
Abstract
Abstract
Introduction
C
CSP is often misdiagnosed as a cervical ectopic pregnancy, an incomplete abortion, or a lower intrauterine pregnancy. For instance, the diagnosis of CSP was missed in 13.6% of the reported cases. 11 This delay in the diagnosis and subsequent management can lead to potentially life-threatening complications.3,8,12,13 Moreover, the overall complications of different treatment regimens are reported to be as high as 44.1%. 11 This indicates the need for a management protocol with the lowest complication rate and the highest success rate. A review of the literature revealed that there is no standard protocol available for managing CSP. To contribute to the existing literature, the current authors present their experience with 2 cases of CSP who were treated successfully with two different management modalities.
Cases
Case 1
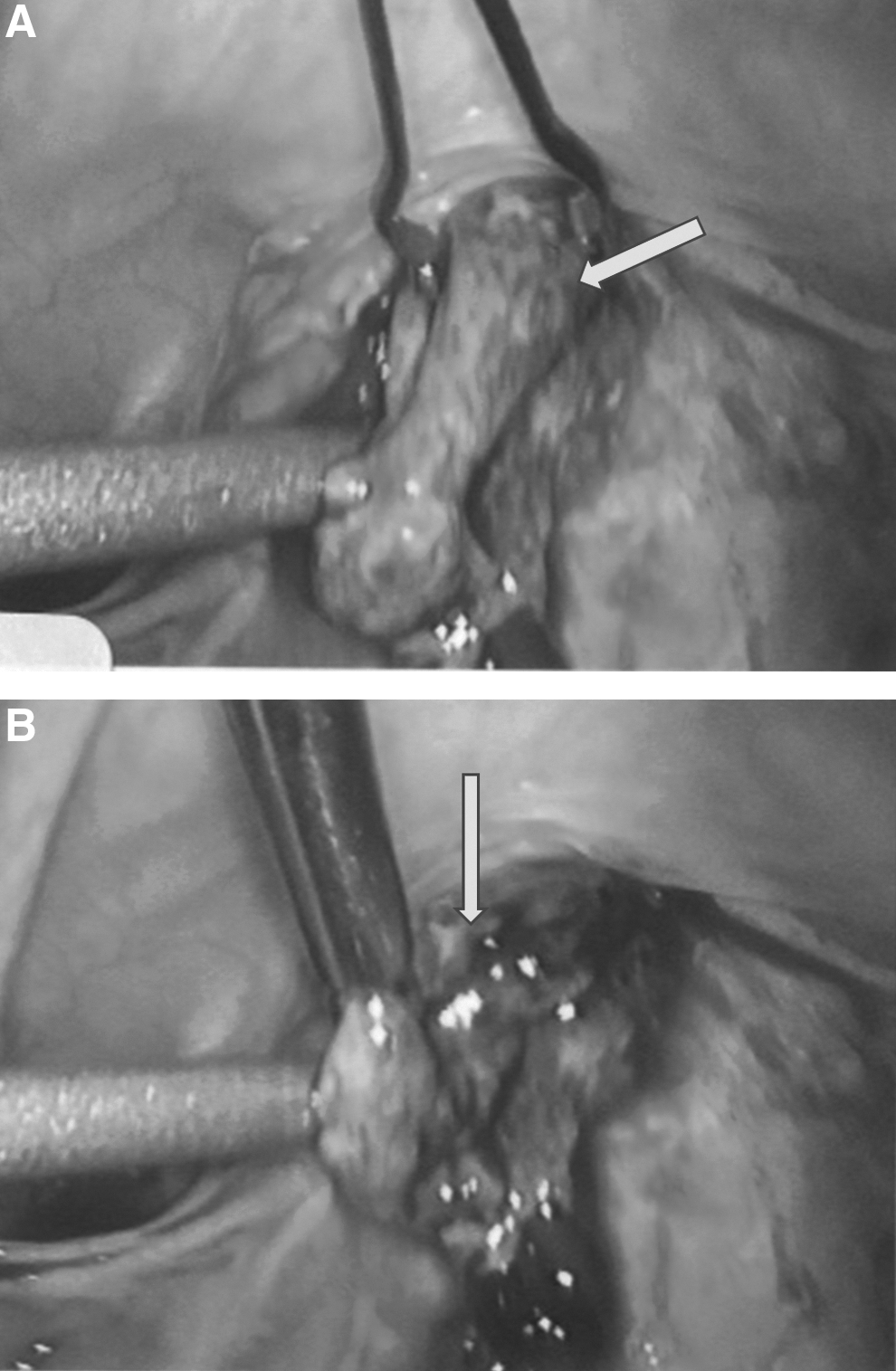
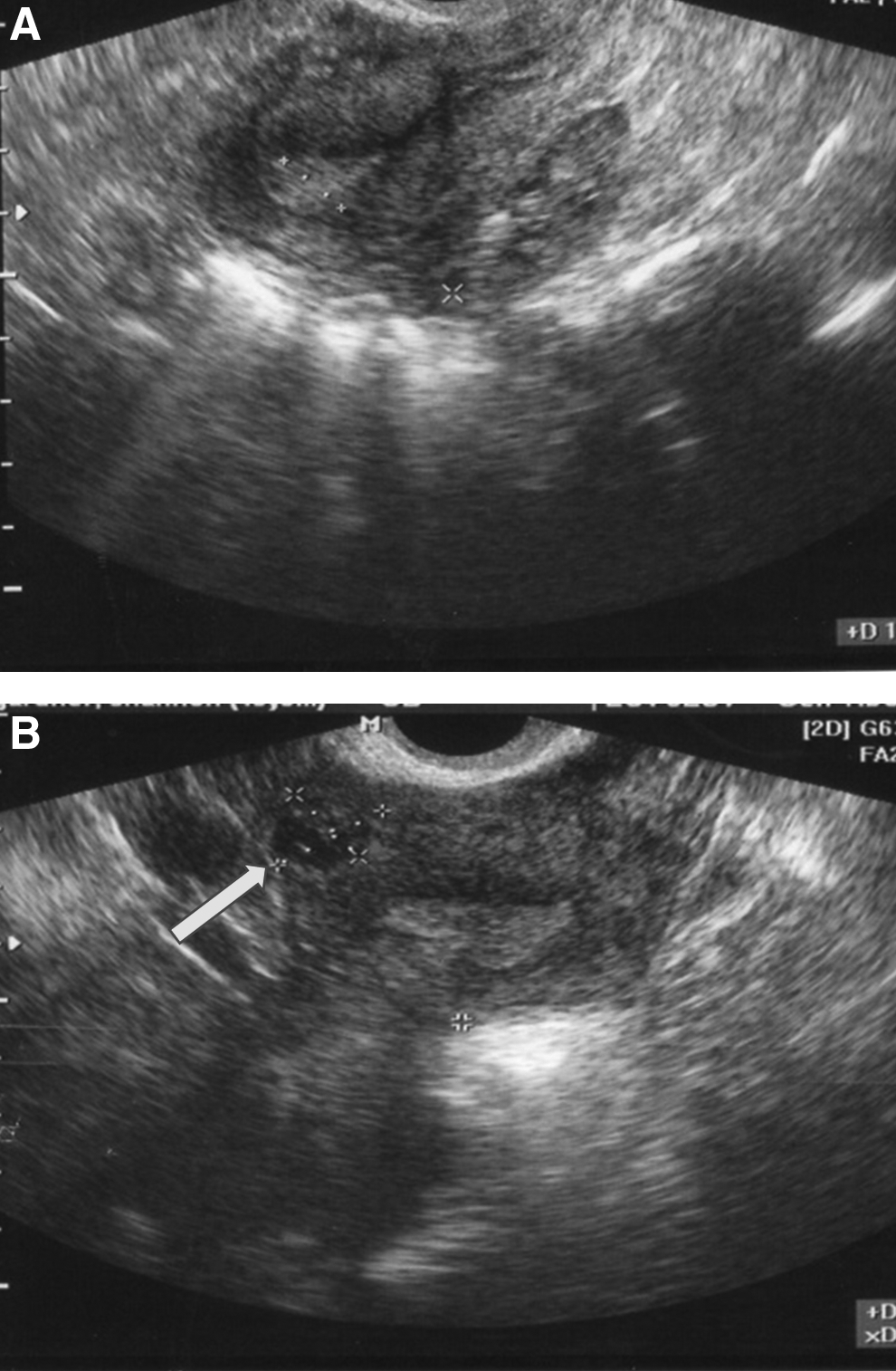
A 34-year-old Caucasian woman, gravida 2, para 1, presented for a routine obstetrical transvaginal ultrasound (TVUS) at 9-weeks of gestation. She had a positive home pregnancy test after missing a period a few weeks prior. Her pregnancy had been uneventful other than some mild spotting at the gestational age of 7 weeks for which the