential for growth of the pregnancy to term, after discussion with the maternal fetal medicine (MFM) department, the decision was made to terminate the procedure and maintain the pregnancy. Postoperatively, patient was informed regarding the findings, and the risks associated with pregnancy in the rudimentary horn of the uterus were discussed with her. After extensive counseling, she indicated that desired to continue the pregnancy.
The patient was followed with serial ultrasounds, and continued to have prenatal care with the MFM Group. Ultrasound confirmed adequate growth of a male infant with normal anatomy (Figs. 4, 5, and 6).

Ultrasound at 7 weeks.

Ultrasound at 13 weeks.

Ultrasound at 18 weeks.
The pregnancy proceeded without complication until ∼22 weeks of gestation. At 22 weeks and 1 day of gestation, the patient presented with abdominal pain. She had benign results from an abdominal examination. Speculum and bimanual examination results were unremarkable. Fetal heart tones were confirmed with a bedside ultrasound. The patient was discharged to go home after a few hours of observation.
The patient again presented to the hospital 2 days later with worsening abdominal pain. Her vital signs were stable. Her abdomen was now significantly tender, with diffuse rebound tenderness. The cervix was closed. She was hemodynamically stable. Complete blood count testing revealed a leukocytosis (16,500/mm3) and a hemoglobin of 11.5 g/dL. Bedside ultrasound did not show any fetal or placental abnormalities. Because of the patient's worsening of symptoms