
Abstract
Abstract
Introduction
V
Case
A 45-year-old female, para 7, living 7, with tubal ligation performed 10 years ago, presented with complaints of a mass in her vagina since 1 year prior to presentation. She had no bowel or bladder complaints or sudden loss of weight or appetite. Her general condition was satisfactory. On examination, a 5×5 cm hard but tender swelling in the region of the left labial margin, free from the pubic ramus, was felt. No obvious ulceration was seen. The vaginal mucosa was intact. Her cervix appeared to be healthy and a Papanicolaou smear was performed, which came back from testing as normal. A vaginal examination showed a normal-size retroverted uterus and the bilateral adnexa were free. A rectal examination showed that rectal mucosa and parametrium were also free. All routine investigations yielded normal results. However, a transperineal ultrasound-guided (USG) scan revealed the presence of a 4.4×5.3×4 cm size, well-defined, hypoechoic focal lesion in the entire vagina extending up to the external surface of the vulva (Fig. 1). The cervix was not involved. The rectum appeared posterior to the hypoechoic focal lesion, separate from the lesion. The Bladder and urethra also appeared to be separate from the lesion (Fig. 2). An abdominopelvic USG scan showed a normal cervix, a uterus of 7.1×5.1×4.9 cm, and an endometrial thickness of 4 mm. The right and left ovaries were normal. There were no other significant findings. A computed tomography scan showed an enhanced, well-defined exophytic mass of 5.2×4.6×4.5 cm along the left lateral wall of the vagina, indenting the vagina. Anteriorly, the mass touched the left inferior pubic ramus, and posteriorly abutted the left half of the anterior wall of the rectum. The mass also laterally abutted the left obturator internus and superiorly reached the lower aspect of the left levator ani (Fig. 3). A biopsy of the mass showed an adenocarcinoma of the Bartholin's gland with perineural invasion (Fig. 4).
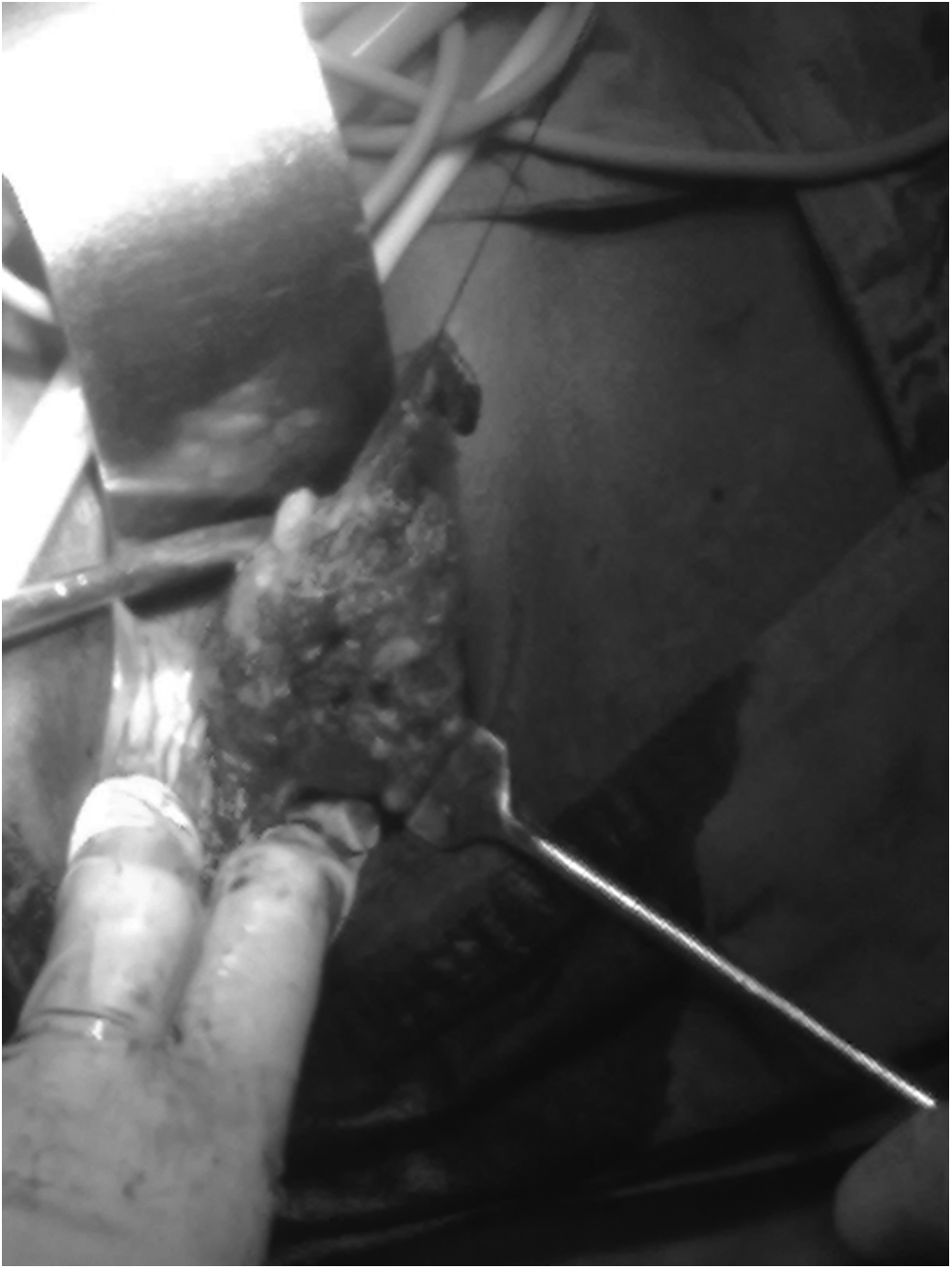
Bartholin's adenectomy being performed in the patient described in current case report.

Cavity after adenectomy to be filled with gracilis flap.
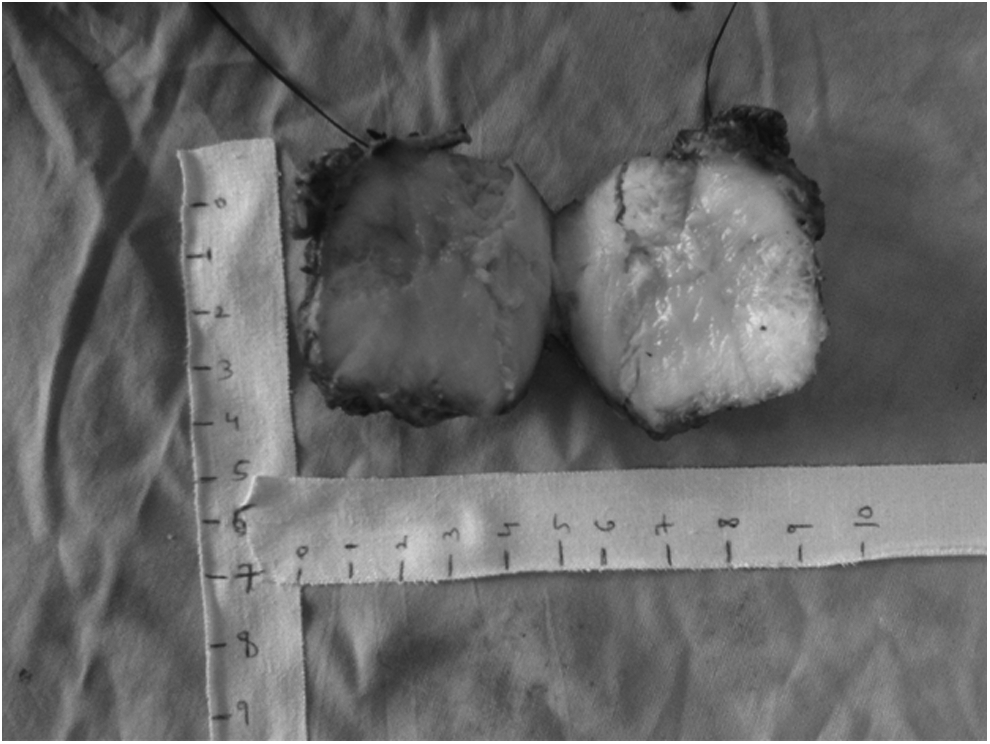
Cut specimen of Bartholin's gland adenocarcinoma.
