
Abstract
Abstract
Introduction
T
Cases
Case 1
A 26-year-old primigravida was referred to Fernandez Hospital in the 12th week of gestation, with suspicion of abdominal pregnancy, during a routine nuchal translucency scan. She was hemodynamically stable, and a nontender suprapubic mass was palpable. There was a single cervix, and her uterus appeared to be enlarged to 14 weeks' size on bimanual examination. Ultrasound evaluation revealed an empty uterus and an extrauterine gestational sac measuring 73×65 mm, with a live fetus of crown rump length (CRL) 51 mm superomedial to the right ovary, suggestive of ectopic pregnancy in the Fallopian tube or rudimentary uterine horn. Both ovaries appeared normal, and there was no free fluid in the pelvis. There were no associated renal anomalies. At laparoscopy, there was a left unicornuate uterus with an unruptured gravid right rudimentary horn measuring 120×80×80 mm. Both ovaries and tubes were normal; the right tube and round ligament were found to be attached to the rudimentary horn (Fig. 1). A harmonic scalpel was used to divide the broad band between the uterus and rudimentary horn. The horn was excised, ipsilateral salpingectomy performed, and tissues were retrieved in an endobag after mechanical morcellation through an enlarged 10 mm left lateral port. The estimated blood loss was 200 mL, and the duration of the surgery was 180 minutes. Histopathologic examination revealed products of conception in the rudimentary horn. The fetus measured 90 mm in length, with well-formed limbs and eyes. There was no other significant pathology.
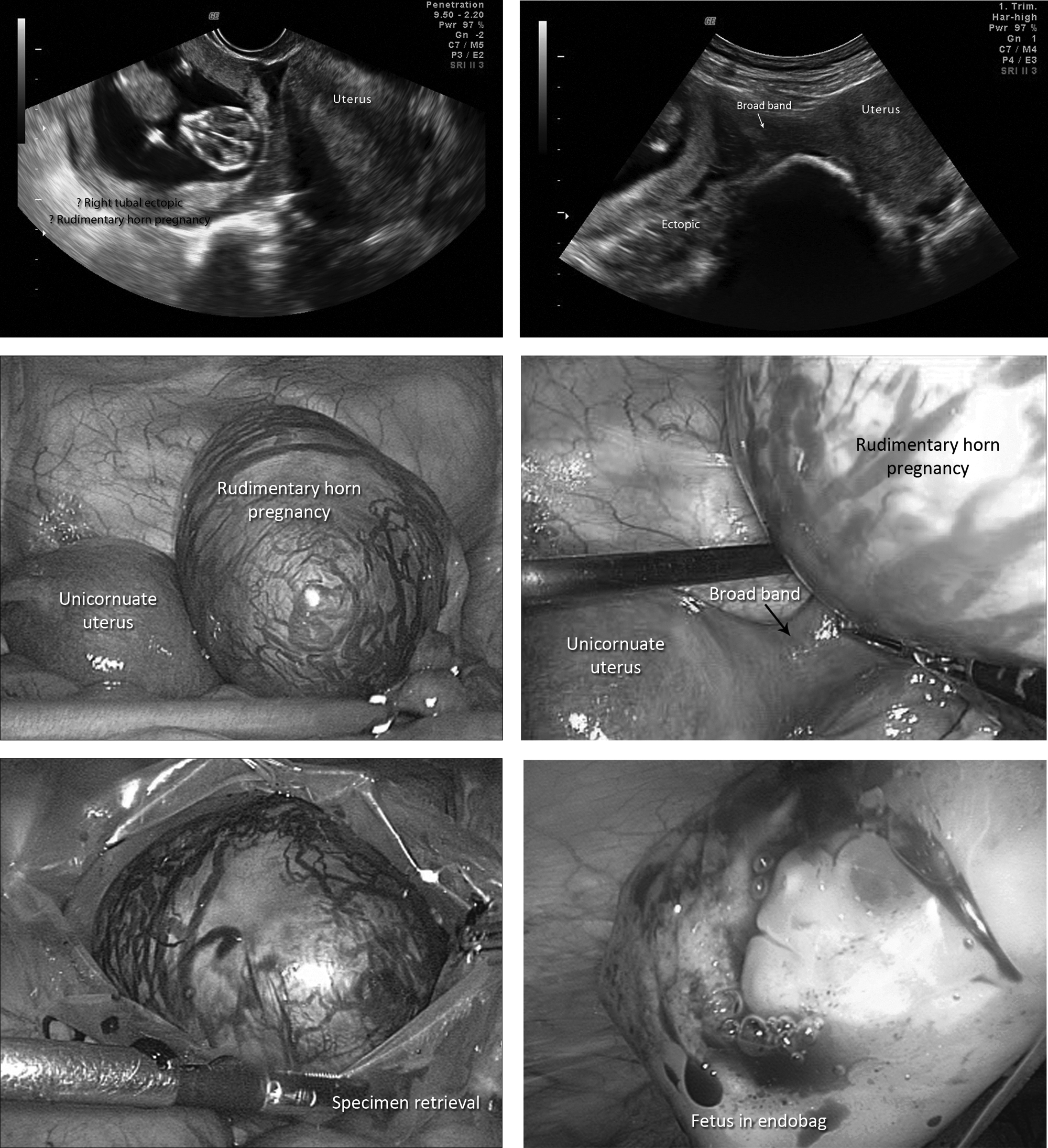
Ultrasound and laparoscopic images of left unicornuate uterus with an unruptured gravid right rudimentary horn.
Case 2
