
Abstract
Abstract
Introduction
S
Case
A 57-year-old, postmenopausal woman presented with a 1-month history of a subjectively enlarging, nontender vulvar mass. She denied drainage from the mass, abnormal vaginal discharge, bleeding, or recent weight loss. She had undergone an excisional biopsy of a lesion at the same location nearly 10 years earlier, but was unaware of the diagnosis. Pathologic records were unavailable for review. Physical examination revealed a 3×3 cm well-circumscribed, solid, nontender, mobile mass attached to the left labium majus. No inguinal lymphadenopathy was appreciated. The surrounding perineal skin appeared normal. An excisional biopsy was performed with the patient under general anesthesia, and the mass was excised in its entirety.
Results
Gross pathology of the left vulvar mass showed two irregular fragments of pink-tan to yellow-tan fatty soft tissue measuring 4.4×2.9×1.1 cm and 2.4×1.8×1.2 cm. Histologic examination of the excised lesion revealed a cellular spindle-cell neoplasm with mild cytologic atypia and an infiltrative growth pattern (Fig. 1). The cells of the lesions showed ovoid to tapered nuclei with variable amounts of palely amphophilic cytoplasm and scattered mitotic figures (Fig. 2). Prominent blood vessels were evident within the stroma, many of which showed fibrinoid change and occasional luminal thrombosis (Fig. 3). Immunohistochemistry showed that the lesional cells were negative for Pan-Keratin, cluster of differentiation 34 (CD34), smooth-muscle actin (SMA), desmin, S-100 protein, and glial fibrillary acidic protein (GFAP). Based on these immunohistologic characteristics and the infiltrative growth pattern, the lesion was considered as an unclassified spindle-cell sarcoma (low-grade), and submitted for expert consultation. On the basis of this consultation, the histologic diagnosis was upheld. As the initial surgical resection was suboptimal, the patient underwent a left partial vulvectomy with no local or inguinal lymph node dissection. Adequate margins were achieved, and she subsequently had an uneventful postoperative recovery.
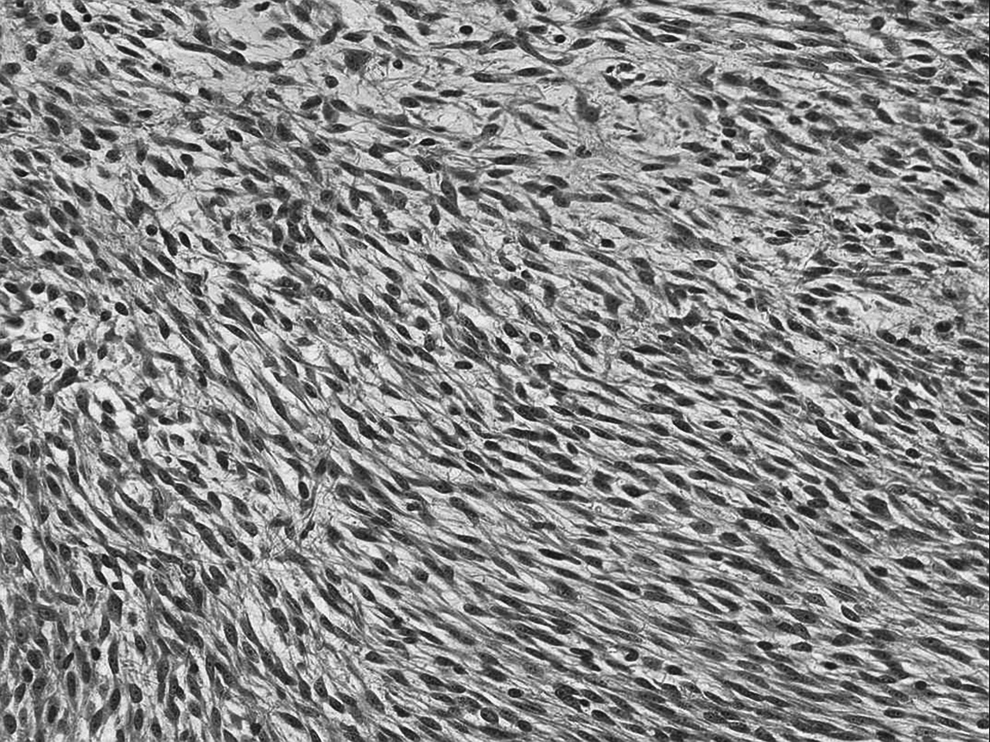
Photomicrograph of the low-grade spindle-cell sarcoma (20× magnification, hematoxylin and eosin stain). The lesion shows an infiltrative growth pattern, with nuclei that are ovoid-to-tapered, with mild atypia. Occasional mitotic figures are also present.