and the history of the Müllerian anomaly, an abdominal magnetic resonance imaging (MRI) scan was performed, as there was no clear explanation for her abdominal symptoms and thus possible rupture of the rudimentary horn was of concern to her care providers. The MRI showed a gestational sac containing a fetus to the right of the uterus, with no definite connection identified between the endometrial cavity or cervix and the gestational sac (Figs. 7 and 8).
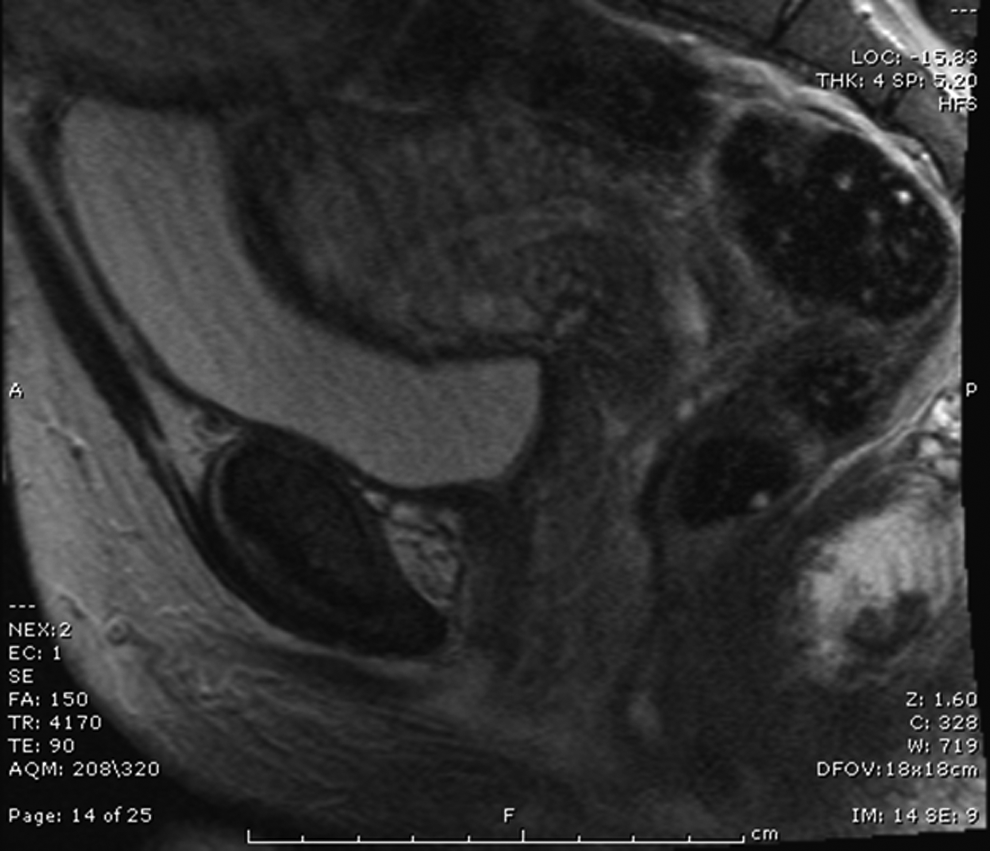
Magnetic resonance imaging at 22 weeks +3 days.
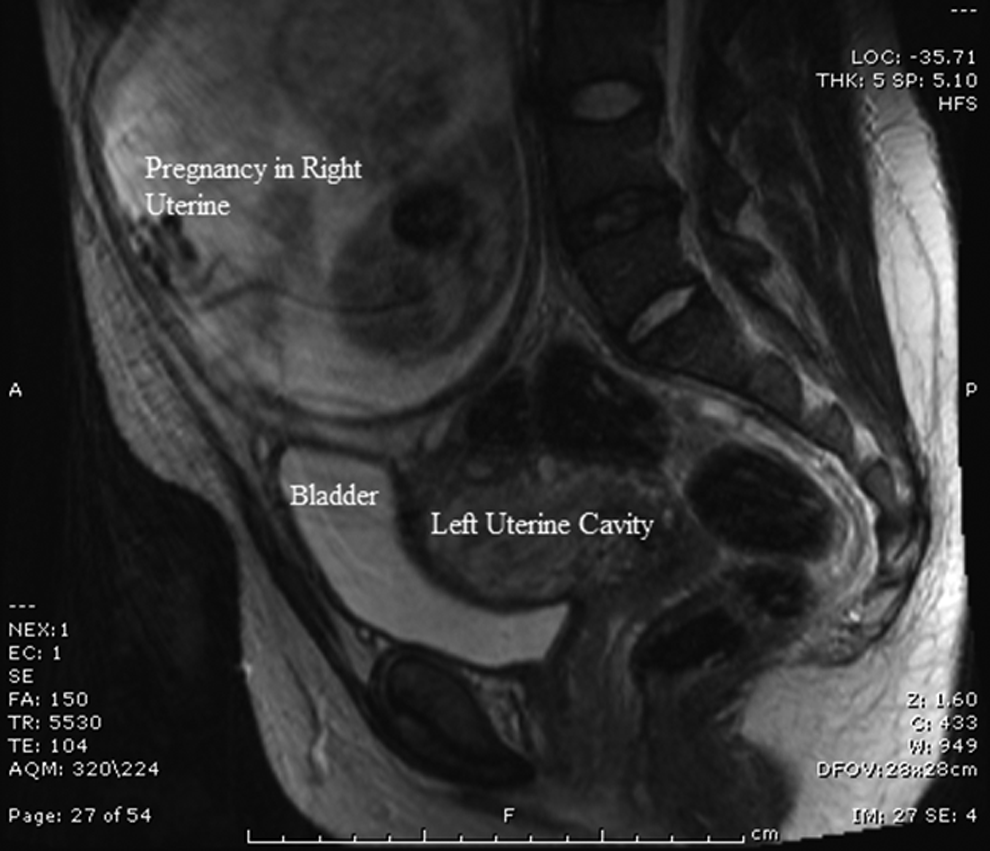
Magnetic resonance imaging at 22 weeks +3 days, showing the pregnancy in the rudimentary horn of the uterus.
As the pregnancy was close to viability, the MFM and the neonatology departments were consulted. After a thorough discussion with the patient, the decision was made to proceed with exploratory laparotomy and removal of the pregnancy. A decision was made not to perform resuscitation of the fetus after delivery. With the patient under general anesthesia, a vertical abdominal incision was made. Upon entry to the abdominal cavity, hematoperitoneum (100 cc) was noted. An intact gestational sac completely occupied the right side of the pelvis. A normal-size uterus and left adnexa were displaced to the left. The gestational sac was attached to the left uterine horn through the broad ligament. The round ligament, ovary, and tube were to the right side of the gestational sac and laterally displaced by the enlarged mass. The right uterine horn, with an intact gestational sac, and the right tube and ovary were removed and sent to the pathology department (Figs. 9 and 10). It was not possible to save the ovary, because of the severe displacement by the mass. The blood loss from the procedure was minimal.