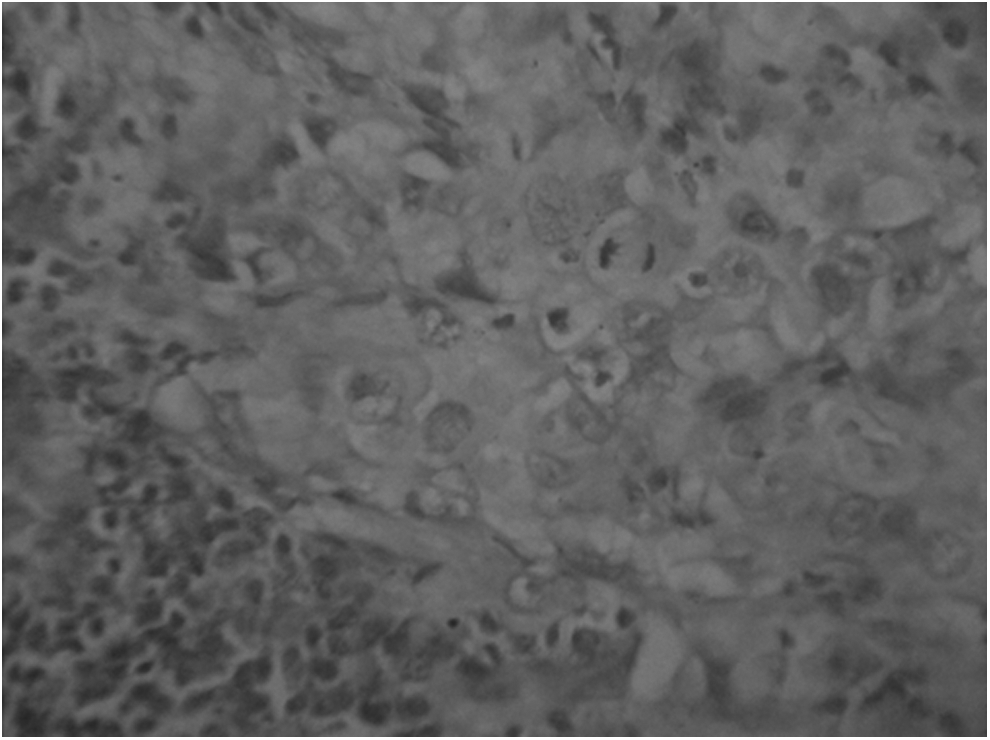
Photomicrograph of microscopic findings.
This patient underwent a left Bartholin's gland adenectomy with reconstruction (Fig. 5A). She was put in a lithotomy position. After excision, the left posterolateral defect was closed by a gracilis flap (Fig. 5B). HPR of the tumor showed an adenocarcinoma of the Bartholin's gland with perineural invasion. Inguinal lymphadenopathy was not tested according to standard treatment guidelines for microinvasive vulvar malignancy with no severe vulvar dystrophy. 2 The patient was advised to undergo immunohistochemistry testing of the mass from a private laboratory, as this kind of testing is not available in our hospital. However, the patient was unable to pay for private laboratory testing.

Results
This patient's postoperative course in ward was uneventful. Her wound was healthy, and she was discharged to go home. As of this writing, a follow-up is planned for scheduling radiotherapy.
Discussion
Surgery is the most common and useful treatment for a Bartholin's gland adenocarcinoma. 3 The treatment may range from a simple local excision to radical vulvectomy, with or without partial or complete regional lymphadenectomy. Radiation is a choice of treatment for patients with high risk factors after surgery, such as a positive surgical margin, deep local invasion and infiltration of perineural spaces, or recurrences without opportunities for excision.
This patient had a Bartholin's gland adenocarcinoma with perineural invasion, which caused pain at that site. Local excision of the tumor was performed, followed by a gracilis muscle graft to cover the defect. Radiotherapy of the bilateral inguinal lymph nodes is planned to address the perineural invasion noted on the biopsy.
Conclusions
Surgery is the mainstay treatment of Bartholin's gland adenocarcinoma with or without radiotherapy.
Footnotes
Acknowledgments
The authors thank the department of obstetrics and gynecology at the Grant Medical College & Sir J.J. Group of Hospitals, in Mumbai, India, for allowing the authors to be part of this organization, where this work was performed.
Disclosure Statement
The authors do not have any commercial associations that might create a conflict of interest in connection this article. Thus, no competing financial interests exist.