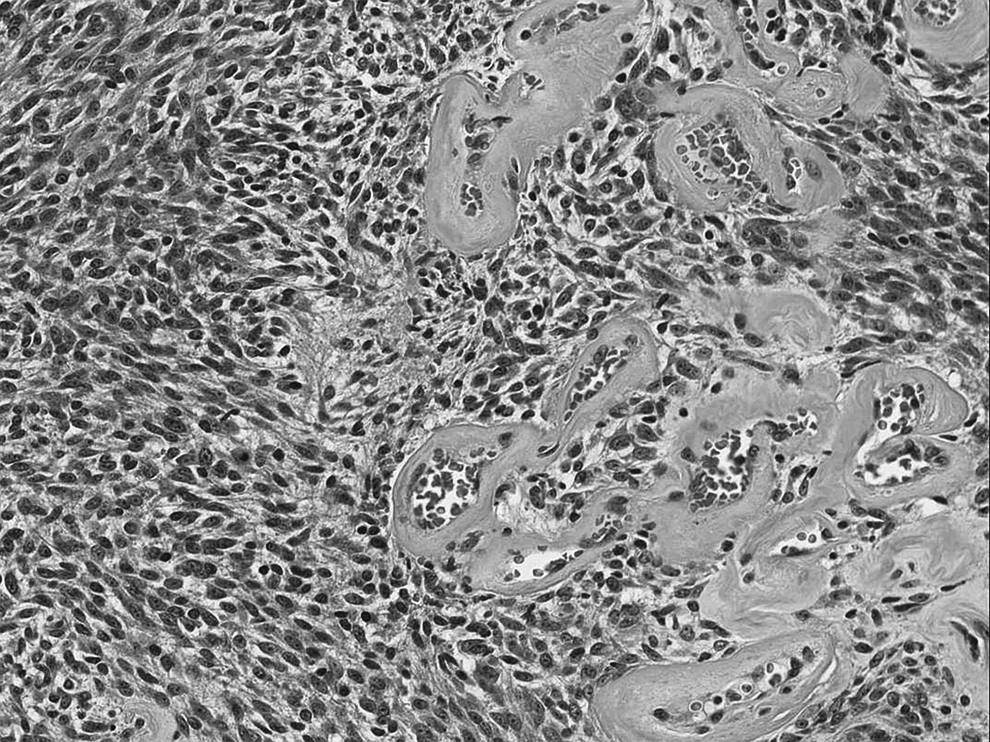
Photomicrograph showing prominent stromal blood vessels with fibrinoid changes and occasional mitotic figures (10× magnification, hematoxylin and eosin stain).
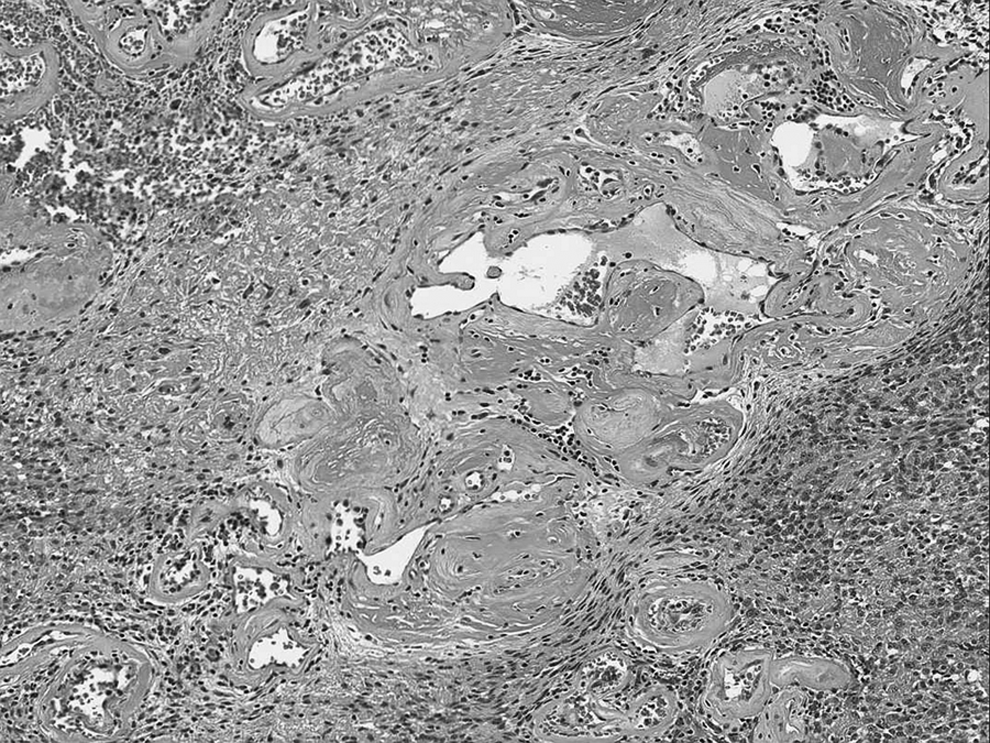
Photomicrograph showing stromal blood vessels with luminal thrombosis and fibrinoid changes within the vessel walls (20× magnification, hematoxylin and eosin stain).