patient did not seek medical attention. She had a prior history of a low transverse cesarean section 1 year prior, which was performed after a failed induction of labor. The dating ultrasound showed a gestational sac in the cervical canal. A possibility of cervical ectopic pregnancy versus an incomplete abortion was considered. A quantitative assay of her level of ß-subunit of human chorionic gonadotrophin (ß-hCG) was 9084 mIU/mL. This ß-hCG 2 days later was 10328 mIU/mL. A second ultrasound (Fig. 1 A and B) showed a gestational sac with a yolk sac in the cervical canal, confirming the diagnosis of either a cervical ectopic pregnancy or a CSP. The patient was offered options of either undergoing a systemic injection of methotrexate or an aspiration of the pregnancy, followed by local injection of methotrexate. She chose the latter option. The next day, the patient underwent TVUS-guided aspiration of the gestational sac followed by a local injection of 77.5 mg (50 mg/m2) of methotrexate. She tolerated the procedure well and went home on the same day. TVUS scanning performed 1 week after treatment showed a collapse of the gestational sac (Fig. 2). Repeat testing of her levels of ß-hCG at days 4, 6, 7, 10, 13, and 17 after the procedure were 16911, 14420, 11502, 8653, 8196, 7426 mIU/mL, respectively. Plateauing of ß-hCG levels was observed. A repeat TVUS at that time showed reaccumulated fluid in the gestational sac with a yolk sac located in the CS scar (Fig. 3). The myometrium of the CS scar was very thin over the gestational sac (1 mm). The patient was advised that the best treatment option was to undergo surgery to prevent a possible rupture of the CSP. Diagnostic and operative laparoscopy with a possible laparotomy was arranged. During laparoscopy, it was observed that the bladder had adhered to the lower uterine segment over the prior CS scar (Fig. 4). A bladder flap was created carefully and the cesarean scar containing the pregnancy was exposed. Twenty mL of vasopressin was injected circumferentially in and around the pregnancy to ensure hemostasis. A small vertical incision was made over the pregnancy and the products of conception were removed, using forceps and scissors (Fig. 5 A and B). Four figure-8 stitches, using 2-0 Vicryl, were placed to close the uterine defect (Fig. 6). Diluted indigo carmine dye was injected through a Foley catheter to ensure that her bladder was intact. The patient recovered from the procedure well, and she was discharged to go home the same day. Her ß-hCG levels were normal after 1 month.