A 30-year-old fifth gravida with 1 living issue presented at 7 weeks of gestation with amenorrhea with lower abdominal pain. She had had three consecutive ectopic pregnancies in the right tube in the past, two of which had been treated conservatively. The third pregnancy, after laparoscopic right tuboplasty, resulted in a ruptured right ectopic pregnancy, which was managed by laparotomy. At the time of presentation, there was no pallor and vital signs were stable. Ultrasound revealed a gestational sac measuring 19×18 mm in the right cornual region, with a live fetus with CRL of 5 mm. Myometrial thickness around the sac was 4 mm, and there was no free fluid in the pelvis. Serum beta human chorionic gonadotropin (βhCG) was 28,038 milli-international units (mIU/mL). The patient was admitted for emergency laparoscopy. Small bowel and omentum were densely adherent to the anterior abdominal wall. Adhesiolysis was performed, and the patient was found to have a highly vascular 30×30 mm right interstitial pregnancy. The lateral one third of the right tube was intact, suggesting that segmental resection had been performed previously (Fig. 2). Vasopressin was infiltrated (20 U in 100 mL) at the base of the interstitial pregnancy, and a circumferential incision was made over the right cornua. The products of conception were removed, and endosuturing was performed with 1-0 Vicryl interrupted sutures. A right salpingectomy was performed, and the tissue was retrieved through a 10 mm port. The procedure-related blood loss was <50 mL. The surgery was completed in 150 minutes. Serum βhCG on the 1st postoperative day was 10,857 mIU/mL, which dropped to 194 mIU/mL 1 week later, and hence adjuvant methotrexate was not given. Histopathologic features were consistent with tubal gestation, and there was no evidence of gestational trophoblastic disease. The patient was advised to use contraception for 1 year and to plan an elective cesarean delivery at term for the next pregnancy.

Ultrasound and laparoscopic images of right interstitial pregnancy.
Results
The postoperative period was uneventful for both patients. The first patient had regular follow-up for 3 months. The second patient was lost to follow-up.