Discussion
Primary soft-tissue sarcomas account for 1%–3% of all malignant tumors occurring in the female genital tract, and develop from mesenchymal tissue, including connective tissue, muscle, fat, and endothelium.1–4 Sarcomas of the vulva can occur over a wide age range, but are found most commonly in women in their fourth and fifth decades of life, with a median age of diagnosis at 50 years.3,5 These tumors typically present as subcutaneous lumps, which may be noticed by the patient or the examining physician. 5 Often, these lesions can be present for many years before patients experience symptoms such as vulvar pruritus, local discomfort, and pain during coitus.3,6 Vulvar sarcomas generally vary in size; however, lesions that are well-circumscribed and 3–5 cm in size are more likely to be benign, whereas those that are infiltrative and >5 cm are often malignant. 5
The most commonly encountered vulvar sarcomas include leiomyosarcomas, rhabdomyosarcomas, angiosarcomas, malignant fibrohistiocytomas, neurofibrosarcomas, and aggressive angiomyxomas. 3 Of these, vulvar leiomyosarcomas are the most common, constituting 1% of all vulvar malignancies.1,3,4,6 A broad differential diagnosis must be considered, particularly when the lesion in question is suspected of being a vulvar sarcoma. Several mesenchymal lesions may appear similar to sarcomas clinically; these belong to broad categories that include aggressive angiomyxoma-like lesions, fibrohistiocystic lesions, adipose-tissue lesions, smooth- and skeletal-muscle neoplasms, vascular neoplasms, and neural neoplasms (Box 1) 7 .
Surgical resection is the mainstay of therapy for vulvar sarcomas.2,3 Whereas patients with low-grade lesions may only require wide local excision to achieve local control, patients with high-grade lesions may need radiation or chemotherapy in addition to surgical excision.2–4 In a study of 11 patients with vulvar sarcomas, who underwent wide local excision with negative histologic margins, Behranwala and colleagues found that during a median follow-up period of 22 months, the median time to local recurrence, distant metastasis, and death in these patients was 37, 135, and 140 months, respectively. 4 These results indicate that vulvar sarcomas tend to recur following initial excision, and often show more worrisome histologic features during recurrence, necessitating long-term follow-up when possible. 5
Angiomyxoma-like lesions:
• Angiomyofibroblastoma • Superficial angiomyxoma • Cellular angiofibroma • Fibroepithelial polyp • Superficial myofibroblastoma
Fibrohistiocytic lesions:
• Fibroma • Dermatofibroma • Dermatofibrosarcoma protuberans • Malignant fibrous histiocytoma
Adipose-tissue lesions:
• Lipoma • Liposarcoma
Smooth-muscle neoplasms:
• Leiomyoma • Leiomyosarcoma • Leiomyomatosis
Skeletal-muscle neoplasms:
• Rhabdomyoma • Embryonal rhabdomyosarcoma
Vascular neoplasms:
• Angiokeratoma • Lymphangioma circumscriptum
Neural neoplasms:
• Neurofibroma • Granular-cell tumor
Analysis of this patient's case highlights two important features. First, the patient had developed a similar lesion in the past for which she underwent an excisional biopsy. Though the current authors remain unaware of this lesion's diagnosis, it would not be surprising to discover that the previous lesion was also a vulvar sarcoma. Consistent with the tendency of vulvar sarcomas to recur in spite of surgical excision, the current authors considered this lesion to be recurrent, likely because of inadequate resection or local invasion during the original surgery.4,5 Second, the patient's vulvar lesion was subjectively perceived to grow over a period of 1 month. Furthermore, our initial excisional biopsy had revealed nonnegative histologic margins. Following these findings and a detailed discussion with the patient regarding the short- and long-term morbidity associated with a definitive surgical procedure, the patient opted for a left partial vulvectomy without local or inguinal lymph-node dissection.
Conclusions
In addition to highlighting an extremely rare unclassified spindle-cell sarcoma of the vulva, this case emphasize the general approach necessary for diagnosing and managing vulvar lesions. Lesions of the vulva, particularly sarcomas, prove to be diagnostically challenging; hence, surgical excision and histopathologic evaluation are imperative to distinguish these lesions from other mesenchymal lesions of the vulva. Because of the relatively rare occurrence of vulvar sarcomas, and the limited number of cases with long-term follow up, the management of patients presenting with these tumors remains a challenge. Implementation of a multidisciplinary approach, including a pathologist with expertise in vulvar malignancies, as well as a surgeon experienced in vulvar surgery, is necessary for the long-term management and favorable prognosis of patients.3–6 As vulvar sarcomas tend to recur, long-term surveillance is necessary, although the overall length, frequency, and modality of surveillance still remains unknown.
Footnotes
Acknowledgments
The current authors thank Christopher Fletcher, MD, from the Dana-Farber Cancer Institute, Harvard Medical School, for the surgical pathology consultation.
Disclosure Statement
No competing financial interests exist.