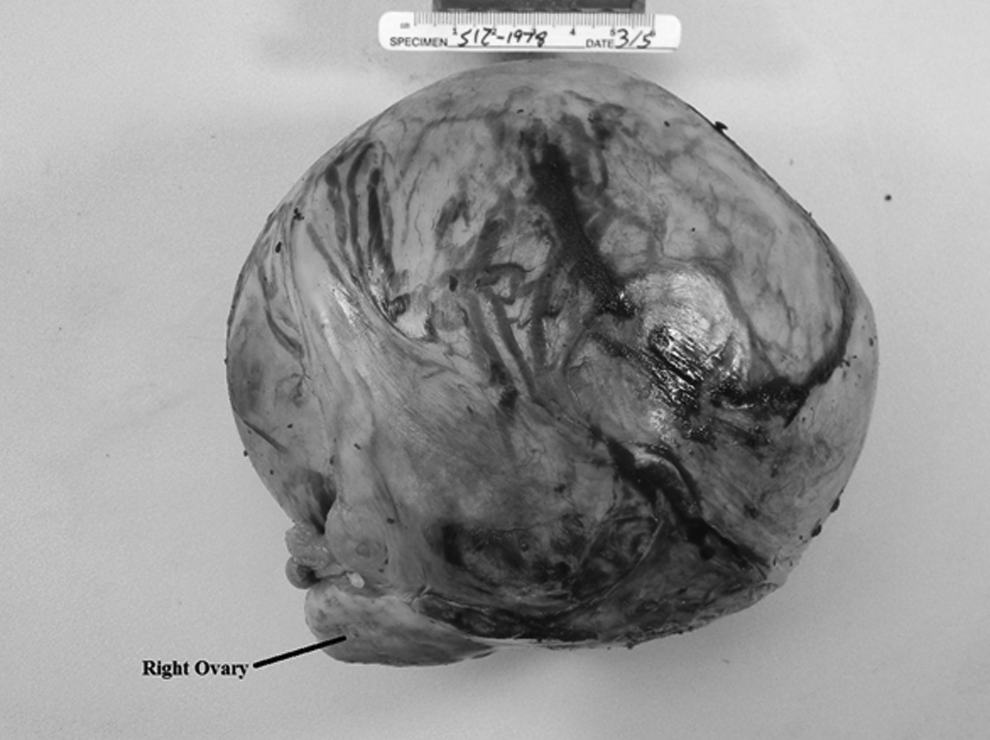
Gestational sac with attached ovary and tube (line to the right ovary).

Gestational sac with 22-weeks +3-day-old fetus.
Results
The patient's postoperative course was uneventful and she was discharged to go home home on postoperative day 3.
The excised mass contained a 22-week-and-3-day-old fetus weighing 430 g. Smooth muscle was identified surrounding the gestational sac (Fig. 11).

Cross-section of rudimentary horn wall containing the gestational sac.
Discussion
The diagnosis and management of rudimentary horn pregnancy remains controversial. Extensive maternal counseling is essential prior to electing to continue the pregnancy. Careful monitoring is required, as pregnancies in the rudimentary horn of the uterus may not grow adequately. The rudimentary horn may not provide the muscular and vascular support required to maintain a pregnancy. In this case, ultrasound was helpful but not definite in the initial diagnosis. An MRI may be beneficial in management of these pregnancies.
Conclusions
When rudimentary horn pregnancy mimics ectopic pregnancy, surgical intervention is mandatory. Conservation of the unilateral ovary is desirable, but excision of the tube and horn should be considered to prevent recurrences.
Footnotes
Disclosure Statement
No competing financial interests exist.