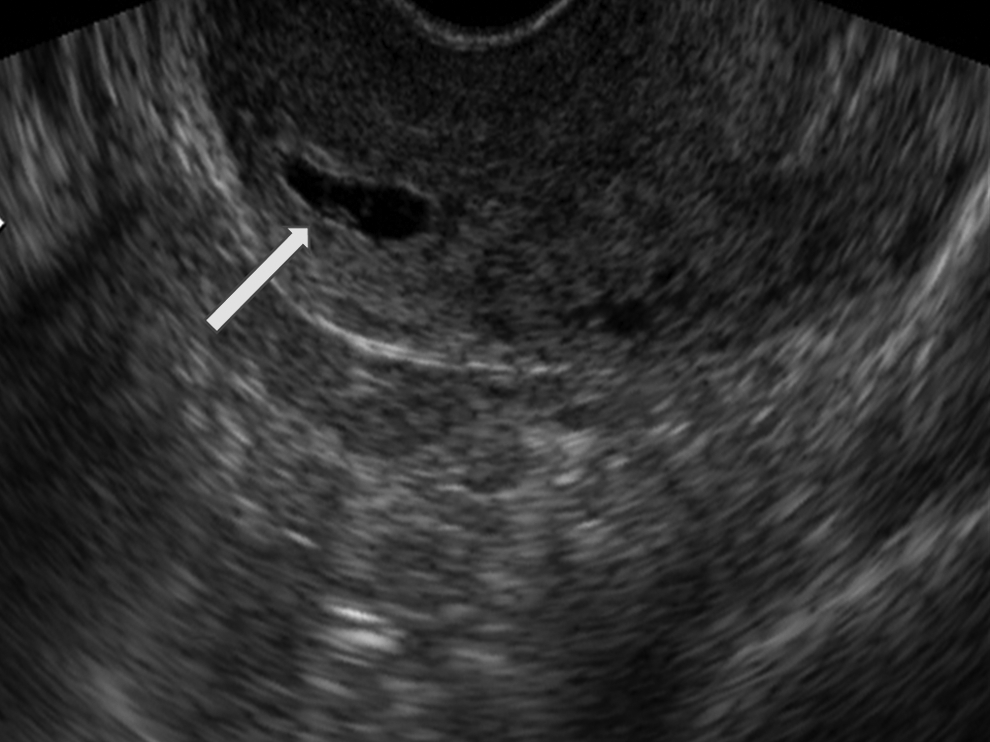
Two-dimensional transvaginal ultrasound (sagittal view). Gestational sac and yolk sac seen at the region of internal os (arrow).
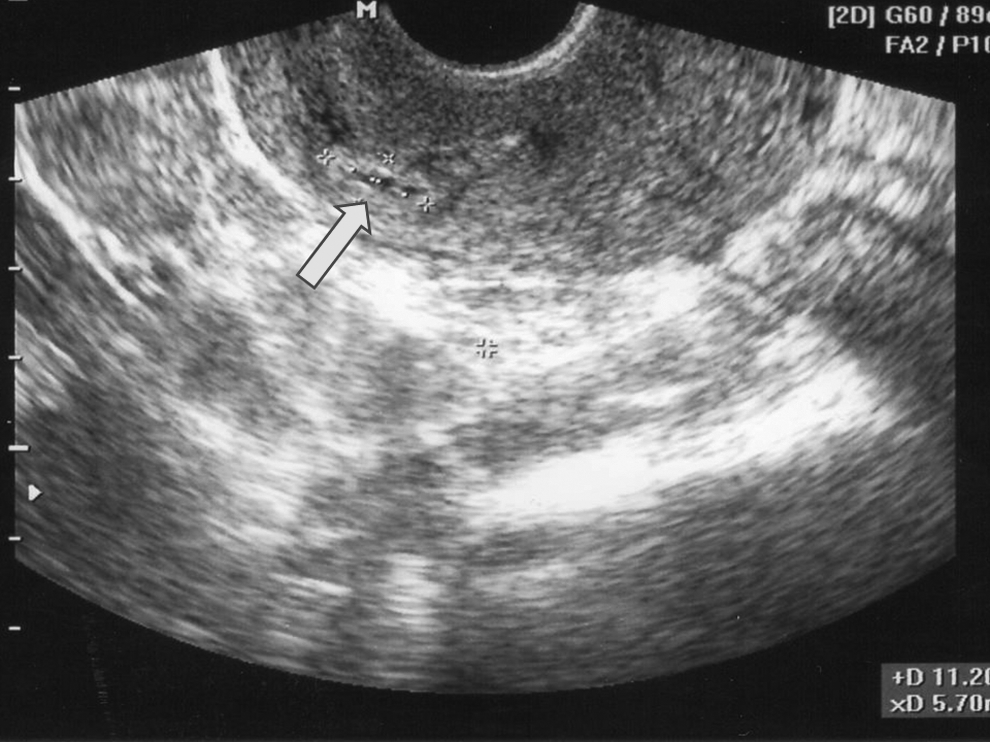
Two-dimensional transvaginal ultrasound (sagittal view): A collapsed gestational sac was noted (arrow) 1 week post aspiration and intragestational methotrexate.

