
Abstract
Abstract
Introduction
C
Gestational choriocarcinoma commonly occurs in the uterus. This cancer originates from placental trophoblastic cells of normal or abnormal pregnancies. Half of choriocarcinoma cases arise from hydatidiform moles, 25% from normal pregnancy, while the other cases arise from ectopic pregnancies or teratomas. 3 Choriocarcinoma presented as a Fallopian-tube mass is extremely rare and poses diagnostic challenges in women of reproductive-age.4,5 Production of ectopic β–human chorionic gonadotropin (β-hCG) by the tumor leads to a misdiagnosis of an ectopic pregnancy. Early diagnosis is the key for patients' survival. Choriocarcinoma can have a good prognosis even at an advanced stage. This is attributed to its chemosensitive nature. 6
Case
A 34-year-old para, 8+2 woman, presented with right iliac fossa pain for a duration of 1 day prior. Her last childbirth had occurred 2 years prior to this admission. Bilateral tubal ligation had been performed after that last delivery. She did not have any history of previous molar or ectopic pregnancies. Her current urine pregnancy test was positive; thus, she appeared to be pregnant again. Serial preoperative β-hCG level testing during admission showed a marked increase within 2 days (15,000–752,601 milli–international units/L [mIU/mL]). Ultrasonography (US) showed a left adnexal mass, but the uterine cavity was empty. Clinical diagnosis of an ectopic pregnancy was made. Intraoperatively, the left broad ligament and infundibulopelvic ligament were dilated and engorged. A left salpingectomy and wedge resection of the broad ligament were performed. Her postoperative β-hCG level was significantly reduced (225,000 mIU/mL).
She apparently had had symptoms of respiratory distress preoperatively; this was treated as influenzalike illness or atypical pneumonia. A chest radiograph was performed and showed bilateral basilar consolidation (Fig. 1).
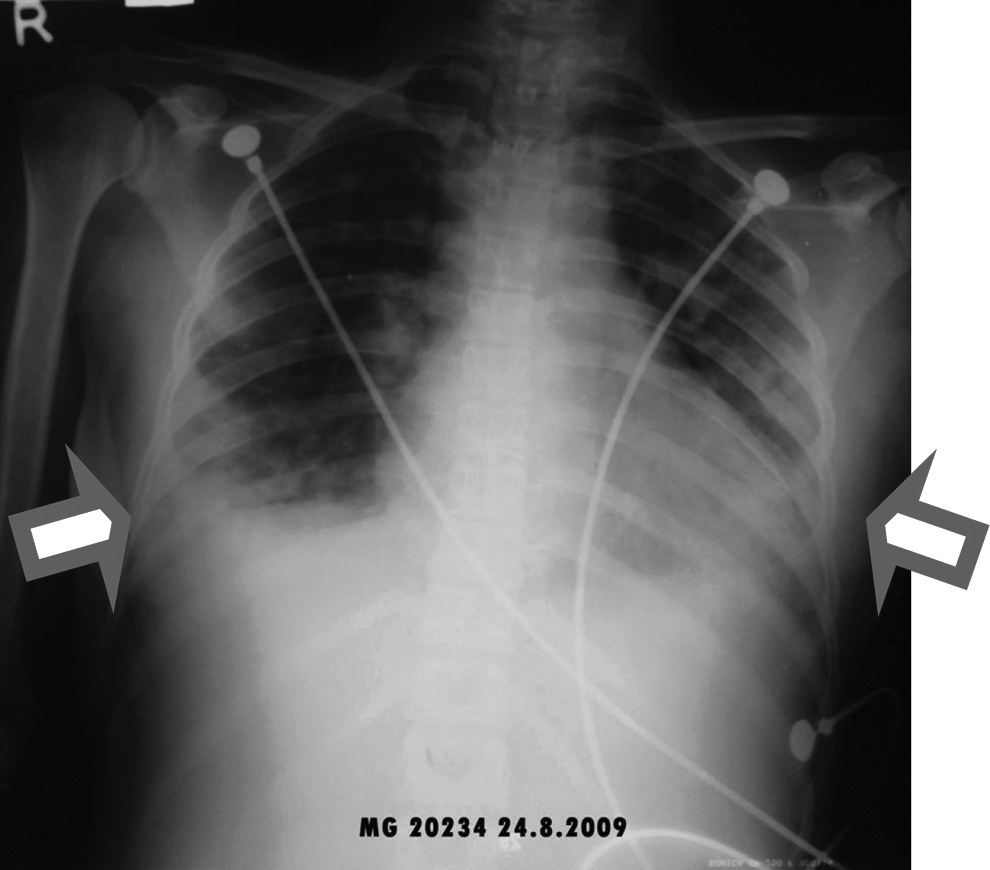
Chest X-ray showing choriocarcinoma (arrows).