Discussion
Müllerian anomalies occur in 4.3% of the general population, with unicornuate uteri accounting for 0.4%. 2 The incidence of rudimentary horn pregnancy (RHP) ranges from 1:760003,4 to 1:140000. 5 The left Müllerian duct advances slightly ahead of the right duct, which may account for the predominance of right-sided rudimentary horns.3,6,7 The proportion of noncommunicating horns ranges from 70% to 90%.3,7 The attachment of the rudimentary horn to the main uterus varies from a fibromuscular band, as in case 1, to an extensive fusion between the two where there is no external separation between them. 8
Complications of rudimentary horns include hematometra with dysmenorrhea, endometriosis, and pregnancy in the rudimentary horn.3,7 Women with rudimentary horns may also have associated renal anomalies. 3 Because the horn is noncommunicating, fertilization and implantation are thought to take place by transperitoneal migration of sperm or the conceptus.3,4 Outcomes of pregnancy are poor, with an increased risk of miscarriage, ectopic pregnancy, preterm labor, and malpresentation. Intrauterine growth restriction and intrauterine fetal death are presumed to be secondary to the poor vasculature of the horn, and placenta accrete is presumed to be secondary to the poorly formed endometrium.3,7 The most significant threat of pregnancy in a rudimentary horn is the risk of rupture, because of the poorly developed musculature. Most of these rupture in the second trimester and result in catastrophic hemorrhage. In 588 cases of RHP from 1990 to 1999, rupture was noted in 50%. 3 The maternal mortality rate is reportedly<0.5%.3,7
Diagnosis of RHP requires a high index of suspicion in nonresponders to pregnancy termination. 9 The criteria for diagnosis are: pseudopattern of an asymmetrical bicornuate uterus, absent visual continuity between the cervical canal and the lumen of the pregnant horn, and the presence of myometrial tissue surrounding the gestational sac. Hypervascularization and abnormal placentation leading to placenta accreta have also been described. 10 Magnetic resonance imaging (MRI) is a useful tool for diagnosing RHP using coronal, sagittal, and axial planes to assess the uterine connection to the horn, and to either confirm or rule out a cavitary communication. One case of RHP resulting in a live birth was diagnosed at cesarean delivery. It had initially been mistakenly diagnosed as pregnancy in a bicornuate uterus. 11 It is plausible that diagnosis may have been similarly missed, and pregnancy allowed to continue, in other cases that resulted in live births.
Recommended treatment of RHP once diagnosed is termination of pregnancy. Traditionally, management of RHP has been by laparotomy and excision of the gravid horn. Ipsilateral salpingectomy is mandatory to prevent future tubal pregnancy. At present, endoscopy is accepted as the standard treatment for unruptured cases and in hemodynamically stable ruptured cases. Sevtap described successful medical management by intrasac instillation of methotrexate. 5 Eleven cases of RHP managed by laparoscopy were reviewed by Kadan and Romano. 12 Coagulation was used to excise the fibrous band, and the gravid horn was removed in an endobag through an 11–15-mm incision. There was only one case reported in this series at 13 weeks of gestation, in which the rudimentary horn was excised through the vagina after aspiration of the contents of the horn. 13 In some cases, medical treatment was administered prior to or during laparoscopy to reduce the pregnant horn size and intraoperative bleeding. With the use of ultrasound, the diagnosis can be made before symptoms occur, and hence most of the cases are diagnosed in the first trimester during routine ultrasound. Early diagnosis makes laparoscopic excision feasible and safe. Although there are options of medical treatment and expectant management in nonviable pregnancies, laparoscopic excision is more promising and offers complete and definitive treatment, considering the challenging situation and potential complications of RHP. Nahum 7 proposed an attitude of guarded optimism; however, there appears to be insufficient evidence, at least at present, to recommend an expectant management when the diagnosis of an RHP is made antenatally. 3
The ectopic gestation in case 2 was an interstitial pregnancy. The incidence of interstitial pregnancies is 16 per 1000 pregnancies, and they account for 2%–4% of all ectopic pregnancies. 1 A previous ipsilateral salpingectomy is a risk factor unique to this condition. The cornual area is well supplied by the Sampson artery, which is connected to both the uterine and ovarian arteries. Unruptured interstitial pregnancy is typically characterized by an asymmetric bulge in the upper corner of the uterus. The surrounding myometrial tissue allows for development of the pregnancy into the second trimester. Consequently, this type of pregnancy may rupture later, and this rupture of the uterus results in even more devastating hemorrhage than tubal rupture. Hemorrhagic shock may be found in 25% of the patients, and the associated mortality rate can be as high as 2%–2.5%. 14