Two-dimensional transvaginal ultrasound (sagittal view). Reaccumulation of fluid in the gestational sac and reappearance of yolk sac (arrow) at the region of the cesarean scar noted 2 weeks post aspiration and intragestational methotrexate.

Bladder adhered to the lower uterine segment over the prior cesarean section scar (arrow).
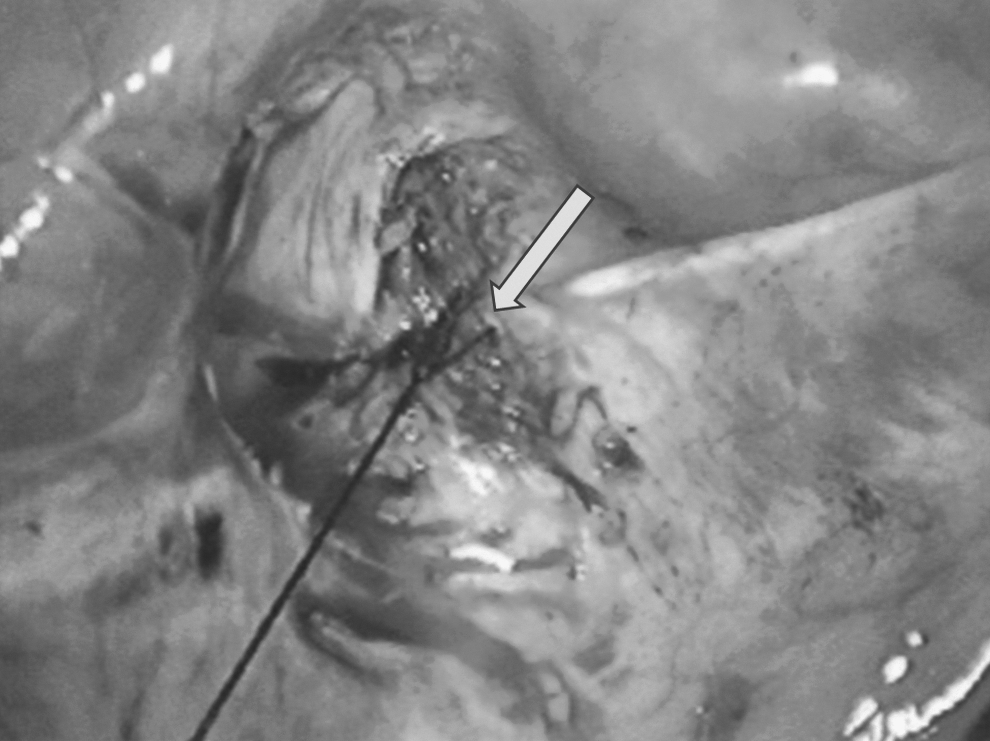
Closure of uterine defect (arrow).
Case 2
A 31-year-old Caucasian woman, gravida 3, para 1, achieved pregnancy via in-vitro fertilization frozen embryo transfer (IVF-FET) with an estrogen- and progesterone-stimulated cycle. Two blastocysts were transferred without any complications. This patient had a prior history of a successful IVF pregnancy (for male-factor infertility) that was delivered at term via a low transverse cesarean section 2.5 years ago. Her first quantitative ß-hCG level 2 weeks post IVF-FET was 246 mIU/mL. She had brownish spotting and mild cramping 15 days after the IVF-FET; this symptom subsided in 2 days. A repeat ß-HCG test in another 2 weeks showed a level of 310 mIU/mL. TVUS was performed, which showed a gestational sac in the cesarean scar with an otherwise normal uterine cavity. (Fig. 7 A and B). Only a small gestational sac and yolk sac were noted, but no fetal pole was seen. Various treatment modalities were discussed with the patient, and she chose systemic methotrexate therapy. She was given 113.5 mg (50 mg/m2) of methotrexate intramuscularly (IM) the next day. Post methotrexate, this patient started having vaginal bleeding for 6 days. Her ß-HCG levels on days 4 and 7 were 260 and 252 mIU/mL, respectively. A repeat TVUS on day 7 showed an empty uterus (Fig. 8A and B). However, a decision was made to administer a second dose of methotrexate secondary to her plateauing ß-HCG levels. She was given 113.5 mg (50 mg/m2) of methotrexate IM again. Her ß-HCG levels on days 4 and 7 were 83 and 51 mIU/mL, respectively. Her ß-HCG levels normalized within 1 month of administration of the first dose of methotrexate.