Results
Clinically, she had significant improvement after the operation. She was recovering well in the ward until she developed sudden respiratory distress and collapsed on the ninth postoperative day, and she died.
A postmortem examination was performed to determine the cause of death. Pleural effusion with serous fluid was detected during autopsy. Both lungs had multiple nodular lesions (Fig. 2). There was no purulent exudate. The heart was normal, and other body systems were unremarkable.

Macroscopic features of choriocarcinoma, including nodular lesions (arrows).
Histologic examination of the earlier Fallopian-tube specimen and the nodular lung lesions revealed classical features of choriocarcinoma (Fig. 3). The malignant cells were positive for β-hCG immunohistochemistry.

Microscopic classical features of choriocarcinoma (arrows).
Discussion
Fallopian-tube choriocarcinoma may develop from a previously unrecognized tubal molar pregnancy or seeding from uterine conception. 7 According to the best knowledge of the current authors, only 40 cases of tubal ectopic hydatidiform mole have been reported. The risk of persistent trophoblastic disease is equivalent to the one seen in uterine molar pregnancy. Cases without previous molar pregnancy have also been reported in the literature. 7
A primary extrauterine choriocarcinoma has a prevalence of 1:5333 ovarian pregnancies and 1:2.2 million normal intrauterine pregnancies. 5 It is estimated that 75% of these patients have metastatic disease. 8 Other reported primary sites include the ovary, abdomen, and pelvis.4,5 Choriocarcinoma can develop as soon as 5 weeks after the antecedent gestation. Late presentation of choriocarcinoma has also been reported. It may occur up to 15 years after gestation and even after menopause. 9
Trophoblastic neoplasms generally produce excessive amounts of β-hCG, which is ∼3–100 times higher than the levels seen in normal pregnancies. Serial measurements of β-hCG levels with follow-ups after treatment are the most useful methods of diagnosis.9–11 In view of the high β-hCG level the current patient had, the suspicion of trophoblastic disease should have been considered.
A chest radiograph taken of a patient with metastatic choriocarcinoma causing choriocarcinoma syndrome may appear to show diffuse parenchymal infiltrates throughout the lung fields. However, typical metastatic nodules can be obscured by the opacity caused by diffuse pulmonary hemorrhage or pleural effusion. 12 The obscured tumor nodules may contribute to a misdiagnosis of pneumonia.
Diffuse alveolar hemorrhage (DAH) as a result of metastasis is rare, compared to immune-related DAH. In neoplastic cases, the findings are generally confined to haematologic malignancies and vascular tumors such as angiosarcomas. 1 This condition frequently leads to acute respiratory failure and death. 1 Metastatic choriocarcinoma cells are generally perfused by fragile blood vessels. The malignant cells have the capacity to erode blood vessels, which leads to life-threatening hemorrhage. 6 Intravascular tumor cells' embolization causes rapid elevation of pulmonary venous pressure and increases capillary-wall permeability. Intrapulmonary local depletion of platelets as a result of intravascular tumor emboli formation and tumor mass rupture also contributes to this complication. 1 The absence of hemosiderin-laden macrophages or organization reflects the short clinical course of the condition.
Conclusions
Chemotherapy is the mainstay treatment for choriocarcinoma. It has an ∼95% cure rate, even in patients with metastatic disease.9,13 The recommended management of primary extrauterine choriocarcinoma is complete surgical resection followed by chemotherapy. 5
Footnotes
Disclosure Statement
The authors declare no conflict of interest.