Ultrasound criteria for the diagnosis include an empty uterine cavity, a gestational sac separate from the cavity and >1 cm from the lateral most edge of the cavity, and a thin myometrium of<5 mm around the sac. When compared with the surgical/pathologic diagnosis, application of these criteria yielded 90% specificity, but only 40% sensitivity. The interstitial line is an echogenic line abutting the gestational sac extending from the endometrial cavity to the cornua, which represents the interstitial portion of the Fallopian tube. 15
Management of this condition has always been a great challenge, because it remains one of the most difficult gestations to diagnose and treat. 1 Methotrexate in single or multiple doses administered systemically or locally at the ectopic gestation is a useful option. Although surgery is averted and tubal and cornual integrity are apparently preserved, an overall failure rate of up to 35% has been reported. 16 The traditional surgical approach has been laparotomy with either cornual wedge resection or hysterectomy. With advances in laparoscopic equipment and surgical skill, laparoscopic management is now considered a safe and effective alternative. Cornuostomy can be performed if the size of the cornual ectopic is<30 mm, to preserve anatomic integrity as much as possible. Cornual wedge resection is proposed when the size is >30 mm, to ensure complete removal of ectopic pregnancy. 17 After conservative surgery, monitoring of serum βhCG levels is indicated to detect the development of persistent ectopic pregnancy, because of the presence of deeply embedded surviving trophoblastic tissue. Methotrexate need not be routinely given postoperatively, and should be reserved for the few patients in whom the hCG concentration does not decrease by 15% within 48 hours. 17
The vascularity of the interstitial region may result in substantial blood loss, at times necessitating hysterectomy. Techniques to minimize blood loss include vasopressin (1:100 or 1:200) infiltration into the base of the cornual pregnancy, tourniquet application (Vicryl 2-0) all around the cornual pregnancy before excision, and selective ipsilateral devascularization by coagulating the ascending uterine artery.18,19 Novel techniques using a laparoscopic stapling device and suture loop have been described by expert laparoscopists, even in cases with a cornual rupture. 20 Ross et al. successfully managed two cases by dilatation and evacuation under ultrasound guidance, leaving the placenta in situ and administering postoperative methotrexate. 21 Laparoscopic and ultrasound-guided vaginal evacuation 22 and hysteroscopic suction 23 have also been reported. In the combined hysteroscopic and laparoscopic approach, concomitant laparoscopy not only guards against cornual rupture during hysteroscopic resection, but also enables diagnosis of certain cases of placenta percreta. 17
Whether or not to perform a concomitant ipsilateral salpingectomy is a matter of contention. Although salpingectomy prevents the occurrence of a tubal ectopic in the future, it does not prevent recurrence of ectopic pregnancies at other sites. Siow and Ng argue that the tube may be left behind for future cornuotubal anastomosis. 17 Ipsilateral salpingectomy was performed in case 2, as this was the fourth recurrence in the same tube. The implications of ipsilateral salpingectomy, including the need for in vitro fertilization treatment, should the contralateral tube be diseased or removed in the future, must be discussed with the patient. Delivery in subsequent pregnancies is usually by an elective cesarean delivery, to avoid the risk of uterine rupture during labor.1,21 Recurrent cornual ectopic pregnancies have been reported in 9.4% of cases. Using a low-voltage cutting current (30 W) for cornuostomy and wedge resection, and limiting the use of diathermy to achieve hemostasis, can prevent cornual dehiscence or rupture in future pregnancies. 17
Although the incidence of these varieties of “cornual” pregnancy is relatively small, the risk of serious maternal morbidity and mortality is high if they are untreated. Those involved in the interpretation and reporting of imaging studies should use clear and precise terminology to avoid misunderstandings that can negatively impact patient management. Clinicians involved in patient care must be aware of the limited ability of imaging modalities to unequivocally establish the diagnosis of interstitial pregnancy, especially in the presence of anatomic uterine abnormalities. 24
Ectopic pregnancies are particularly suited to laparoscopic management, because of their small volume and soft consistency, which allows for easy retrieval through laparoscopy ports. Use of endobags and morcellation permits retrieval of larger masses as well. As the development of postoperative adhesions is less than after laparotomy, fertility may be better preserved with laparoscopy.
Conclusions
It can be concluded that early diagnosis using newer ultrasound technologies and availability of surgical expertise can obviate the need for laparotomy, and facilitate successful management of even these rare and challenging varieties of “cornual” ectopic pregnancies by endoscopic procedures.
Footnotes
Disclosure Statement
No competing financial conflicts exist.