Results
The treatments (aspiration, methotrexate, and laparoscopic excision for Case 1, and methotrexate for Case 2) enabled resolution of the CSPs of these 2 patients.
Discussion
CSP represents a diagnostic and management dilemma. Delayed diagnosis and management can lead to life-threatening complications.3,8,11,13 The increasing rate of cesarean deliveries, a higher index of suspicion secondary to mounting awareness, and better diagnostic studies such as high-frequency TVUS can possibly explain the recent increase of cases described in the literature.3,5,14
Many management modalities have been described in the literature. In a review article, Timor-Tritsch et al. describe a combined modality with the lowest complication rate that was based on a review of literature and their own experience. 11 These researchers recommended local intragestational and systemic methotrexate therapy; this was reported to produce a complication rate as low as 5.3% in the cases that were treated. The downside of this treatment is a longer return to baseline and a lengthy follow-up, which is up to a minimum of 3 months. This might not be suitable for a noncompliant patient or one who will not be able to come back for frequent follow-up visits. In Case 1, a local injection of methotrexate and gestational sac aspiration resulted in plateauing of the patient's ß-hCG levels. Reaccumulation of fluid in the gestational sac and marked thinning of the ceserean scar predisposed the CSP to a high risk of impending rupture; hence, laparoscopic surgery was performed without any complications and a quick return of ß-hCG to baseline was observed.
Vial et al. 15 has described two distinct types of CSP: (1) Superficial implantation in the scar with progression of the pregnancy toward the uterine cavity; and (2) deeper implantation in a cesarean-scar defect with pregnancy progression outside the uterine cavity. One of the surgical treatments with the lowest complication rate described was hysteroscopic resection (14.7%). 11 A literature review showed that this modality might be one of the best available surgical managements for a CSP that projects inside the uterine cavity, because this approach can enable direct visualization of the vessels and subsequent coagulation, as the CSP is resected with a resectoscope.16–24 However, hysteroscopic resection might not be the best choice when the pregnancy is implanted deeper in the cesarean scar and tends to progress toward the bladder. In case 1, the TVUS revealed a very thin myometrium of 1–2 mm overlying the scar and a CSP in close proximity to the bladder. The decision was made to perform laparoscopy in order to dissect the bladder away from the CSP under direct visualization and hence reduce the risk of injury. This would have been very challenging if a hysteroscopic resection had been performed. This concept has also been supported by other researchers.10,25 However, it remains undisputed that both operative laparoscopy and hysteroscopy are heavily dependent on a surgeon's expertise. Systemic methotrexate is a modality with one of the highest complication rates (i.e., 62.1%). 11 The literature review also showed that, if ß-hCG was <5000 and the gestational age was <8 weeks, the chance of success was higher.3,5–7,26 In the experience of the current authors, Case 2 was diagnosed very early in her pregnancy secondary to close follow-up after her IVF-FET. She was treated with 2 doses of systemic methotrexate 1 week apart, which resulted in a prompt resolution without any complications (1 month).
Conclusions
An earlier diagnosis leads to a better outcome. Various treatment modalities have been described for managing CSP, with varied levels of success, but the optimal management and a standardized protocol remains to be determined. The goal of therapy should be preservation of fertility, reduction of life-threatening complications, and maintaining the patient's quality of life. In the current author's experience, when local injection of methotrexate in the gestational sac is not successful, laparoscopic removal of CSP is safe and effective. In the presence of low levels of β-hCG, treatment with systemic methotrexate is usually successful.
Footnotes
Acknowledgments
The authors would like to thank Cheryl Anderson, AAS, IVF, Michigan, P.C., for her assistance in the preparation of this article.
Disclosure Statement
Hina Javaid, MD, has no competing financial interests to disclose, nor does she have any commercial associations that might creat a conflict of interest to disclose.
Mostafa Abuzeid, MD, has no competing financial interests to disclose, nor does he have any commercial associations that might creat a conflict of interest to disclose.